Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.2018.v04i02.006
Year: 2018, Volume: 4, Issue: 2, Pages: 28-30
Case Report
S V Poflee1, S M Chawhan1, H S Bahirat1, S K Patil2
1Department of Pathology, Government Medical College, Nagpur, Maharashtra India,
2Department of Plastic Surgery, Government Medical College, Nagpur, Maharashtra, India
Address for correspondence:
Dr. Poflee SV, Department of Pathology, Government Medical College, Nagpur - 4400, Maharashtra, India.
Phone: +91-919822942472. E-mail: [email protected]
Folliculitis keloidalis nuchae (FKN), also known as acne keloidalis nuchae, represents a form of chronic scarring folliculitis. It is characterized by the formation of fibrotic papules and nodules over nape of the neck. The condition is seen mostly in men of African descent and less known in persons of another ethnicity. With persistence of the inciting factors, the condition recurs in most cases. The bulky recurrent lesion may mimic a tumor and is sampled with clinical suspicion of malignancy. A 34 years male of Asian origin presented with tumor-like swelling on posterior part of neck. The morphological diagnosis of FKN could be given only after correlation of the histological findings with the detailed clinical history of the patient. The case is reported for its rare occurrence in Indian men. Advanced lesions in the absence of relevant clinical data and paucity of Indian literature may pose difficulty in diagnosis.
KEY WORDS:Clinical presentation, folliculitis keloidalis nuchae, morphological diagnosis.
Folliculitis keloidalis nuchae (FKN) is a rare form of primary scarring alopecia.[1] The occurrence of the lesion finds mention mostly in men of African descent.[2] Recurrent lesions may result into the formation of ugly tumorous masses causing psychological morbidity to the patient and diagnostic difficulty for the unaware medical consultant. Histological findings are non-specific and need to be correlated with clinical course.
An excised specimen of a recurrent swelling over the posterior part of the neck from a 34-year-old male was received in surgical pathology section, with clinical suspicion of malignancy.
On gross examination, the specimen comprised multiple skin covered nodular tissue pieces of variable sizes, the largest being 7 cm × 2 cm × 2 cm. External surface of the nodules was uneven and revealed loss of hair, while tufted hair was on the larger nodule. Cut surface of all the nodules appeared firm white [Figure 1b and c]. Multiple sections were taken and stained with H and E stain.
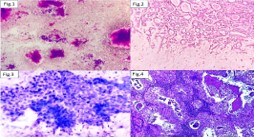
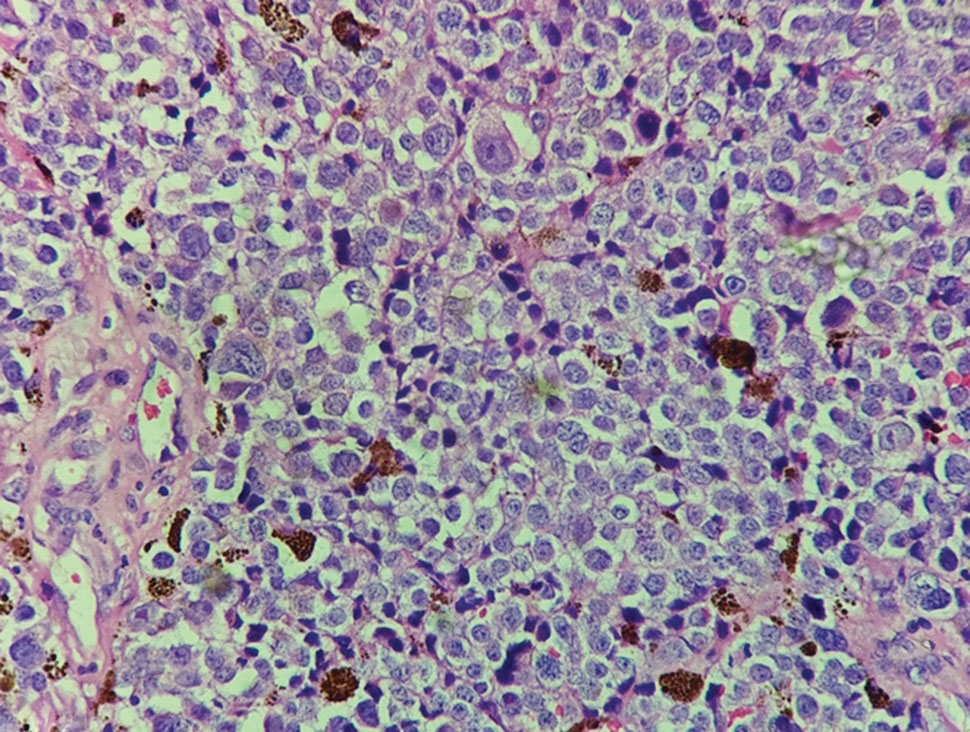
Microscopic examination revealed epidermis with focal ulceration. There was rupture and destruction of hair follicles with liberation of hair shafts into the dermis. Hair shafts were surrounded by chronic inflammatory infiltrate with prominent plasma cells, foreign body giant cell reaction, and focal microabscess formation [Figure 2a and inset]. In addition to pandermal inflammation, numerous bundles of sclerotic collagen were noted throughout the dermis. Special stain was done [Figure 2b and inset]. Sections from the deeper fibrofatty tissue showed congested blood vessels and sparse inflammatory infiltrate. Literature search was made to correlate the unusual gross and microscopic features.
The patient was approached to know the clinical course. He revealed that he noticed small nodules over nape of neck 8 years back. The nodules increased in size and formed a large swelling over next 2 years. There was intermittent purulent and bloody discharge from the swelling. The patient received antibiotics and intralesional steroid injections. With no significant symptomatic relief to the patient, the swelling was excised in 2011 at a private medical center. The patient did not have histopathological reports of the procedure.
Within 6 months of operation, the patient started developing pustules at the suture site that coalesced to form an elongated swelling and multiple small pustules laterally, over next 3 years. He received antibiotics, local ointments, and intralesional steroid injections with little relief. The central neck swelling showed rapid increase in size [Figure 1a]. With suspicion of malignancy, treating dermatologist referred the anxious patient to plastic surgery department of our tertiary care hospital. The swellings were excised with removal of deeper layer of skin and sent for histopathological examination.
The patient is a security person by occupation, a regular drinker, and seasonal smoker. He did not give a history of any major illness in the past nor similar swellings on other body sites.
His routine hematological investigations, liver and kidney function tests were normal. He was non- diabetic, non-hypertensive, and non-reactive to human immunodeficiency virus (HIV) I and II.
Taking into consideration, the clinical details of the patient, gross, and microscopic features final diagnosis of FKN were conveyed.
6 months after latest excision, the patient is symptom free and back to duty. Importance of avoiding trauma during shaving, combing, and maintenance of strict hygiene was explained to the patient. He has been advised yearly clinical follow-up.
FKN is a follicular-based disorder mainly affecting the nape of the neck. It is also known as acne keloidalis nuchae (AKN) and is primarily shown in men of African ancestry.[3] Historically, the entity was known by different terminologies before Bazin named the distinct entity as AKN in 1872. The term AKN is commonly used, though the condition is not keloid, the affected individuals do not have a tendency to develop keloids in other areas of the body, and the lesions do not have histological features suggestive of keloid.
The exact cause of FKN remains unknown. Contributory factors include trauma, chronic irritation, seborrhea, infection, genetics, and androgens.[2] Occurrence in renal transplant patient treated with cyclosporine is reported.[4] Verma and Wollina have suggested the condition to be a marker of metabolic syndrome.[5] Inflammation is central to the pathogenesis of the condition FKN shares some features with other forms of cicatricial alopecia and may occur together in the same individual.[6]
FKN is seen to occur in post-pubertal men and is rare after the age of 55 years. A few cases have been reported in females.[1]
Clinical presentation at the onset is characterized by the development of papules and/or pustules on the nuchal or occipital region. Pruritus, pain, and contact bleeding are common in active lesions. In severe or long-standing cases, the papules may coalesce into large, hairless fibrotic plaques, or nodules.[3,7] Tufted hairs may be present. In early stages, the non-specific clinical picture needs differentiation from other conditions.[8] FKN can be disfiguring and may adversely affect self-esteem of the person, like our patient.
The histopathology of FKN is variable and depends on the duration and activity of the lesion. The histology shows evidence of follicular and perifollicular inflammation with prominent plasma cells in early lesions. More advanced lesions reveal disrupted hair follicles, a foreign-body reaction, and subsequent dense dermal fibrosis and scarring. Findings are not pathognomonic. Perilesional and normal appearing skin may show evidence of low- grade chronic inflammation.[9,10]
Treatment for the early lesions includes topical and oral steroids and antibiotics. Surgical intervention is reserved for large fibrotic lesions. Targeted UV treatment is also advocated,[11] FKN remains therapeutically challenging and relapses are common.[3] There is an urgent need to encourage safe shaving habits to minimize the risk of acquiring blood-borne infections such as viral hepatitis and HIV among susceptible individuals.[2]

Delay in diagnosis of a rare condition like FKN can unnecessarily prolong the clinical course. Clinical awareness and timely treatment of FKN lesions at the onset are needed to prevent occurrence of unsightly lesions and avoidance of psychological morbidity to the patient.
What is new - advanced or recurrent lesions of FKN result into the formation of tumor-like masses that may be mistaken for malignancy on clinical grounds. Rare occurrence of FKN in persons of other ancestry may pose diagnostic dilemma to the uninitiated.
The authors would like to thank Dr. W.K. Raut, Professor and Head, Department of Pathology, GMC, Nagpur, and Dr. D.T. Kumbhalkar, Professor, Department of Pathology, GMC, Nagpur.
Subscribe now for latest articles and news.