Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.2015.v01i01.003
Year: 2015, Volume: 1, Issue: 1, Pages: 14-18
Case Report
Ashish H Shah1, Eduardas Subkovas2, Christopher M Bellamy3, Nicholas P Waterfield3, Paul Das2
1 Coronary, Structural and Congenital Interventional Fellow, Department of Cardiology, Toronto General Hospital, University Health Network, Toronto, Canada,
2 Consultant Interventional Cardiologist, Department of Cardiology, Glan Clwyd Hospital, Bodelwyddan, Wales, United Kingdom,
3 Consultant Cardiologist, Department of Cardiology, Glan Clwyd Hospital, Bodelwyddan, Wales, United Kingdom
Address for Correspondence:
Dr. Ashish Shah, Department of Cardiology, Toronto General Hospital, Toronto, Ontario, M5G 0B2, Canada.
Tel.: +1 416-835-2822. E-mail: [email protected]
Vasospastic angina (VA) is characterized by segments of coronary artery that have exaggerated constrictor response to a variety of stimuli, resulting in partial or complete occlusion of the vessel, leading to myocardial ischemia. Here, we are presenting a case report of a patient who was known to have VA. Initially, she was treated with pharmacotherapy. Once it became treatment-refractory and involved left main stem and exposed significant amount of myocardium at risk, it required treating with percutaneous coronary intervention, which controlled her symptoms markedly. We briefly discuss the treatment options currently available.
KEY WORDS: Refractory, treatment, vasospastic angina
IntroductionVasospastic angina (VA) is highly probable in patients presenting with recurrent cardiac sounding chest pain without any clear precipitating factors, mainly in the night or early in the morning, with dynamic ST-T segment changes affecting multiple electrocardiogram (ECG) leads in the absence of flow-limiting coronary artery disease (CAD).[1,2] In patients with VA, vascular smooth muscle reactivity is variable to multiple stimuli (such as cold, emotion, hyperventilation, or even exercise).[1,2] Clusters of angina interspersed by symptom-free periods also characterize the VA in some of the patients. The exact underlying mechanism for VA is unknown, but thought to be due to increased sensitivity of the contractile protein of the vascular smooth muscle that activates through different receptors and pathways.[1] This hypothesis is supported by the fact that attempting to treat the condition with individual receptor antagonist has failed, whereas agents that suppress the smooth muscle contractility, such as calcium channel blocker (CCB) and nitrates are more effective.[3] Diagnosis is usually delayed due to the transient and dynamic nature of coronary artery spasm involving either the single or multiple segments, so that by the time patient presents to the hospital, ECG may have normalized. In the majority of patient’s intensity and duration of coronary spasms are not enough to result in troponin release, a highly sensitive marker to identify myocardial injury or infarction. Routinely performed stress tests, which can demonstrate myocardial ischemia in the presence of fixed atherosclerotic coronary stenosis, are unable to induce VA. Unless challenged by a provocation test, coronary angiography (CAG) demonstrates either normal or non-flow limiting mild CAD. If the proximal segments of major epicardial coronary arteries are affected and the spasm lasts for a long enough time, the resulting myocardial infarction or arrhythmias can be life threatening.[4] The majority of patients are successfully treated with CCB, either alone or in combination with nitroglycerine. However, there is a small subgroup of patients, who fail to respond to optimum medical management, and may require more invasive treatment options. |
||||||
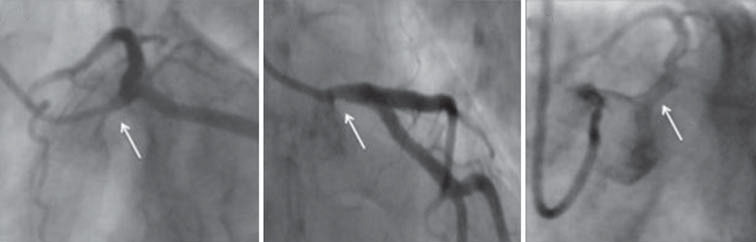
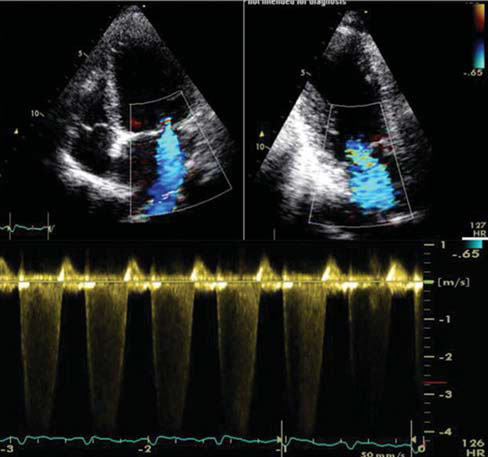
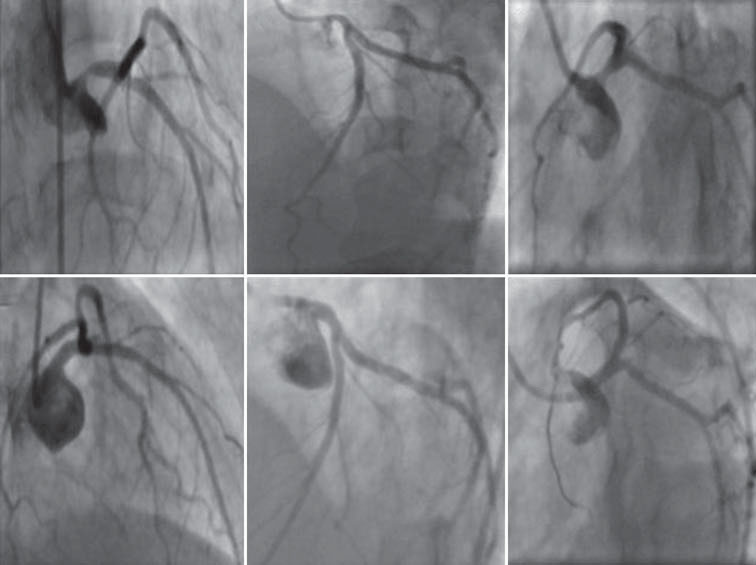
Case ReportA female patient initially presented in 1997 when she was 38-year-old, with cardiac sounding chest pain and significant dynamic ST-T changes on ECG. She underwent CAG that was reportedly normal. As she continued experiencing anginal attacks with angiographically normal coronary arteries, she was diagnosed as having syndrome-X. She was treated with anti-anginal medications, to which she responded very well. Her symptoms were well-controlled for more than a decade with amlodipine and isosorbide mononitrate (ISMN). She was re-admitted in 2009 with a prolonged episode of nitroglycerine refractory chest pain and dynamic ECG changes, but no troponin rise. As she had a prolonged and nearly symptom-free period, she was treated as having acute coronary syndrome and underwent CAG. The angiogram demonstrated the left main stem (LMS), to be of a smaller caliber than expected, using Finet’s adaptation of Murray’s Law (Figure 1a and b). Non-selective injection of the LMS, after the intra-coronary nitrate infusion, showed it to be of good caliber and free of any significant disease (Figure 1c). These findings confirmed the diagnosis of VA involving LMS. As her symptoms were well controlled with medications for more than a decade before her presentation, we decide to treat her medically. Once again, after a brief symptom-free period, she started having clusters of angina episodes, a few times every day, mainly early in the morning. Nitroglycerine, which was initially effective in terminating the episode, eventually failed, requiring multiple hospital admissions. Increasing dose of slow-release ISMN and amlodipine resulted in headache and symptomatic hypotension. Nicorandil helped her for a few months, but resulted in multiple oral ulcers, which resolved on its discontinuation and recurred upon recommencement of medication. Diltiazem caused generalized tiredness and documented second-degree atrio-ventricular nodal block. Despite being on optimum medical management, she continued experiencing troublesome angina on a daily basis. Over the prior month, she had noticed marked hoarseness of voice, dyspnea and sweating during each episode of chest pain. During one of the VA episodes, she was found to have an apical early-mid systolic murmur, which resolved within an hour from the termination of the anginal episode. Based on this clinical finding, we decided to perform the trans-thoracic echocardiogram (TTE) during an episode of chest pain. The TTE confirmed that she had significantly impaired global left ventricular systolic function along with left ventricular cavity dilatation, resulting in ischemic mitral regurgitation (MR) while she was in pain (Figure 2). This finding completely resolved within an hour from termination of her chest pain. Transient pulmonary edema and associated hypotension were also recorded during such an episode; quickly recovering once the chest pain resolved. These TTE findings clearly demonstrated that a significant amount of myocardium was at risk by the spastic segment of coronary artery, very likely to be the LMS. If such an extensive myocardial ischemia, lasted long enough, it could lead to either myocardial infarction or life threatening arrhythmia. In addition, the patient was failing to respond to routinely used anti-anginal medications. Hence, we decided to take her back to the catheter laboratory for further investigation, including acetylcholine provocation test. Angiographic findings were similar to those demonstrated in her previous CAG 6 months ago. But, before we could perform the provocation test, deep-seated catheter-induced significant LMS spasm causing recurrence of symptoms, (Figure 3a-c) which responded to intra-coronary nitrate. Left ventriculogram, performed immediately after the LMS spasm, demonstrated globally impaired left ventricular systolic dysfunction. Intravascular ultrasound (IVUS) demonstrated the presence of mild atheroma in the LMS with mean luminal area of < 4 mm2. In view of medication-refractory, prolonged and frequent episodes of chest pain that involved the LMS, exposing significant amount of myocardium to risk, we decided to perform percutaneous coronary intervention (PCI) of the LMS, as a last therapeutic option. Informed consent was obtained from the patient. PCI was performed using 3.0 mm × 18 mm Xience® everolimus eluting stent (Abbott vascular, USA), which was post dilated with 3.5 mm non-compliant balloon at high atmospheres; stent expansion and apposition were confirmed by IVUS examination. Patient remained asymptomatic for 18 months, before experiencing recurrence of angina. The frequency and intensity of pain had become markedly less. Patient underwent CAG 3 years post index PCI, which demonstrated the stent in the LMS to be widely patent with no evidence of re-stenosis. However, distal segments of epicardial arteries demonstrated coronary spasm, responsive to intracoronary nitrate. Left ventricular systolic function was normal without any evidence of MR. Patient has also been commenced on trans-cutaneous electrical nerve stimulation (TENS), offering her symptomatic relief. |
||||||
|
||||||
DiscussionThis case demonstrates the various aspects and challenges associated with patients presenting with VA. Our patient presented with angina without any clear precipitating factors. The earlier coronary angiograph was reported normal whereas the one performed a decade later demonstrated presence of spasm in the LMS responsive to intra-coronary nitrate, but the absence of a flow-limiting CAD. She experienced symptoms in clusters with intermittent asymptomatic periods. She developed hoarseness of voice, which could be due to compression of or irritation of the recurrent laryngeal nerve from the enlargement of the pulmonary artery in the area between the aorta and ligamentum arteriosum.[5] Initially CCB and nitrates were adequate to control her symptoms, but eventually became less efficacious. Addition of nicorandil was beneficial for a brief period of time, but we were limited in using these medications due to its side-effects. Once we confirmed that the VA involved the LMS in our patient, resulting in MR due to ischemic left ventricular cavity dilatation, we decided to perform IVUS guided PCI. IVUS helped us understanding the underlying disease, determine the stent size and confirm post-PCI stent expansion and apposition. IVUS confirmed presence of mild atheroma, obscuring nearly 50% of the mean luminal area. VA can occur in the presence of underlying atheromatous coronary lesion. Repeated VA attacks can also induce hypo-cellular, fibro-fatty coronary lesion, or it can lead to neo-intimal proliferation that histo-pathologically mimics to restenosis.[6] Similar to these lesions, arteries with VA have been shown to have smooth muscle-like cell induced intimal hyperplasia[7] or functional medial thickening and folding of internal elastic lamina,[8] and IVUS may not be sensitive enough to differentiate between such lesions. In the pre-stent era, balloon angioplasty was attempted in pharmacotherapy refractory VA patients without much success.[9] Since the availability of stents, case reports and series are in literature suggesting their use in treatmentrefractory patients.[10,11] Stenting offers few benefits: It prevents coronary spams, avoids elastic recoil after balloon angioplasty alone and treats underlying atheroma. However, these benefits comes at the risk of in-stent restenosis[11] and the possibility of spasm related under-sizing of the stent or stent recoil, that poses patient to the risk of stent thrombosis, which can be fatal. In addition, VA can affect multiple segments of coronary circulation, and stenting one or more segments may not be enough to relieve symptoms completely.[11] Coronary artery bypass grafting (CABG) is a treatment option for those who experience treatment refractory VA in presence of obstructive atherosclerotic CAD. CABG can be performed with or without cardiac denervation.[11,12] Coronary spasm can persist post-CABG and result in significant hemodynamic compromise.[13] If CABG is performed in those without significantly CAD, long-term graft patency will be a concern. Overall CABG has shown to be beneficial in < 50% of patients.[14] In our case, we decided to perform PCI only when we observed transient, global severe left ventricular systolic dysfunction. Prolonged episode of VA can result in myocardial infarction, atrio-ventricular nodal conduction block, ventricular tachycardia, ventricular fibrillation or even death.[15,16] Stenting should be limited only to the patients who demonstrate significant hemodynamic or electrical instability at the time of VA attack. Post PCI our patient remained asymptomatic for 18 months and then experienced recurrence of angina. We performed repeat CAG to confirm that stent was well expanded, apposed to the vessel wall and free of in-stent restenosis. CAG demonstrated presence of spasm in distal segments of coronary circulation, similar to the observation reported by others.[11] Now her angina is less intense and controlled with the use of nitrate as well as TENS, a device that has shown to be beneficial in those with cerebral spasm after subarachnoid bleeding.[17] |
||||||
ConclusionOur case was unique in that patient had clusters of chest pain over more than 15 years with variable response to vascular smooth muscle dilators. PCI was performed only when we observed significant myocardium at risk. PCI can be an alternative therapeutic option, only once pharmecotherapeutic options are exhausted, and patient continues experiencing troublesome angina, which has to be guided by intra-coronary imaging. Possibility of in-stent restenosis, vasospasm induced stent recoil or under-sizing of the stent should be kept in mind, as if missed can have life-threatening consequences. |
Subscribe now for latest articles and news.