Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.v10.i1.23.220
Year: 2024, Volume: 10, Issue: 1, Pages: 32-38
Original Article
Sruthi Prasad1 , Thejasvi Krishnamurthy1 , M Priyanka2
1Associate Professor, Department of Pathology, Kempegowda Institute of Medical Sciences, Bengaluru,
2Department of Pathology, Kempegowda Institute of Medical Sciences, Bengaluru
Address for correspondence:
M Priyanka, Department of Pathology, Kempegowda Institute of Medical Sciences, Bengaluru.
E-mail: [email protected]
Received Date:26 June 2023, Accepted Date:27 December 2023, Published Date:04 April 2024
Background: Ulcerative colitis (UC) is a chronic inflammatory disease of unknown etiology characterized by a relapsing and remitting course. Assessment of disease activity is based on combination of clinical features, endoscopic scoring and histological scoring. Over the years, Histological healing has replaced mucosal healing as the therapeutic endpoint in UC. Various histological parameters have their own significance in predicting treatment outcomes and prognosis. Many histologic scoring systems have been proposed with one such validated score being Geboes score. However, in view of its complexity to use the Simplified Geboes Score (SGS) was developed in 2016. Aim & Objectives: To assess the interobserver agreement of SGS in ulcerative colitis. Methods: This was retrospective study of 6 years duration. Relevant clinical and endoscopic details were documented. 41 cases of UC were included in the study. The SGS scoring was done by two pathologists independently. Agreement for individual grades of SGS and for the detection of Histologic activity (score >3.1) was compared between both pathologists using Cohen’s kappa coefficient. Results: Majority of the patients were in the age group of 15-72 years with male preponderance. Left sided colon was more commonly involved with loose stools being most common symptom. Cohen’s test showed moderate to good agreement for individual grades and good agreement for Histologic activity. Conclusion: The SGS is simple to use and shows good interobserver agreement for histological activity and moderate to good agreement for individual parameter. Therefore, it can be adopted for routine reporting of all biopsies in ulcerative colitis.
Keywords: Histological healing, Mucosal healing, Simplified Geboes Score, Ulcerative colitis
Ulcerative Colitis (UC) is a chronic inflammatory disease of unknown etiology characterized by a relapsing and remitting course 1. Patients typically present with diarrhea, rectal bleeding and tenesmus 2. Chronically uncontrollable disease can lead to development of serious complications like colorectal cancer 3. Therefore, the determination of disease activity is important for therapeutic monitoring and predicting treatment outcomes 1. Assessment of disease activity is based on a combination of clinical features, endoscopic scoring and histologic scoring. Clinical and endoscopic remission is no more the therapeutic end point 1. Histologic inflammation is known to persist even with endoscopically normal mucosa, and is known to be associated with increased risk of disease relapse, dysplasia and colorectal cancer 4. Various histologic scoring systems have been proposed for assessment of disease activity, however only three have undergone extensive validation and these include- Geboes score, Nancy index and Robart’s histopathology index 4. Though the Geboes score is being used in clinical trials, its application in routine reporting is limited due to its complexity. Hence to overcome this, the Simplified Geboes Score (SGS) was developed in 2016 5.
In view of the presence of multiple parameters, the scoring system may show variability between different pathologists. The aim of this study is to assess the interobserver agreement of SGS in Ulcerative Colitis.
This was a retrospective study conducted over 6 years from 2013 to 2019. Slides of all endoscopically and histopathologically confirmed cases of ulcerative colitis were retrieved. Relevant clinical history and endoscopic details were collected from the Department of Gastroenterology and documented. The slides were examined individually by two pathologists (pathologist 1 and pathologist 2). Both pathologists have over 15 years experience in reporting histopathology, with one of them being a certified gastrointestinal pathologist. A consensus was reached on the specific diagnostic criteria for grading of individual parameters. Interpretation of the biopsies was done following that. The biopsies were screened and in case of multiple bits, the bits showing maximum activity were selected for interpretation. The Simplified Geboes Scoring system was applied. It includes 6 parameters- No inflammation, Basal plasma cells, Eosinophils in lamina propria, Neutrophils in lamina propria, Neutrophils in epithelium and Epithelial injury (Table 1) 5.
|
Grade |
Subgrade |
Interpretation |
|
|
Grade 0 No inflammatory activity |
0.0 |
No abnormalities |
No active inflammation (neutrophils) or no architectural changes |
|
0.1 |
Presence of architectural changes |
Branching crypts, crypts atrophy and loss |
|
|
0.2 |
Presence of architectural changes and chronic mononuclear cell infiltrate |
Branching crypts, crypts atrophy and loss, lymphoplasmacytic infiltrate. |
|
|
Grade 1 Basal plasma cells |
1.0 |
No increase |
No plasma cells |
|
1.1 |
Mild increase |
Plasma cells seen in single position in single fragments |
|
|
1.2 |
Marked increase |
Multiple fragments in single or multiple slides or band like infiltrate seen in all slides |
|
|
Grade 2A Eosinophils in lamina propria |
2A.0 |
No increase |
Normally few eosinophils are seen in lamina propria |
|
2A.1 |
Mild increase |
Compact group of eosinophils in lamina propria |
|
|
2A.2 |
Marked increase |
Multiple compact groups or diffuse presence of eosinophils |
|
|
Grade 2B Neutrophils in lamina propria |
2B.0 |
No increase |
No neutrophils |
|
2B.1 |
Mild increase |
Neutrophil seen only in 40x |
|
|
2B.2 |
Moderate increase |
Neutrophils seen in low power |
|
|
Grade 3 Neutrophils in epithelium |
3.0 |
None |
No neutrophils in epithelium |
|
3.1 |
<50% crypts involved |
Cryptitis, crypt distortion and crypt abscess seen in few crypts |
|
|
3.2 |
>50% crypts involved |
Cryptitis, crypt distortion and crypt abscess seen in more crypts |
|
|
Grade 4 Epithelial injury (in crypt and surface epithelium) |
4.0 |
None |
- |
|
4.1 |
Marked attenuation |
- |
|
|
4.2 |
Probable crypt destruction: probable erosions |
Includes crypt branching, tortuosity, dilation and variation in size and shape |
|
|
4.3 |
Unequivocal crypt destruction: unequivocal erosion |
Loss of continuity between the epithelial cells within the crypts |
|
|
4.4 |
Ulcer or granulation tissue |
Indicates higher grade of inflammation |
|
All cases of UC were interpreted using SGS, as shown in Table 1 5. Basic interpretation of few of the parameters was carried out as per the criteria discussed below. Basal plasmacytosis is defined as plasma cells separating the base of colonic crypts from the muscularis mucosae 6. Interpretation of Eosinophils is tricky, as they are normally seen more in the right side of colon than left colon 7. This was considered while interpreting the biopsies. Neutrophils are not seen in normal colon and presence of any neutrophils either in the lamina propria or epithelium was considered abnormal 8.
Histologic activity was defined by a score of ≥3.1 5. Individual parameters were then analyzed to assess inter observer agreement for each grade and also for histologic activity. The Cohen's kappa test was applied to measure the strength of agreement. The score ranges from 0 to 1, where score of <0.20 indicates very low agreement, 0.20-0.40 is low agreement, 0.41- 0.60 is moderate, 0.61-0.80 is good, 0.81-1.00 is almost perfect and 1 is perfect agreement 5.
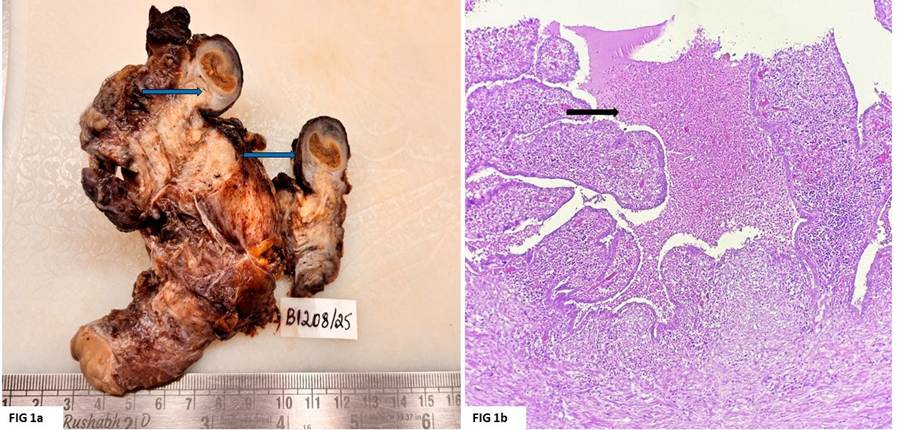
A total of 42 slides were retrieved. One case was excluded from the study as it showed only granulation tissue and inflammatory exudate. The study included biopsies from 27(65. 8%) male patients and 14(34.1%) female patients. The age of the patients ranged from 15 to 72 years with mean age group of 43years. Most of the patients presented with loose stools. Of the 41 cases, 19 were from the right side of colon and 22 from left side of colon.
Table 2 shows the frequency distribution of parameters in Simplified Geboes Score by both the pathologists and interobserver agreement measured by kappa coefficient (Table 2 Figure 1, Figure 2, Figure 3, Figure 4 ).
|
Grade |
Pathologist 1 (n/ %) |
Pathologist 2 (n/ %) |
Kappa coefficient |
Agreement |
|
Grade 0: No inflammatory cells |
||||
|
0.0 |
2 (4.87%) |
2 (4.87%) |
0.513 |
Moderate agreement |
|
0.1 |
1 (2.43%) |
2 (4.87%) |
||
|
0.2 |
38 (92.68%) |
37 (90.24%) |
||
|
Grade 1: Basal plasma cells |
||||
|
1.0 |
9 (21.95%) |
11 (26.82%) |
0.678 |
Good agreement |
|
1.1 |
20 (48.78%) |
15 (36.58%) |
||
|
1.2 |
12 (29.26%) |
12 (29.26%) |
||
|
Grade 2A: Eosinophils in lamina propria |
||||
|
2A.0 |
14 (34.14%) |
19 (46.83%) |
0.532 |
Moderate agreement |
|
2A.1 |
21 (51.21%) |
13 (31.70%) |
||
|
2A.2 |
6 (14.63%) |
6 (14.63%) |
||
|
Grade 2B: Neutrophils in lamina propria |
||||
|
2B.0 |
4 (9.75%) |
8 (19.56%) |
0.659 |
Good agreement |
|
2B.1 |
25 (60.97%) |
7 (41.46%) |
||
|
2B.2 |
12 (29.26%) |
13 (31.70%) |
||
|
Grade 3: Neutrophils in epithelium |
||||
|
3.0 |
3 (7.31%) |
4 (9.75%) |
0.678 |
Good agreement |
|
3.1 |
34 (82.92%) |
6 (14.63%) |
||
|
3.2 |
4 (9.75%) |
31 (75.60%) |
||
|
Grade 4: Epithelial injury (in crypt and surface epithelium) |
||||
|
4.0 |
3 (7.3%) |
6 (14.63%) |
0.335 |
Low agreement |
|
4.1 |
0 |
3 (7.3%) |
||
|
4.2 |
16 (39.02%) |
19 (46.34%) |
||
|
4.3 |
13 (31.70%) |
6 (14.63%) |
||
|
4.4 |
9 (21.95 %) |
7 (17.07%) |
||




The agreement for the detection of histologic activity (score ≥3.1) using was compared between both the pathologists using kappa coefficient. Of the 41 cases, Pathologist 1 scored 38 cases (92.68%) as histologically active disease and 3 cases (7.3%) as inactive. Whereas Pathologist 2, scored 35 cases (85.3%) as histologically active disease and 6 cases (14.63%) as inactive disease. This showed good agreement with kappa coefficient of 0.678. A total of 3 cases (7.3%) showed no correlation between both pathologists in assessing histologic activity.
Over the years histologic healing has slowly replaced clinical and endoscopic healing to become the targeted therapeutic goal in UC 9. The absence of histologic healing, makes patients prone to develop recurrences/ relapses and also confers them to an increased risk of dysplasia 10. An interest in histologic inflammation was seen as early as 1966, when Wright and Truelove attributed persistent histologic inflammation to poor clinical outcomes even with endoscopically normal mucosa 4. In 1991, 25yrs later, Riley et al, demonstrated that active inflammation on histology is associated with disease relapse among patients in remission 3. Ever since, many researchers have studied the association between different histologic parameters and relapse/ refractoriness to therapy. Thus, many scoring systems came into existence. Among the 30 scoring systems available for grading UC some are complex to use and only a few have been validated- one such score is Geboes score 11. Though the scoring systems have been used extensively in clinical trials, their use in routine reporting is limited mainly due to their complexity and interobserver variability 12. Therefore, assessment of interobserver variability becomes essential to rely on reproducibility. Other scoring system used for UC is Nancy Index (NI) and Robarts Histopathology Index (RHI). NI is the simplest scoring system to use but it doesn't evaluate important prognostic parameters like basal plasmacytosis, increase in eosinophils and structural changes. Robart’s Histopathological Index (RHI) has a better definition of parameters which makes it a better scoring system over GS for routine use. It also evaluates basal plasmacytosis which is an important prognostic parameter. Unlike GS, it does not evaluate increase in eosinophils
Amezaga et al, reviewed 103 biopsies using Original Geboes Score (OGS) and SGS. These histological scores were each compared with Mayo Endoscopic subscores. They further studied interobserver agreement for both OGS and SGS between 3 trained readers with experienced Gastropathologists. The interobserver agreement showed moderate agreement for all grades of SGS and also OGS except for grade 2B where it showed low agreement 5.
The current study showed poor agreement for Grade 4, moderate for Grade 0 and Grade 2A, whereas good agreement was noted for Grades 1, 2B and 3 (Table 2). Each of the individual parameters in SGS have their own relevance in disease monitoring as discussed below.
Grade 0- No inflammatory activity with architectural changes: This is characterized by features such as branching crypts with loss of parallelism, crypt shortening, crypt loss and atrophy 13. These features may be seen even in complete remission and their persistence in patients on clinical remission/ mucosal healing is predictive of relapse within short time period 14.
Grade 1- Basal plasmacytosis: It is defined by expansion of the space between the base of the crypts and muscularis mucosae by plasma cells 6. BP has been confirmed and validated by various studies as an early diagnostic feature and also an important prognostic factor. The persistence of BP during remission can predict disease relapse, especially in asymptomatic cases. Basal plasmacytosis as a parameter is also being used in other scoring systems like Robart’s Histopathology Index, which is derived from Geboes Score 15.
Grade 2A- Eosinophils in lamina propria: Eosinophils in the lamina propria are normally present in the colon and more so in the right colon 16. They also show geographic and seasonal variations. There is no definite criteria as to what exactly constitutes increased eosinophils. A good knowledge of histology is therefore crucial for interpretation of eosinophils. Similar to current study, other studies have also shown only a moderate inter observer agreement 17. Eosinophils may be increased in both active and quiescent disease 18. Increased eosinophils are also seen to be associated with relapses, indicate non responsiveness to therapy. They are also known to constitute a high risk towards the development of fibrosis and stenosis 19.
Grade 2B and Grade 3-Neutrophils in the lamina propria and in the epithelium: The colonic mucosa usually does not show any neutrophils, so the presence of neutrophils either in lamina propria or epithelium is abnormal. As per, the RAND consensus even the presence of two neutrophils in the colonic mucosa constitutes active inflammation 4. Also, persistence of activity among the patients on treatment is said to be associated with poor clinical outcomes as well as relapses 6. Lobaton et al, noted that a combination of basal plasmacytosis and intraepithelial neutrophils showed a strong association with disease relapse 10. Few studies have also shown that persistence of cryptitis and crypt abscess are predictors of an aggressive and refractory disease 9.
Grade 4, Epithelial injury (in crypts and surface epithelium). A marked variation was noted in grading Grade 4.1 between both the pathologists. Pathologist 1 did not notice marked attenuation of crypts in any of the biopsies, whereas Pathologist 2 noticed the same in 3 (7.3%) cases. The grading lacks precise defining criteria for 4.1. This could have been the cause for subjectivity between both the pathologists. It could have been improved by prior discussions between both the pathologists on arriving at precise definitions for Grade 4.1.
The current study showed substantial agreement for histologic activity (>3.1) as shown in Table 2, whereas Amezaga et.al showed moderate agreement 5. The presence of even two neutrophils in the colonic mucosa is considered activity 9.
A total of 3 cases (7.3%) showed no correlation between both pathologists in assessing histologic activity. Here pathologist 2 graded all three cases as absence of neutrophils in epithelium (Grade <3.1) while Pathologist1 graded them as active (Grade ≥3.1). This could be due to lack of adequate screening, thus neglecting the presence of occasional neutrophils.
Mucosal healing on endoscopy is not the therapeutic end point, instead it is histologic healing as observed on biopsy. Thus, it is recommended to biopsy the colon for microscopic evaluation in all UC, even in those with endoscopically normal mucosa 12. Also, considering the impact of identification of various histologic parameters on disease prognosis and treatment responses, it is valuable to adopt these in routine scoring of all biopsies of UC.
The current study is limited by evaluation of slides by only two pathologists. Study of slides by more pathologists with assessment of interobserver agreement would have added more credibility.
Over the years, Histologic healing has replaced mucosal healing as the therapeutic endpoint in UC. Various histologic parameters have their own significance in predicting treatment outcomes and prognosis. Thus, adopting a standard scoring system for routine histopathological reporting of all cases is essential. The SGS is simple to use and shows good interobserver agreement for histological activity and moderate to good agreement for individual grades. Therefore, it can be adopted for routine reporting of all biopsies in Ulcerative Colitis.
Subscribe now for latest articles and news.