Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.2019.v05i02.008
Year: 2019, Volume: 5, Issue: 2, Pages: 36-37
Case Report
Ganesh Nallur Shivu, Anzy Azad, Vivek G Raman
Department of Cardiovascular Sciences, Sparsh Superspecialty Hospital, Bangaluru, Karnataka, India
Address for correspondence:
Ganesh Nallur Shivu, Department of Cardiovascular Sciences, Sparsh Superspecialty Hospital, Bangaluru, Karnataka, India. E-mail: [email protected]
Patients with Ebstein’s anomaly can present with bradyarrhythmias at any age. In view of the abnormal tricuspid valve anatomy associated with this condition, pacing these individuals can present with various challenges. We present a patient with Ebstein’s anomaly and complete heart block who was successfully treated with transvenous permanent pacing using the low septal position for lead placement.
KEY WORDS:Complete heart block, Ebstein’s anomaly, permanent pacing, septal pacing.
Patients with Ebstein’s anomaly can present with bradyarrhythmias at any age. In view of the abnormal tricuspid valve anatomy associated with this condition, pacing these individuals can present with various challenges. We present a patient with Ebstein’s anomaly and complete heart block who was successfully treated with transvenous permanent pacing.
A 60-year-old female with a known history of Ebstein’s anomaly presented with recurrent episodes of syncope. Her ECG demonstrated features of complete heart block with Himalayan P waves, prolonged QRS complex, and extreme left axis deviation. Echocardiography revealed features of Ebstein’s anomaly with severe tricuspid regurgitation and right atrial dilatation. The septal leaflet of the tricuspid valve was displaced 13 mm toward the apex. The left ventricular systolic function was normal.
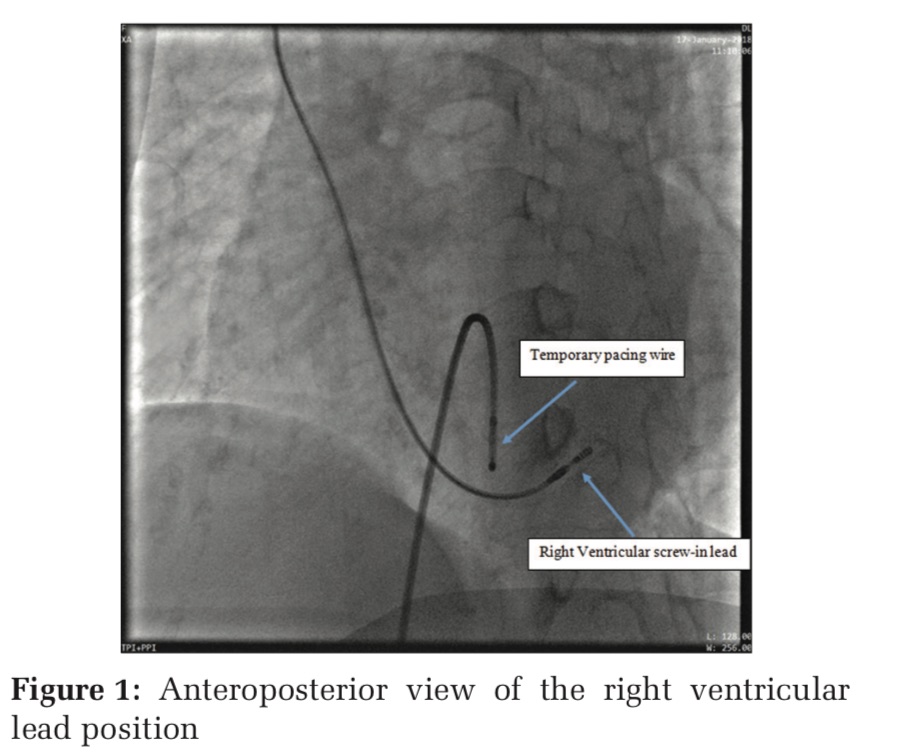
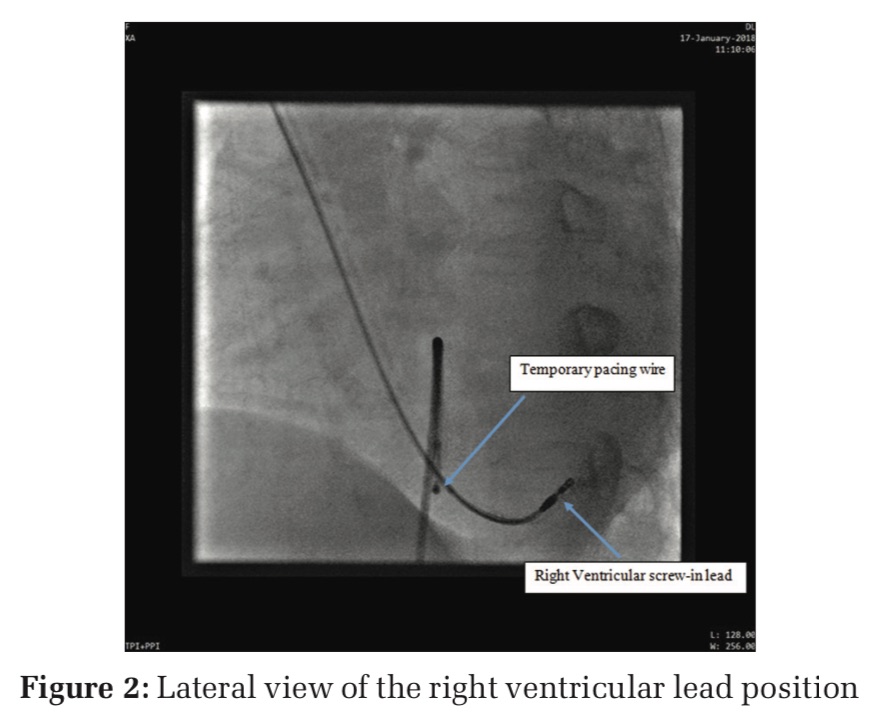
Permanent transvenous pacing was planned in view of the clinical presentation and ECG findings. A left axillary venous approach was taken. A screw in the right ventricular lead was placed in the distal septum of the right ventricle (Figures 1 and 2). This unconventional position was used in view of the abnormal anatomy. Despite this, the lead position has been stable and the patient is asymptomatic on follow-up of more than 6 months.
Permanent pacing in Ebstein’s anomaly can present various hurdles either due to abnormal position of tricuspid valve or previous surgery including tricuspid valve replacement. Jayaprakash et al. have elegantly described the various unique positions and methods that can be used for pacing in these individuals.[1] Epicardial leads have been placed through mini-thoracotomy or the cardiac veins have been used for pacing. Allen et al. reviewed all Ebstein’s patients who had pacing done at their center.[2] Pacing was done epicardially in patients receiving VVI pacemaker and in patients receiving dual-chamber pacemakers, a combination of epicardial and transvenous routes was used. The right ventricular outflow tract and atrialized portion of the right ventricle also have been used for pacing. Lopez et al. demonstrated the use of cardiac veins for insertion of internal cardioverter-defibrillator.[3] The defibrillator lead was placed in the middle cardiac vein. Our case is unique in that we obtained good results by unusual positioning of the leads. We used a screw-in lead which aided the lead to be stable in the low septal position. This position of lead placement can be used in other patients with Ebstein’s. However, obtaining this position may not be easy and would depend on the position of the septal leaflet of the tricuspid valve. Lead displacement would be the main concern in this lead position. A screw-in lead would be the choice in our patient in view of the septal positioning. The lead positioning in Ebstein’s anomaly can be challenging and routine apical positioning may not be favorable. Hence, screw-in leads would be desirable in these patients.
Subscribe now for latest articles and news.