Journal of Medical Sciences and Health
Year: 2023, Volume: 9, Issue: 2, Pages: 182-189
Original Article
Oisika Dutta1 , Anadi Roy Chowdhury2 , Niladri Sarkar3 , Suman Ghosh4
1 Junior Resident, Department of Pathology, Murshidabad Medical College & Hospital, Berhampore, 742101, West Bengal, India,
2Professor, Medical Superintendent cum Vice Principal, Murshidabad Medical College & Hospital, Berhampore, 742101, West Bengal, India,
3Associate Professor, Department of Surgery, Murshidabad Medical College & Hospital, Berhampore, 742101, West Bengal, India,
4Associate Professor and Head, Department of Pathology, Murshidabad Medical College & Hospital, Berhampore, 742101, West Bengal, India
Address for correspondence:
Suman Ghosh, Associate Professor and Head, Department of Pathology, Murshidabad Medical College & Hospital, Berhampore, 742101, West Bengal, India.
E-mail: [email protected]
Received Date:03 March 2023, Accepted Date:03 June 2023, Published Date:20 September 2023
Background: Breast carcinoma is the most common malignancy among women around the world. Core needle biopsy provides samples that are adequate in size thus allowing a histological diagnosis of breast carcinomas. CNB specimens can also be used for the immunohistochemical (IHC) assays of hormone receptors. Aims: To evaluate the concordance of ER, PR, HER2 Neu and Ki-67 in core needle biopsy and surgical specimens obtained by Modified radical mastectomy (MRM). Methods: A cross-sectional observational study was conducted in the Department of Pathology in association with the Department of Surgery at Murshidabad Medical College and Hospital for a duration of one and a half years. Patients undergoing Core needle biopsy of the breast who have been diagnosed with breast carcinoma on the basis of histopathology report and subsequently planned for MRM who have given consent for the study were included in this study. The samples were classified according to the immunohistochemical staining into four molecular subtypes: Luminal A, Luminal B, HER 2 Neu enriched, and triple-negative subtype depending on the expression of ER, PR, HER 2 Neu, and Ki-67. Result: The most common molecular subtype of breast carcinoma in both CNB and MRM specimens was the Triple-negative subtype. Conclusion: CNB has been found to be a reliable diagnostic tool that can help in determining Histopathological biomarkers for ER, PR positive, and HER2 Neu positive or negative tumors and it has also been found that retesting these markers again on the surgical specimens may not be necessary.
Keywords: Core needle biopsy, Breast carcinoma, Molecular subtyping, Immunohistochemistry
Breast cancer is the most common malignancy among women around the world. It has now overtaken lung cancer as the commonest cause of global cancer incidence in 2020, with an estimated 2.3 million new cases, which is about 11.7% of all cancer cases. In India, breast cancer is the most common cancer among women in many regions and has surpassed cervical cancer which, a decade ago was the most frequent cancer. 1
The Interest that has developed in novel prognostic markers is based on the fact that a considerable number of patients with early-stage breast cancer carry microscopic metastasis at the time of diagnosis. Most of the molecular markers that have been studied have both prognostic and predictive values. The Prognostic markers indicate aggressiveness, invasiveness, and the extent of the spread of tumors, and thus, they correlate with survival independent of the systemic therapy and can be used to select patients who are at risk. The predictive markers, on the other hand, are reports which allow clinicians to 2
Age, size of the tumor, histological type, histological grade, lymphovascular invasion, axillary lymph node (ALN) metastasis, and hormone receptor status (Estrogen receptor, Progesterone receptor, and Human epidermal growth factor receptor 2 (HER2 status) are traditionally considered as prognostic markers in patients with breast carcinoma. In the routine clinical management of patients with invasive breast carcinoma, the molecular markers — Estrogen receptor (ER), Progesterone receptor (PR), and HER 2 are used as predictive markers. An accurate assessment is essential and mandatory since all are targets and/or indicators of highly effective therapies against invasive breast cancer. 3
Determination of the Estrogen receptor (ER) status of breast carcinoma acts both as a prognostic and predictive factor and hence it has become a standard practice in the management of breast cancer. The positivity of ER provides prediction aimed at the response to endocrine therapy such as Anti-Estrogen (Tamoxifen) administration or ovarian suppression. Similarly, the positivity of Human epidermal growth factor receptor 2 (HER2) is beneficial for selecting targeted therapy with a monoclonal antibody (Trastuzumab) against HER2. 4
Prognostic and therapeutic information is provided by IHC–based classification of both ER/PR and HER2 status which cannot be achieved from either of them alone. Four distinct subtypes of morphologically similar breast cancers (Luminal A, Luminal B, HER2, and Basal-like) have been identified by Microarray profiling of invasive breast carcinoma. 4 The basal-like subtypes, which account for about 15% of the breast cancer cases and are ER, PR and HER2 negative, are associated with aggressive histology, poor prognosis, absent response to the usual endocrine therapies, shorter duration of survival, and BRCA1-related breast cancer. 4
HER 2 Neu which is a member of the Erb family plays an important role in the promotion of oncogenic transformation and growth of the tumor. About 25-30% of breast tumors over express HER 2 Neu protein and this contributes to poor clinical outcomes.5 Along with the treatment of metastatic disease, it has been found that the adjuvant treatment of primary HER 2 Neu breast carcinomas with Trastuzumab improves the outcome of the patients significantly. 5
Ki-67 is a proliferation marker, first described in 1983. It labeled the nuclei of proliferating non-neoplastic and neoplastic cells. For evaluating the disease aggressiveness, breast cancer proliferation is an important parameter and hence for taking therapeutic decisions, especially concerning chemotherapy. Ki-67 can be of clinical importance (if available and scored accurately) as a supplement to grade in determining prognosis and chemotherapy benefit. 6 The survival rates among patients with breast cancer can be increased by early diagnosis and by providing appropriate therapy. According to the recent treatment protocol Neoadjuvant chemotherapy (NACT) is given as initial management to all patients with locally advanced breast cancers which is then followed by surgery (MRM/ Breast conservative surgery). 7 What type of Neoadjuvant therapy is to be given, it depends upon the ER, PR and HER-2 Neu expression of the tumor cells and this influences the survival rates of the patients markedly.
Core needle biopsy (CNB) provides samples that are adequate in size giving a histological diagnosis, which in turn allows differentiation between in situ and invasive cancers. 8 For the immunohistochemical (IHC) assays of hormone receptors and other prognostic tumor markers, the CNB samples can also be utilized. Valuable prognostic information is provided by the ER, PR, HER2 Neu and Ki-67 status of these samples and thus the response of the tumor to neoadjuvant and adjuvant chemotherapy can be predicted. 9
The CNB specimen may be the only available pre-treatment tissue sample for assays of prognostic and predictive markers in some breast cancer patients, chiefly those patients who have been treated earlier with preoperative chemotherapy or neoadjuvant endocrine therapy. Cytotoxic chemotherapy may cause adequate tumor regression which can alter the histological, hormonal and proliferative markers. 10 Ablation of the tumor may completely alter the status of the prognostic markers, and IHC analysis of ER, PR, HER2 Neu expression, and the Ki-67 index may be equivalent to a molecular analysis by microarray. 10
To estimate the concordance of ER, PR, HER-2-Neu& Ki-67 between core needle biopsy and subsequent Modified Radical Mastectomy (MRM) specimens. To study the accuracy of CNB in the diagnosis of breast cancer.
A cross-sectional observational study was conducted in the Department of Pathology in association with the Department of Surgery, Murshidabad Medical College & Hospital for a duration of one and half years (December 2020 to June 2022). After obtaining ethical clearance from Institutional Ethics Committee and informed consent from the study population, the work was initiated.
Patients undergoing Core needle biopsy of the breast who have been diagnosed with breast carcinoma on the basis of histopathology report and subsequently planned for MRM who have given consent for the study. Exclusion criteria were women who were planning for MRM for having breast cancer but did not give consent. Patients whose CNB/surgical specimen receptor status was unavailable or remained unequivocal. All the tissue samples were collected in a 10% buffered formalin, and then they were processed for the routine histopathological examination. From formalin-fixed paraffin-embedded blocks, five micrometers thick sections were cut and stained with hematoxylin and eosin for histopathological diagnosis, and then immunohistochemical (IHC) staining was done for the expression of ER, PR, H2Neu, and Ki-67. According to IHC staining, the specimens were classified into four molecular subtypes: Luminal A, Luminal B, HER2Neu enriched, and Triple negative and then it was corroborated with molecular subtypes and clinicopathologic parameters.
Laboratory investigation and parameters included history taking, Gross morphology, Tumor size, Histological type, Nottingham combined histologic grade, Lymphovascular invasion, Lymph nodal status, Distant metastasis, ER expression, PR expression, Her2Neu expression, Ki-67 expression.
A core needle biopsy was obtained through the BARD 16G disposable needle under local anesthesia. The sample was put in formalin for HPE analysis and IHC study. The patient felt absolutely no pain after the procedure as it was done completely under local anesthesia. The post-procedure oral antibiotic was given along with an analgesic and a mild dressing on the wound. 5
The CNB specimens were subjected to thorough Histopathological examination and an IHC study for ER, PR, HER 2 Neu, and Ki-67. It was assigned a molecular type according to St. Gallen International Consensus Conference. Subsequently, patients were followed up and planned MRM who had given consent for the study.
About three micrometers thick sections from formalin-fixed paraffin-embedded tissues were cut for IHC staining. Positive Estrogen and Progesterone receptors show strong brown staining of the nuclei. For reporting the results of HER2 testing, the Allred scoring system for hormone receptors along with ASCO-issued recommendations was used.11 Grading of IHC staining for HER2/neu overexpression 12 : -Negative (Score 0) -No staining observed or membrane stating that is incomplete and is faint/barely perceptible and within ≤10% of tumor cells. Negative (Score 1+) -Incomplete membrane staining that is faint/barely perceptible and within >10% of tumor cells. Equivocal (Score 2+)- Weak to moderate complete membrane staining in >10% of tumor cells or Complete membrane staining that is intense but within ≤10% of tumor cells. Positive (Score 3+) -Complete membrane staining that is intense and >10% of tumor cells. Both weakly positive and strongly positive cases were considered to be positive.
For Ki67 positivity, a minimum of 1000 cells in at least 10 high-power fields per section were counted and expressed as a percentage. Cells that showed distinctive brown staining of nuclei and nucleoli were counted as positive cells and sections which showed >30% were counted as ki67 positive cases.5 In our study, we had two raters (also known as “judges” or “observers”) for CNB and MRM samples. The raters were responsible for measuring a variable on a categorical scale.
All data were thoroughly maintained on a Microsoft excel worksheet. For descriptive purposes mean ± SD, range and percentage were used. The concordance between core needle biopsy and surgical specimens (MRM) was analyzed by determining Cohen’s Kappa coefficient using the kappa (k) test of concordance. Concordances of 0.01 – 0.20, 0.21 – 0.40, 0.41 – 0.60, 0.61 – 0.80, 0.81 – 1.00 and 1.00 were defined as Slight, fair, moderate, substantial, almost perfect, and perfect, respectively.
The CNB specimens were subjected to thorough histopathological examination and an IHC study of ER, PR, HER2 Neu, and Ki-67 was assigned a molecular type. Subsequently, the patients were followed up. The MRM specimens of the same patients were subjected to Histopathological examination and an IHC study. After data accumulation, they were analyzed and the following results were obtained
The age of the patients ranged from 21 to 80 years with the Median age being 51.45 years. In the age group of 41-60 years (20 cases) breast carcinoma was most commonly found followed by 61-80 years (5 cases) and 21-40 years (4 cases). All the patients were females. Among all the patients, 13 cases involved the right breast, and 16 cases involved the left breast. So, apparently, the involvement of the left breast is slightly higher than that of the right breast (55% vs 45%).
Tumors with different sizes were observed starting from 10 mm to 110 mm. The T2 group had maximum tumor masses (17, 59%) followed by T3 (9, 31%), T4 (2, 7%), and T1 (1, 3%).
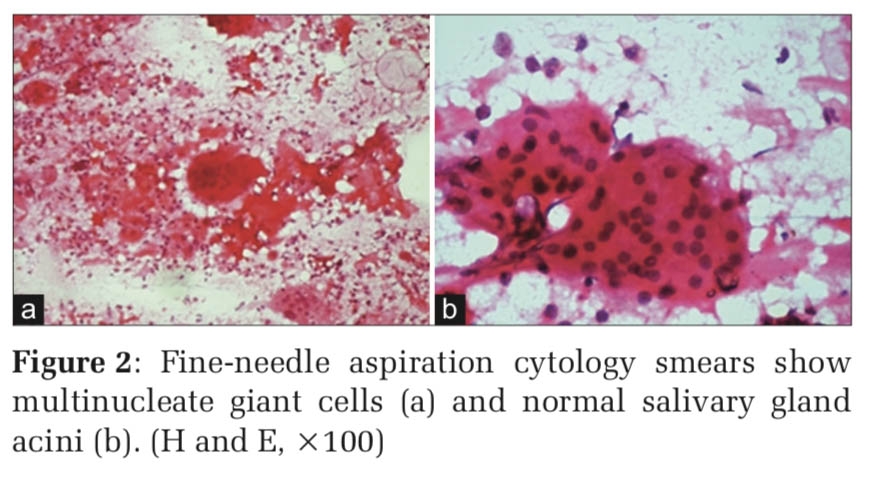
Most of the patients were suffering from infiltrating ductal carcinoma of No special type (IDC NST) [Figure 1]. Among the 29 patients, 27 were suffering from IDC NST (94%) followed by Mucinous breast carcinoma and Medullary carcinoma (each 1 case). Histological grading was done on all the specimens (MBR grading). Among the 29 patients, 19 patients had Grade 2 tumors (66 %), 8 had Grade 3 tumors (27 %) [Figure 3] and 2 had Grade 1 tumors (7 %). Lymphovascular invasion (LVSI) was present in 79% (23 cases). Axillary lymph node involvement was present in 69% (20 cases) of tumors and 31 % (9 cases) did not have lymph node involvement. [Figure 2]



Subsequently, an IHC study (ER, PR, HER2 Neu, and Ki67) was done on all the cases, both in core needle biopsies and MRM specimens and were classified accordingly [Table 1, Table 2].
|
Molecular subtypes (IHC defined) |
No. of cases in CNB (%) |
No. of cases in MRM (%) |
|
Luminal A |
4 (14%) |
6 (21%) |
|
Luminal B |
7 (24%) |
5 (17%) |
|
H2N Enriched |
4 (14%) |
2 (7%) |
|
Triple Negative |
13 (45%) |
13 (45%) |
|
Triple Positive |
1 (3%) |
3 (10%) |
Total number of cases =29, Molecular subtyping of Women undergoing Core needle biopsy (CNB) of the breast and diagnosed with breast carcinoma on the basis of histopathology report and subsequently planned for Modified Radical Mastectomy (MRM).
|
|
|
ER POSITIVE (MRM) |
ER NEGATIVE (MRM) |
Cohen’s K value |
|
CNB |
ER POSITIVE (CNB) |
12 |
0 |
0.86 |
|
ER NEGATIVE (CNB) |
2 |
15 |
||
|
|
|
PR POSITIVE (MRM) |
PR NEGATIVE (MRM) |
Cohen’s K Value |
|
CNB |
PR POSITIVE (CNB) |
5 |
0 |
0.63 |
|
PR NEGATIVE (CNB) |
4 |
20 |
||
|
|
|
H2N POSITIVE (MRM) |
H2N NEGATIVE (MRM) |
Cohen’s K value |
|
CNB |
H2N POSITIVE (CNB) |
2 |
3 |
0.28 |
|
H2N NEGATIVE (CNB) |
3 |
21 |
||
|
|
|
Ki-67 <= 30% (MRM) |
Ki-67 > 30% (MRM) |
Cohen’s K Value |
|
CNB |
Ki-67 <=30% (CNB) |
11 |
3 |
0.72 |
|
Ki-67 > 30% (CNB) |
1 |
14 |
For CNB, maximum cases (13,45%) were triple negative subtype (ER, PR, HER 2 Neu negative) followed by Luminal B subtype (ER-positive, HER 2 Neu negative, PR negative or Ki67 high) (7 cases, 24%), Luminal A subtype (ER positive, PR positive, HER 2 Neu negative, Ki67 low) and HER 2 Neu enriched subtype (ER negative, PR negative, HER2 Neu positive) had both 4 cases each, 14% each, and Triple positive subtype (ER positive, PR positive, HER2 Neu positive) (1 case, 3%). [Table 1 , Figure 4]

For MRM, maximum cases (13, 45%) were Triple-negative subtype (ER, PR HER2 Neu negative) followed by the Luminal A subtype (ER positive, PR positive, HER 2 Neu negative, Ki67 low) (6 cases, 21%), Luminal B subtype (ER-positive, HER2 Neu negative, PR negative or Ki67 high) (5 cases, 17%), Triple positive subtype (ER positive, PR positive, HER2 Neu positive) (3 cases, 7%) and HER 2 Neu enriched subtype (ER negative, PR negative, HER2 Neu positive) (2 cases, 10%). [Table 1]
The concordance between core needle biopsy and surgical specimens was almost perfect, 93.10 % (k=0.86) for ER, substantial, 86.20 % (k= 0.63) for PR, fair, 79.31% (k= 0.28) for HER 2 Neu and substantial 86.20% (k= 0.72) for Ki-67. [Table 2]
The importance of a correct preoperative evaluation of the proliferative activity and immunohistochemical marker status of the tumor has been increased by the use of Neoadjuvant chemotherapy for locally advanced tumors. 13
In our study, a total of 29 patients were included (all females). The age range was 21 – 80 years. The most common age group affected was 41-60 years (69%) followed by 61-80 years (17%). A. Khemka et al. found that the peak incidence of breast carcinoma was between 40-44 years. 14 Our study is also almost supportive of it. As per the data from Breast Cancer India (BCI), the average age of developing breast cancer has faced a significant shift in the last few decades; patients in the age group of 25 to 40 years of age have increased drastically. Of the 29 patients, 16 patients had breast carcinoma involving the left breast (55 %). A study by Aljarrah et al. stated that both breasts are almost equally involved in breast carcinoma. 15 So, our finding more or less correlates with them.
In our study, in the MRM specimens, we found tumors of different sizes starting from 10 mm to 110 mm. Most of the patients had Tumors in the T2 stage (17 patients, 59%) followed by T3 (31 %), then T4 (7 %), and T1 (3 %). In a study conducted by Zubair Ahmed et al., about 44.16% of patients had tumors in the T2 stage which was similar to our study. 16 The survival decreases with increasing tumor size have been found in numerous studies and also there is a coincidental rise in the frequency of axillary nodal metastasis. 16, 17
From the CNB and MRM specimens of 29 patients, we found that 27 patients were suffering from IDC NST (94%) followed by Mucinous and Medullary breast carcinoma (3 % each), which is in accordance with the study of Eheman CR et al. 18
In our study, 66 % of tumors (19 cases) were of Grade 2 (MBR Grading). Another latest Indian study conducted by Ravi Kumar et al. found 67.5% of Grade 2 breast carcinoma in their study. 19
On IHC studies in CNB specimens, 13 patients (45%) had a Triple-negative subtype of breast carcinoma which was followed by the Luminal B subtype (24%), thereafter Luminal A and HER 2 Neu enriched subtype (each 14%) and Triple positive subtype (3%). [Table 1]
In MRM specimens, 13 patients of 29 (45 %) had a Triple-negative subtype of Breast carcinoma followed by Luminal A subtype (21 %), Luminal B subtype (17%), Triple positive subtype (10%) and HER 2Neu enriched subtype (7 %) [Table 1]. The incidence of the triple-negative subtype was 30 % in a study conducted by Kim et al. on 776 consecutive cases of breast carcinoma which is not in accordance with our study. 20
About the hormone receptor status in CNB specimens, ER was positive in 41% of cases, and PR and HER2 Neu were positive in 17% of cases each.
In the MRM specimens, ER, PR, and HER 2 Neu were positive in 48%, 31%, and 17 % of the cases respectively. Pu X et al. found 35.4 % of ER-positive tumors in their study. 21
Coming to the Concordance rates, ER CNB and ER MRM had an almost perfect agreement, PR CNB, and PR MRM had a substantial agreement, HER 2 Neu CNB, and HER 2 Neu MRM had a fair agreement and Ki-67 CNB and Ki-67 MRM had a substantial agreement. [Table 2]
Ricci MD et al. in their study conducted on 69 breast cancer patients found almost perfect concordance for ER (k = 0.89), a substantial concordance for PR (k = 0.70), HER2 (k = 0.61) and Ki-67 (k = 0.74) obtained which is more or less similar to our study. 22
Aravind Barathi Asogan et al. conducted a study on 560 breast cancer patients and concluded that the concordance of CNB is high with surgical specimens in the evaluation of the molecular profile of invasive breast cancer. Therefore, it is not necessary to repeat the molecular evaluation with surgical specimens except for those cases where ER, PR, and HER2/neu are negative in the CNB samples. 23 In our study also, we found almost perfect substantial agreement between CNB and Surgical specimens indicating that CNB is accurate for early diagnosis of invasive breast carcinoma. 3 cases that were positive for her2/neu on CNB turned out to be negative on MRM. This may be due to the alteration of Her-2/neu receptor status following neoadjuvant chemotherapy in locally advanced breast cancer. Chemotherapy resulted in an alteration in Her-2/neu status from the core biopsy to the treated resected tumor. A similar study conducted by Ramteke P et al. showed alteration in steroid hormone and Her-2/neu receptor status following neoadjuvant chemotherapy in locally advanced breast cancer. 24 . One case that showed more than 30% positivity for ki67 on CNB shows less than 30% positivity on MRM was possibly due to the effect of Neoadjuvant chemotherapy received by the patient.
Ming Liu et al. in their study found that the concordance for HER2 was the poorest (κ=0.178) among the four markers. Our study also HER2 had the least agreement. 25
Xiaosong Chen et al. analyzed 298 invasive breast cancer patients and found the concordance rates for ER, PR, and HER2 were 93.6%, 85.9%, and 96.3%, respectively. The expression of Ki-67 was slightly higher in surgical specimens than in CNB samples (29.3% vs. 26.8%). So, they concluded that CNB was accurate in determining ER, PR, and HER2 status as well as non-luminal molecular subtypes in invasive breast cancer. 26
Limitations: The sample size was very small, comprising 29 cases. Larger population-based studies are needed to avoid this selection bias. The standard methods for assessing the status of HER 2 Neu is by FISH or CISH but in our study, the status of HER 2 Neu was assessed by IHC.
From our study, CNB has been found to be a reliable diagnostic tool that can help in determining Histopathological biomarkers for ER, PR positive, and HER2 Neu positive or negative tumors and it has also been found that retesting these markers again on the surgical specimens may not be necessary. The most common Molecular subtype of the CNB specimens was the Triple-negative subtype followed by Luminal B whereas, in the case of the MRM specimens, Triple negative subtype was the most common subtype followed by the Luminal A subtype. The marker status of the tumor is accurately reflected in the immunohistochemical assays of ER, PR, HER 2 Neu and Ki-67 in CNB samples. The concordance rates for HER2 Neu were less consistent as compared to the concordances for ER, PR, and Ki-67.
None
The authors do not have any conflicts of interest to declare.
Subscribe now for latest articles and news.