Journal of Medical Sciences and Health
Year: 2022, Volume: 8, Issue: 1, Pages: 65-72
Original Article
Pallavi K Gedam1 , Sanjay M Chawhan2 , Seema S Chawhan3 , Manish L Pandhare4
1Assistant Professor, Department of Pathology, GMC, Gondia, 2Associate Professor, Department of Pathology, GMC, Gondia, 3Assistant Professor, Department of Biochemistry, GMC, Nagpur, 4Senior Resident, Department of Orthopaedics, GMC, Gondia
Address for correspondence: Sanjay M Chawhan, Associate Professor, Department of Pathology, GMC, Gondia.
E-mail: [email protected]
Context: The lesions of nasal cavity and paranasal sinuses provides problem in their diagnosis, prognosis and management because of limited anatomical space and certain unusual clinicopathological features. Aims: The present study was undertaken to study the incidence & frequency of various non-neoplastic and neoplastic lesions. It also aimed to describe the histomorphologic features of lesions of nasal cavity and paranasal sinuses. Settings and Design: This is a simple retrospective observational study. Methods and Materials: The material for present study was obtained as excisional biopsy of the lesions. The specimens were received in 10% formalin along with requisition form which also included the clinical data. The material was processed as routine histopathological examination. Special stains were done wherever required. Results: Total 62 cases were analyzed. The lesions were classified as non-neoplastic and neoplastic. The non-neoplastic lesions were classified according to classification given by Friedman and Osborn. Tumors of nasal cavity and paranasal sinus were classified according to WHO classification and observations compared with other studies. Conclusions: Non-neoplastic lesions were more common than neoplastic lesions. Sinonasal polyps were the most common lesions in the present study (50%). The age incidence ranges from 1st decade to 7th decade. There was slight female preponderance. The incidence of malignant tumours was slightly more than the benign tumours. Thus categorizing the sinonasal lesions according to histopathological features into various types helps clinicians to know the clinical presentation, the best management, clinical outcome and prognosis of the disease.
Keywords: Histopathology, Nasal, paranasal, Sinonasal, Polyp, WHO
The nose and paranasal sinuses (PNS) form a complex system of airway.[1] It comprises of epithelial, glandular, lymphoid, fibrovascular connective tissue, cartilage and bony elements.[2] It is the site of origin of some of the more complex, histologically diverse group of lesions which causes problem in their diagnosis, prognosis and management because of certain unusual clinicopathological features. The lesions of nasal cavity and PNS were first described by Hippocrates and Galen.[3] It forms a single functional unit with common pathological process,most of which are inflammatory. Cancers of the nose and PNS account for less than 1% of all malignancies and about 3 % of all head and neck cancers.
The material for the present study was obtained from the biopsies received in the pathology department of tertiary care academic institute. In case of nasal polyps, biopsies of the polyps were sent. The biopsies and the surgical specimens were received in 10% formalin along with requisition form which included the clinical data after taking informed consent. The material was processed as routine. Five micron thick sections were cut and stained with haematoxylin and eosin. Special stains such as Periodic Acid Schiff (PAS) and Grocott’s Methenamine Silver (GMS) were done wherever required. The histopathological and clinical data from 62 cases were analysed. The lesions were classified as non-neoplastic and neoplastic.
In the present study, 62 cases of non-neoplastic and neoplastic lesions of nasal cavity and PNS were studied over a period of seven years from tertiary care academic institute retrospectively. Out of which 41 cases were non-neoplastic and 21 cases were neoplastic. Out of 21 neoplastic cases, 10 cases were benign and 11 cases were malignant.
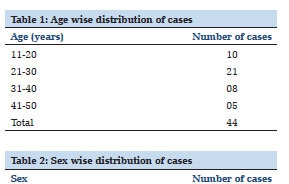
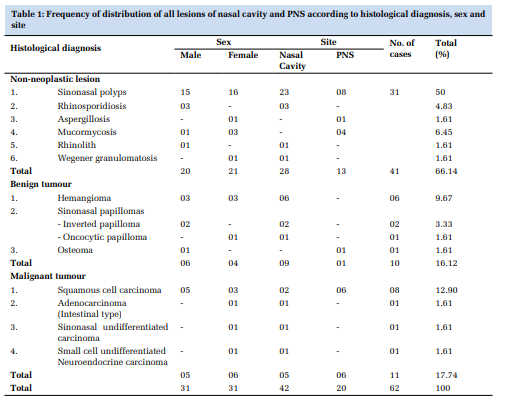
Table 1 shows the number of patients included in our study along with their histological diagnosis.
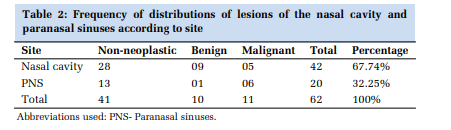
Non-neoplastic lesions (66.14%) were more common than neoplastic lesions in nasal cavity and PNS in present study. The age distribution for nonneoplastic lesions, benign tumours and malignant tumours was seen in age group 11- 30 years, 41- 50 year and 61-70 year respectively. The males and females were equally affected with male to female ratio was 1:1. Out of 41 cases of nonneoplastic lesions, 20 were males (48.78%) and 21 (51.22%) cases were females with slight female preponderance. The benign tumours were common in males and male to female ratio was 1.5:1. In present study, the malignant tumours were slightly common in females with male to female ratio of 0.9: 1. The lesions of nasal cavity (42 cases) were common than the PNS in the present study. Out of 41 cases of non-neoplastic lesions, 28 cases (68.29%) were in nasal cavity and 13 cases (31.71%) were from PNS. The benign tumours were more common (90%) in nasal cavity than PNS in the present study. The malignant tumours were slightly more (54.54%) in PNS than in nasal cavity. (Table 2)
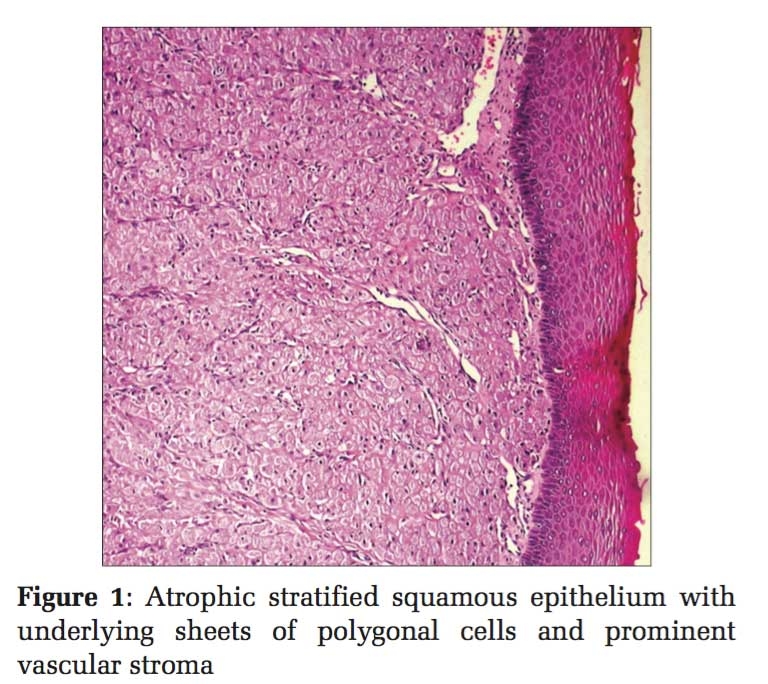
Out of 62 cases, 41 cases were of non-neoplastic lesions. Sinonasal polyp was the most common lesion seen in 31 cases (75.60%) (Figure 1 1) followed by mucormycosis (9.75%) (Figure 1 2) and rhinosporidiosis (7.32%). (Figure 1 3) Maximum cases were seen in age group of 11- 20 year (09 cases).
Out of 62 total cases, 21 cases were neoplastic. 10 cases were of benign tumours and 11 cases were of malignant tumours. Out of 10 benign tumours, hemangioma was the most common lesion (60%). Two cases of hemangioma were seen in age group of 61-70 year. All the cases of inverted papilloma, oncocytic papilloma and osteoma were seen in the age group of 41-50 year. In malignant tumours, squamous cell carcinoma (72.73%) was the most common histologic type in present study. (Figure 1 4) Maximum cases (05 cases) of squamous cell carcinoma were seen in the age group of 61-70 year.
The non-neoplastic lesions were classified according to classification given by Friedmann and Osborn. Tumours of nasal cavity and PNS were classified according to WHO classification and observations compared with other studies.
The present histopathological study includes 62 cases of nasal cavity and PNS. In present study, non-neoplastic lesions were 66.14% (41cases) and neoplastic lesions were 33.86% (21cases). In present study, non-neoplastic lesions outnumbered the neoplastic lesions and are comparable with study by Rawat et al (2012)and Modh et al (2013).[4,5] The age range in present study was from 1st to 7th decade. Zafar et al (2008)had reported the age range from 1st to 6th decade.[6] Gupta et al (2013) had reported the age range of 7 year to > 70 year.[7] According to Agarwal et al, out of 39 benign cases the most common age group for benign diseases (Non neoplastic lesions) was 41–50 years (5th decade) with 17 cases (43.6 %). [8]
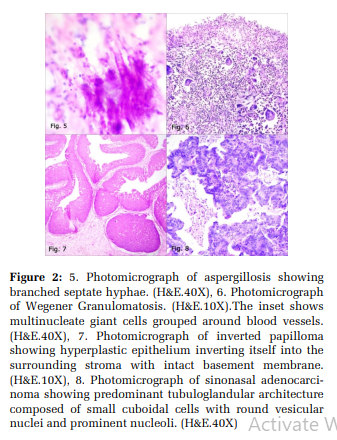
The study by Osho et al observed the sex ratio of 1:1.1 for non-neoplastic lesions and 1.8:1 for benign tumors respectively.[9] Regarding age, the most vulnerable period was 2nd to 3rd decades of life as observed by Garg et al. Malignant lesions were common in 6th to 7th decades and non-neoplastic lesions were 81.6% of the total cases of nasal cavity, paranasal sinuses and nasopharynx. [10] The median age of the presentation is the sixth decade, with men more commonly affected than women. The male to female ratio is 2.3:1.[11,12] Thus, there is wide range of age for presentation of lesions of nasal cavity and PNS. The lesions of nasal cavity and PNS had an equal predilection for males and females with male to female ratio being 1: 1. However other studies has greater predilection for males as compared to females. Nasal cavity was the predominant site of involvement with 42 cases (67.74%) compared to PNS with 20 cases (32.25%). Zafar et al (2008)also found nasal cavity as the predominant site of involvement (74.48%). [6] In present study, there were 41 cases of non-neoplastic lesions which were common in the age group of 11 to 20 years (09 cases) followed by 21 to 30 years (08 cases). Lathi et al (2011) and Parajuli et al (2013)also noted maximum 21 cases and 34 cases respectively in the age group of 11-20years.[13,14] The increased number of cases in younger age may be because of frequent exposure to infection due to more outdoor activities. In present study, frequency of female patient was quite more unlike that of other studies. Out of 41 cases of non-neoplastic lesions of nasal cavity and PNS, 31 cases were of sinonasal polyps. Out of 31 cases, 27 were non-allergic polyps and 04 were allergic polyps. Out of 27 cases of non-allergic polyps, 15 cases were from nasal cavity and 08 were from the maxillary sinus (Antrochoanal polyps). In present study, out of 41 cases of non-neoplastic lesions, we have 31 sinonasal polyps comprising of 75.60% of total cases which is compared with the study by Tondon et al (1971).[15] In present study, out of 31 cases of sinonasal polyps, more cases were seen in 2nd and 3rd decade which is comparable with Zafar et al (2008) and Ghosh and Bhattacharya (1966).[6,16] It is evident that polyps were common in the nasal cavity in all studies including present study. Histopathological examination revealed that, out of 31 cases of sinonasal polyp, 27 cases (87.09 %) were inflammatory in nature. Out of 27 cases of inflammatory polyps, 08 cases were of antrochoanal polyps (29.62%). Rawat et al (2013)found 49 cases of antrochoanal polyps (34.50%) in their study.[4] Four cases (12.90%) were allergic in nature. Lathi et al (2011) observed allergic polyps (62.5%) were more common than inflammatory polyps (25%).[7] Out of 41cases of non-neoplastic lesions of nasal cavity and PNS, 03 cases (7.32%) of rhinosporidiosis were found in present study. Bjerregaard et al (1992), Modh et al (2013)and Gupta et al (2013) found 6.16%, 1.81% and 12.16% cases of rhinosporidiosis respectively in their study.[5,7,17] Out of 03 cases of rhinosporidiosis, 02 cases were seen in 6th and 7th decade and one case in 3rd decade. Prabhakar et al (1985) and Balchandran (1990) reported maximum number of cases of rhinosporidiosis in 2nd and 3 rd decade.[11,12] In present study all the cases of rhinosporidiosis were found in males. Similarly, there was male predominance observed by various authors in their study. Out of 41 cases of nonneoplastic lesions of nasal cavity and PNS, only one case of maxillary sinus aspergillosis (2.44%) in a 35 year female was seen in present study. (Figure 2 5) Chang et al (1992)reported 13 cases of aspergillosis out of which 08 were male.[18] Study by Chang et al (1992) reported wide age range for aspergillosis from 47 year to 71 year. [18] Chang et al (1992) reported maximum number of cases in maxillary sinus. [18] Out of 41 cases, there were 04 cases (9.75%) of mucormycosis. Modh et al (2013) observed the frequency of mucormycosis as 3.64%.[5] Out of 04 cases of mucormycosis, two cases were seen in 7th decade. Modh et al (2013)observed maximum number of cases in 5th decade of life.[5] In present study, out of 04 cases, 03 were of females. Modh et al (2013) observed all the cases of mucormycosis in males.[5] In present study, all the lesions were seen in the maxillary sinus.
Out of 41 cases of non-neoplastic lesions of nasal cavity and PNS, only one case of rhinolith was seen in 55 year male. (2.44%) Rawat et al (2013) and Gupta et al (2013) observed the frequency of rhinolith as 1.75% and 2.70% respectively.[4,7] Study by Rawat et al (2013) showed mean age of presentation as 9.25 year and equal predilection for male and female.[4] Out of 41 cases of non-neoplastic lesions of nasal cavity and PNS, only one case of Wegener granulomatosis was seen. (2.44%) (Figure 26). Modh et al (2013) observed the frequency of Wegener granulomatosis as 0.9%.[5] The age of presentation in present study was 25 year female. Study by Modh et al (2013) showed presentation of Wegener granulomatosis in a 17 year male.[5] In present study 21 cases of neoplastic lesions of nasal cavity and PNS were found. Out of 21 cases, 10 cases were of benign and 11 cases were of malignant tumours. In present study, malignant tumours (52.38%) were slightly more common than benign tumours (47.61%). Buchanan and Slavin (1972) also found malignant tumours (76.36%) more common than benign tumours (23.63%) in their study.[19] Lathi et al (2011), Rawat et al (2012), Modh et al (2013)and Gupta et al (2013) observed predominance of benign tumours as compared to malignant tumours in their study.[4,5,7,13] In present study, neoplastic lesions of nasal cavity and PNS had a greater predilection for males as compared to females with male to female ratio being 1.1: 1 as observed in other studies. Out of 21 cases of neoplastic lesions of nasal cavity and PNS, 14 cases (66.66%) were found in nasal cavity as compared to 07 cases (33.34%) of PNS. Dewan et al (2013)also found nasal cavity as the predominant site of involvement (57.32%). [20] In present study, out of 62 cases 10 cases were of benign tumours (16.12%). Out of 10 cases, there were maximum 04 cases in the age group 41 to 50 years. Ashok kumar et al (2013) observed maximum 21 cases in the age group 41 to 50 years.[21] The mean age of presentation for benign tumour in present study was 45.6 year. Ashok kumar et al (2013) and Dasgupta et al (1997)also noted mean age for benign tumour as 42.5 years and 32.4 years respectively. [21,22] Benign tumours of nasal cavity and PNS had a greater predilection for males than females with male to female ratio being 1.5: 1 which was comparable with study by Lathi et al (2011) and Ashok kumar et al (2013).[13,21] Out of 10 cases of benign tumours, 09 cases (90%) were seen in nasal cavity. Ashok kumar et al (2013)also found 82 cases (88%) in nasal cavity.[21] Out of 10 cases of benign tumours, hemangioma constituted 06 cases (60%). The other benign tumours in the decreasing order of frequency were 03 cases of sinonasal papilloma (30%) and one case of osteoma (10%). Bjerregaard et al (1991), Dasgupta et al (1997)and Lathi et al (2011) also observed hemangioma as the predominant benign tumour as 39%, 45% and 47% respectively in their study. [13,17,22] Bjerregaard et al (1992)and Ashok kumar et al (2013)found 31 cases (39.74%) and 27 cases (29.03%) of hemangioma in their study respectively. [17,21] There were 02 cases of hemangioma in 7th decade and one case each in 2nd , 3 rd, 4th and 6th decade. Deshmukh et al (1982) and Modh et al (2013) found more cases of hemangioma in 2nd decade and 3rd to 5th decade respectively. [5,23] In the present study, there were 03 males and 03 females having male to female ratio of 1:1. Deshmukh et al (1982)found male preponderance whereas Sayed and Al-Serhani (1997), Modh et al (2013) and Rawat et al (2013)had female preponderance for hemangioma in their study. [4,5,23,24] In present study, all cases were in the nasal cavity. Sayed and Al-Serhani (1997) and Lathi et al (2011)also observed all the cases in the nasal cavity.[13,24] Thus hemangiomas were common in nasal cavity than PNS. In present study, there were 04 out of 06 cases (66.66%) of capillary hemangiomas. Fu and Perzin (1974) also found capillary hemangioma in 30 out of 38 cases of hemangiomas (78.94%). [25] There were 03 cases (30%) of sinonasal papilloma which was comparable with study by Tondon et al (1971)and Bjerregaard et al (1992).[15,17] In present study all the cases were seen in 5th decade comparable with the study by Modh et al (2013)who found maximum cases of sinonasal papilloma in 4th and 5th decade. [5] In present study, there were 02 males and 01 female with a ratio of 2:1 showing male preponderance. In present study, all 03 cases were seen in the nasal cavity. Ashok kumar (2013)observed 41 out of 44 cases in nasal cavity indicating predominant site of involvement.[21] In present study, 02 cases (66.64%) were of inverted papilloma (Figure 2 7) and one case (33.33%) was of oncocytic papilloma. Panchal et al (2005) observed inverted papilloma in 16 out of 20 cases (80%) of sinonasal papilloma. [26] Ashok kumar et al (2013) observed inverted papilloma in 40 out of 44 cases (90.90%). [21] In present study, out of 10 cases of benign tumours, only one case of osteoma was seen in 42 year male with frequency of 10% whereas, Fu and Perzin (1974)and Ashok kumar et al (2013)observed frequency of osteoma as 19.87% and 1.08% respectively in their study.[21,25] Ashok kumar et al (2013)reported only one case of osteoma in 18 year male whereas, Atallah and Jay (1981) observed osteoma in wide age range from 8 year to 77 years with male preponderance in a ratio of 1.5: 1. [21,27] In present study, the lesion was seen in the ethmoidal sinus. Atallah and Jay (1981)observed 01 case in ethmoidal and 13 cases in frontal sinus out of 23 cases of osteoma. [27] Ashokkumar et al (2013) reported a case of osteoma in frontal sinus. [21] In the present study of 62 cases, 21 cases were neoplastic out of which 11 cases were of malignant tumours. Malignant tumours were commonly seen in age group of 61 to 70 years (05 cases). Mean age of presentation was 57.9 years in comparison with study of Rawat et al (2013) who found mean age of 53 years in their study. [4] Lathi et al (2011)found more cases of malignant tumours in age group of 61 to 70 year (7 out of 13 cases). [13] Kazi et al (2009)also found majority of malignant tumours in 40 to 70 years of age. [28] In present study and study by Thakur et al (2001), there were slightly predominance of females than males (0.8: 1). [29] Out of 11 cases of malignant tumours, maximum 06 cases (54.55%) were seen in PNS and 05 cases (45.45%) in nasal cavity. Kazi et al (2009)reported high prevalence of malignant tumours in PNS (93.93%). [28] Lathi et al (2011)found all the malignant tumours in PNS. [13] In present study, out of 11 cases of malignant tumours, squamous cell carcinoma constituted 72.73% (08 cases). Modh et al (2013) found squamous cell carcinoma in 07 out of 16 malignant tumours (43.75%). [5] Gupta et al (2013)observed 05 cases (83.33%) of squamous cell carcinoma out of 06 cases of malignant tumours. [7] Thus, it showed that squamous cell carcinoma outnumbered other malignant tumours of nasal cavity and PNS. Lathi et al (2011)also observed 10.71% cases of squamous cell carcinoma comparable with present study.[13] All the cases of squamous cell carcinoma were encountered in age group of 5th to 7th decade with mean age of 64.3 year. Rawat et al (2013)found mean age of frequency for squamous cell carcinoma as 53 year.[4] Modh et al (2013)observed more cases of squamous cell carcinoma in 6th to 7th decade.[5] Lathi et al (2011)observed maximum number of cases in the 7th decade.[13] It was evident that there was male preponderance for squamous cell carcinoma of nasal cavity and PNS. Present study had male to female ratio of 1.6: 1 which was comparable with study by Ghosh and Bhattacharya (1966).[16] In present study squamous cell carcinoma was common in PNS (66.66%) which was comparable with study by Bjerregaard et al (1992)(65.12%). [17] In paranasal sinus, all the cases were noted in maxillary sinus. Lathi et al (2011) also noted all the cases of squamous cell carcinoma originating from maxillary sinus.[13] Out of 08 cases of squamous cell carcinoma, histologically 04 cases of moderately differentiated squamous cell carcinoma were identified. Gupta et al (1986) also observed moderately differentiated squamous cell carcinoma as the common grade in their study whereas, Kazi et al (2009)observed 10 out of 21 cases of poorly differentiated squamous cell carcinoma as common grade in their study. [28,30] In present study only one case of adenocarcinoma in 45 year female observed constituting 9.09 % of all the cases of nasal cavity and PNS (Figure 2 8) which was comparable with the study by Thakur et al (2001)(8.2%). [29] Age range for adenocarcinoma reported by Orvidas et al (2005) was from 24 year to 85 years. [31] Lopez et al (1990)reported adenocarcinoma in the age range of 50 year to 84 year. [32] Lee et al (2002)and Orvidas et al (2005)observed male preponderance in their study with male to female ratio being 1.2 : 1 and 2.4 : 1 respectively. [31,33] In present study a case of adenocarcinoma was observed in nasal cavity. Orvidas et al (2005)observed nasal cavity (83%) as the most common site of involvement.[31] In present study, we reported intestinal– type of adenocarcinoma (ITAC). Lopez et al (1990) observed intestinal type adenocarcinoma was the most common variant (83.33%). [32] Out of 11 cases of malignant tumours of nasal cavity and PNS, there was only one case of sinonasal undifferentiated carcinoma in a 35 year male with frequency of 9.09%. Neil Bhattacharya (2002)observed frequency of sinonasal undifferentiated carcinoma as 3.97% in their study. [34] Smith et al (2000) observed age range of sinonasal undifferentiated carcinoma from 25 year to 58 year. [35] Cerilli et al (2001) observed a wide age range from 20 year to 81 years. [36] Smith et al (2000)and Cerilli et al (2001)observed male predominance with male to female ratio of 3: 1 and 2: 1 respectively. [35,36] In present study, the lesion was seen in nasal cavity. Cerilli et al (2001)(72%) and Smith et al (2009) (70%) also observed common location of tumour in nasal cavity. [35,36] In present study, out of 11 cases of malignant tumour, only one case (9.09%) of small cell undifferentiated neuroendocrine carcinoma was found in a 42 year female. Smith et al (2009)observed 04 cases of small cell undifferentiated neuroendocrine carcinoma out of 10 malignant tumours (40%).[35] Smith et al (2009)observed wide range of age group for occurrence of small cell undifferentiated neuroendocrine carcinoma (17-58 years).[35] In the study by Smith et al (2009) male preponderance reported with male to female ratio being 3: 1.[35]
It is seen that there is a wide spectrum of lesions in the complex region of nasal and paranasal sinuses. Non-neoplastic lesions were more common than neoplastic lesions in the nasal cavity and paranasal sinuses. Hence categorizing the lesions of nasal cavity and paranasal sinuses according to histopathological features into various types helps the clinicians for the best management and clinical outcome of the disease.

Subscribe now for latest articles and news.