Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.2015.v01i02.007
Year: 2015, Volume: 1, Issue: 2, Pages: 34-35
Case Report
Ishi Sharma1, Anshul Gupta1, Richa Jindal2, Molly Joseph3
1Post Graduate, Department of Pathology, St. Stephens Hospital, New Delhi, India,
2Specialist, Department of Pathology, St. Stephens Hospital, New Delhi, India,
3Head, Department of Pathology, St. Stephens Hospital, New Delhi, India
Address for correspondence:
Dr. Ishi Sharma, Department of Pathology, St. Stephen’s Hospital, New Delhi, India. E-mail: [email protected]
Histoplasmosis is not uncommon in India. However, most of cases have been sporadic unlike epidemics seen in USA. The under reporting of this fungal infection in India may be influenced by epidemiology of tuberculosis and lack of awarenass and diagnostic laboratory facilities. A high index of suspicion is required for its diagnosis.
KEY WORDS:Granulomatous inflammation, histoplasmosis, seronegative
IntroductionHistoplasma capsulatum is a dimorphic fungus that grows as a mold in nature or on Sabouraud’s agar at room temperature.[1] The under-reporting of this fungal infection in India may be influenced by the epidemiology of tuberculosis and lack of awareness and diagnostic laboratory facilities. A high index of suspicion is required for its diagnosis.[2] Here, we present a case of histoplasmosis of the scalp. |
||
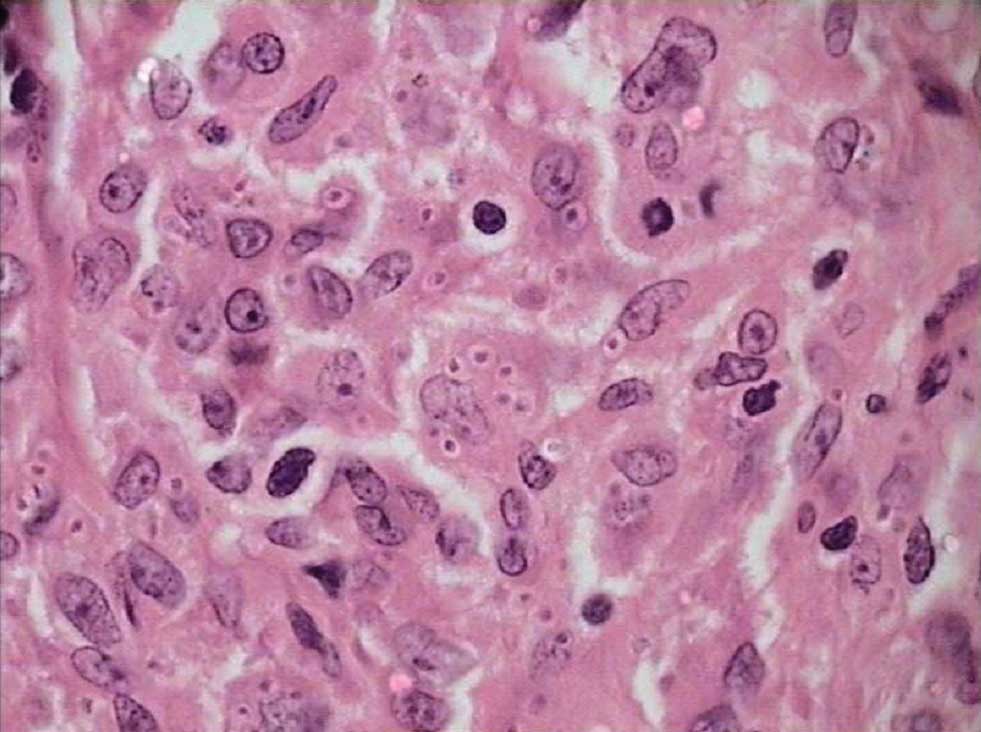
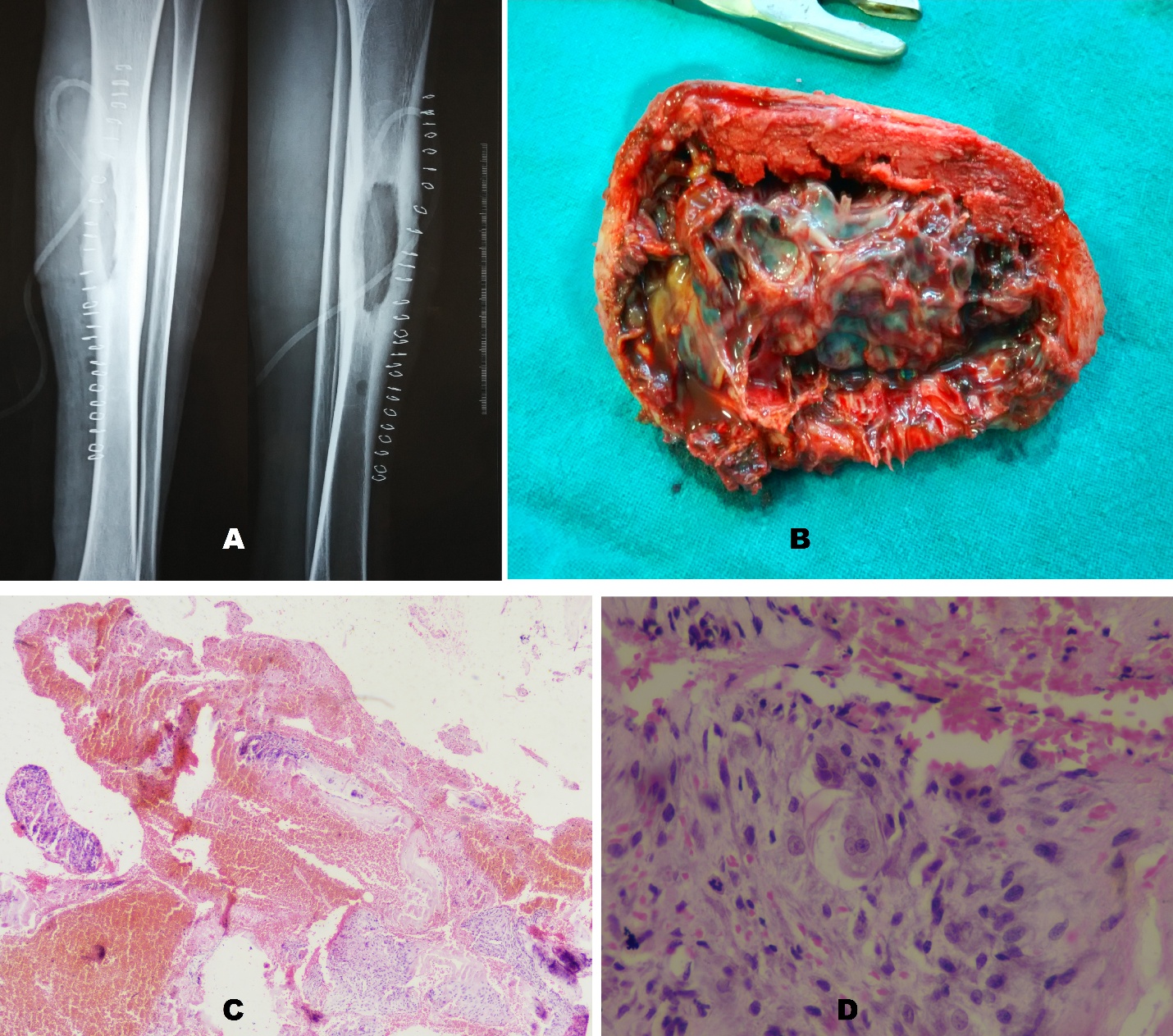
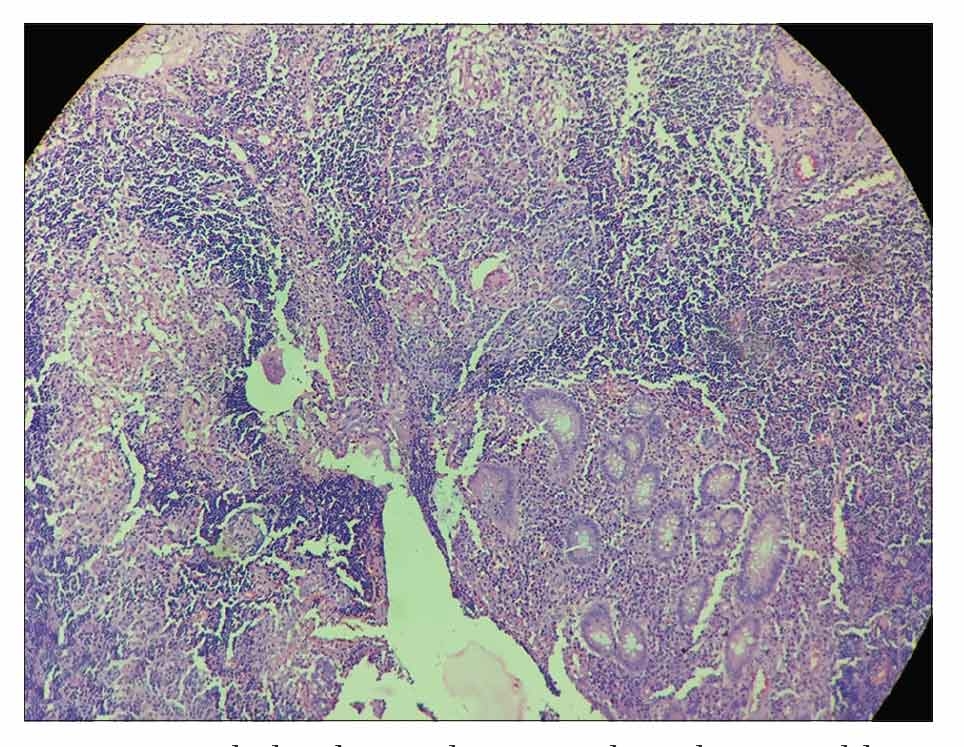
Case ReportA 48-year-old male presented with slowly increasing scalp swelling present for 2 to 2½ months with headache. No neurological deficit was detected in the clinical examination. There was no other positive finding. AFB: Negative A final opinion of granulomatous inflammation of the scalp with fungal organisms resembling histoplasma was made. |
||
|
||
DiscussionThis infection is acquired by inhalation of dust particles from soil contaminated with bird or bat droppings that contain small spores (microconidia), the infectious form of fungus.[3] Spores can be recognized in sections stained with H and E as round oval bodies surrounded by a clear space.[5] Primary cutaneous inoculation histoplasmosis is benign and self-limited in duration. It generally occurs as a laboratory infection. Cutaneous lesions occur in 6% of cases with disseminated histoplasmosis. They consist of either papules or nodules that undergo ulceration, large plaque-like lesions or primary ulcer. In this case, patient has presented as a primary lesion over the scalp, which is the rare site for the histoplasmosis.[5] Very few cases of histoplasmosis of the scalp causing bony erosions have been reported. |
Subscribe now for latest articles and news.