Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.2018.v04i03.006
Year: 2018, Volume: 4, Issue: 3, Pages: 29-30
Case Report
Shruthi Neelakanth Shetageri, S R Raja Parthiban, L R Karthik, A Mohamed Hamza
Department of Pathology, MVJ Medical College and Research Hospital, Hoskote, Karnataka, India
Address for correspondence:
Dr. Shruthi Neelakanth Shetageri, Department of Pathology, MVJ Medical College and Research Hospital, Hoskote, Karnataka, India. Phone: +91-8277209401/8217592179. E-mail: [email protected]
Liesegang rings (LRs) are benign and concentric non-cellular lamellar structures, occasionally found in kidney, synovium, conjunctiva, and eyelid. They are uncommon pathological findings which may cause diagnostic dilemmas for pathologists. We report a rare case of a 40-year-old female patient presenting with the left-sided lumbar pain, burning micturition, and hematuria for 1 week. With the radiological impression of a renal tumor, she underwent left radical nephrectomy. A diagnosis of clear cell renal cell carcinoma, the WHO/ISUP Grade II, and a stage of pT2aNxMx was made. An additional feature noted was the presence of LRs at the periphery of the tumor. It is important to recognize these rings to avoid mistaking them with parasites and dystrophic calcification. Hence, awareness among pathologists about these lesions would help in the proper management of the patients.
KEY WORDS:Clear cell renal cell carcinoma, kidney, Liesegang rings.
Liesegang rings (LRs) are benign and concentric non-cellular lamellar structures, occasionally found in kidney, synovium, conjunctiva, and eyelid.[1] They occur as a consequence of the accumulation of insoluble products in a colloidal matrix.[2] LRs are uncommon pathological findings which may cause diagnostic dilemmas for pathologists. LRs are known to occur in a variety of lesions; we present a rare incidental finding of LRs in a case of clear cell renal cell carcinoma (CC-RCC).
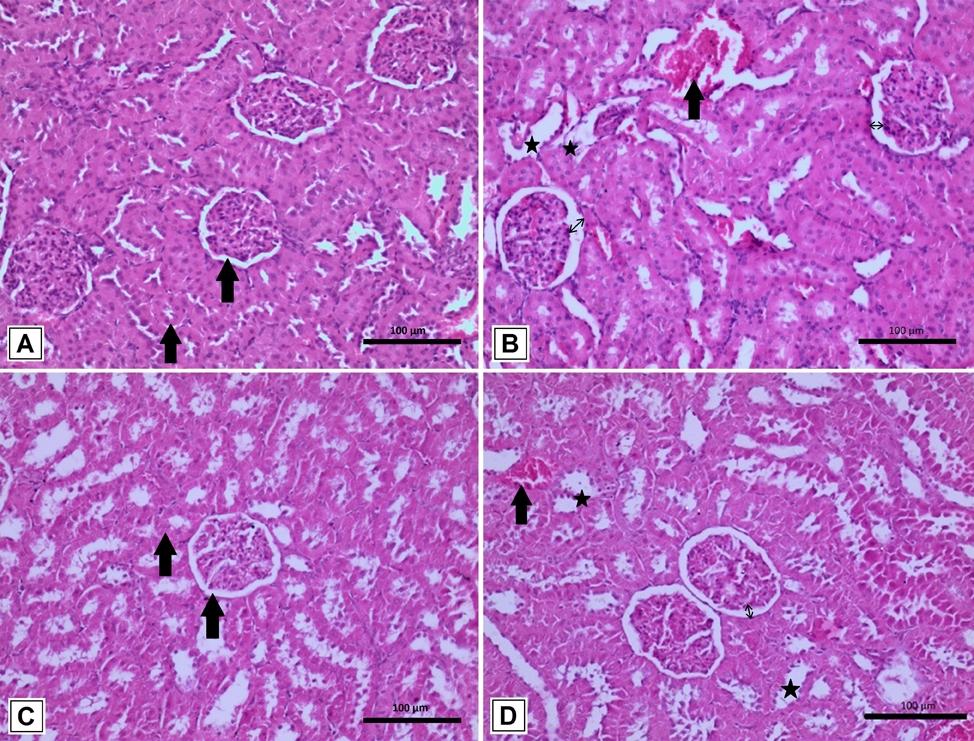
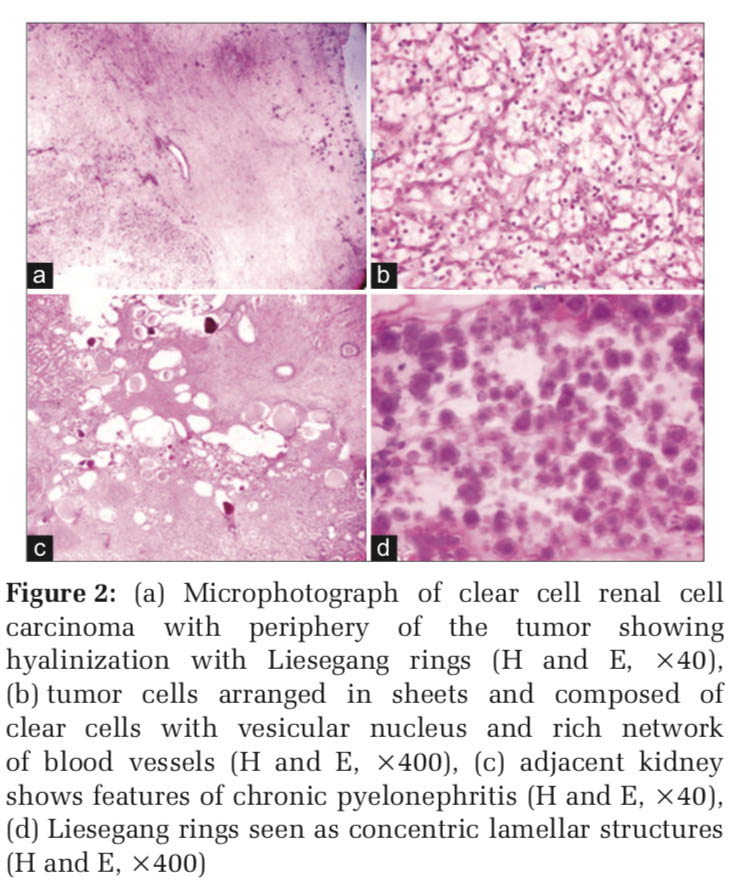
We received a left radical nephrectomy specimen of a 40-year-old female patient who presented with complaints of the left-sided lumbar pain, burning micturition, and hematuria for 1 week to our hospital. The patient also had a history of significant weight loss for the past 3 months. There was no history of diabetes or hypertension. On examination, she appeared pale. Per abdomen findings revealed a palpable mass in the left hypochondriac and lumbar region. The patient was advised for ultrasonography and contrast-enhanced computed tomography (Figure 1a). Radiological investigations revealed a hypoechoic mass in the upper pole of the left kidney suggestive of a malignant renal tumor. After routine clinical investigations, the patient underwent left radical nephrectomy. On gross examination, the left radical nephrectomy specimen measured 17 cm × 10 cm × 6 cm. Outer surface was lobulated at the upper pole. On cut section (Figure 1b), a circumscribed gray-yellow tumor measuring 9 cm × 8 cm × 6 cm was seen in the upper pole with areas of necrosis. Microscopically, a malignant tumor arranged predominantly in sheets and composed of cells having clear cytoplasm, vesicular nucleus, and occasional nucleoli admixed with rich thin network of blood vessels was noted. <5% of the tumor showed necrosis. Adjacent kidney showed features of chronic pyelonephritis. A diagnosis of CC-RCC, WHO/ ISUP Grade II, and a stage of pT2aNxMx was made (Figure 2a-c).
An interesting feature observed was at the periphery of the tumor in the region of pelvis, an extensive area of hyalinization with several amphophilic spherical- laminated structures having an amorphous central core resembling LRs (Figure2d). They were highlighted by special stains such as periodic acid–Schiff (PAS) (Figure 3a), Papanicolaou (PAP) (Figure 3b), and Gram’s stain (Figure 3c). These rings were non-refractile on polarizing light and negative for Congo red stain. An unusual feature noted was fading away of these rings immediately on mounting the slides with distyrene, a plasticizer, and xylene and eventually with time even without mounting the slides (Figure 3d).
The term LRs are attributed to the Liesegang phenomenon, first described by the German biochemist R. E. Liesegang, in 1896. According to him, these rings formed in vitro by periodic precipitation of certain chemicals around a central nidus in colloidal gels.[3] Over the years, LRs have been well recognized in the field of chemistry and attributed to the rhythmic accumulation of sub- and super-saturation of insoluble products in a colloidal matrix, which precipitate by diffusion resulting in characteristic precipitation rings. Hence, their formation involves an interplay of nucleation, precipitation, and supersaturation. They are usually spherical and vary in size from 5 nm to 820 nm.[1]
LRs are often mistaken for eggs or larvae of parasites, psammoma bodies, calcification, Michaelis–Gutmann bodies, corpora amylacea, hyaline globules of adenoid cystic carcinoma, and collagenous spherulosis.[2,3] In the past, it was often mistaken for ova, larvae, or adult forms of “giant kidney worm,” dioctophyma renale which is a large nematode whose mature form is found in the kidneys of mammals.[3]
Immunohistochemical and special stains for calcium, iron, mucopolysaccharide, amyloid, glycogen, keratin, and epithelial membrane antigen are negative.[1] They show negative staining with Perls, Von Kossa, Congo red, Alcian blue, mucicarmine, and Masson’s trichrome.[3] Special stains, radiographic analysis, or scanning electron microscopy in some cases have revealed that these rings contain iron, silicon, and sulfur.[1] Hence, their exact composition is not fully understood.
LRs have been reported mostly in association with calcifying epithelial odontogenic tumor, cysts of kidney and breast, conjunctiva and eyelid, paranasal sinus, submental mass, and in association with endometriosis and chronic salpingitis, and peritoneum.[4-9] Isolated cases of LRs have also been reported with tubercular lymph node.[10]
The largest case series was reported by Tuur et al., in 1987, where they described LRs in lesions from 29 patients mostly from kidney, synovium, conjunctiva, and eyelid. They found that majority of LRs formed in cysts, fibrotic, inflamed, or around necrotic tissue. There was a great variation noted in the size and shape of LRs ranging from 7 to 800 μ.[11]
Gupta, in 2009, reported 14 cases of LRs seen in breast cysts on fine-needle aspiration studied over a period of 26 years. This has been one of the largest case series reported on LRs. He found that there was the presence of several apocrine cells around the LRs; however, the role of these cells in the formation of LRs remained unclear. Under polarized light, the rings were found to be non-refractile, and no birefringence was noted in Congo red-stained preparations.[5]
Onodera et al., in 2009, reported a rare case of biliary deposition of LR presenting as a tumor-like polypoid mass in the liver in a 70-year-old man which again shows the rarity of sites it can occur.[12]
In our study, special stains-Gram’s, PAS, and PAP highlighted the rings and helped us in better understanding the morphology of these rings. An interesting fact noted which has not been reported in literature was the fading away of these rings rapidly on mounting the slides and with time even when slides were not mounted. However, the exact cause for this could not be determined and further studies are required to find out the specific cause for the occurrence of such phenomena.


In literature, LRs are usually described in relation to cystic or inflammatory lesions. However, they can also be found in close proximity to tumors like in our case. It is important to be aware of this rare entity and recognize them to avoid mistaking them with parasites, calcifications, corpora amylacea, etc. Further studies are needed to authenticate the significance of these rings.
Subscribe now for latest articles and news.