Journal of Medical Sciences and Health
Year: 2022, Volume: 8, Issue: 2, Pages: 166-172
Case Series
Sheela Mathew1 , Aquil Kalanad2 , Muhammed Masood Khan3 , Anees Mullappally Abdul Hameed3 , Anusha Sathyapal3 , Paramesh Mohankumar3
1 Professor, Infectious Diseases, Government Medical College Hospital, Kozhikode, Kerala
2 Assistant Professor Department of Medicine, Government Medical College Hospital, Kozhikode, Kerala
3 Junior Resident, Department of Medicine, Government Medical College Hospital, Kozhikode, Kerala
Address for correspondence:
Sheela Mathew, Professor, Infectious Diseases, Government Medical College Hospital, Kozhikode, Kerala.
E-mail: [email protected]
Received Date:21 January 2022, Accepted Date:23 June 2022, Published Date:03 September 2022
Following COVID -19 infection people are prone for developing bacterial, viral and fungal infections. The main reasons highlighted for increased susceptibility to infection are severe COVID -19 infection and use of immune suppressants. We had 3 cases of cryptococcal meningitis where two patients had mild COVID -19 and one had asymptomatic COVID -19. Evaluation for immune suppression revealed persisting pan lymphocyte depletion in one patient, isolated CD4 depletion in second patient and underlying HIV infection in the third patient with a very low CD4 count of 11 which was totally asymptomatic till then. Cryptococci is a ubiquitous pathogen and both innate and adaptive immunity is important in eradicating infection. COVID -19 per se as well as the various treatment modalities given in COVID -19 infection disrupts the immune system making people vulnerable for opportunistic infections. Even mild COVID -19 infection can predispose such diseases. A brief description of innate and acquired immune mechanisms preventing cryptococcal infection and how this is altered in COVID -19 infection is highlighted in this article. Post COVID patients when come with infections, unusual pathogens also should be considered. Unusual infection when occur in immune competent people, asymptomatic COVID -19 infection should also be ruled out.
Keywords: CD4 cytopenia, Pan lymphocyte depletion, Cryptococcal meningitis, Cryptococcus, Covid 19 infection
Cryptococcus is a basidiomycete yeast that includes more than 30 species. However, the majority of human infections are caused by Cryptococcus neoformans (C. neoformans) and Cryptococcus gatti (C. gatti). Cryptococcosis is an invasive fungal infection caused by C. neoformans or C. gatti. C. neoformans is ubiquitous in soil contaminated with pigeon or chicken droppings. It is an encapsulated yeast, which is the asexual form, and it reproduces by budding. A large majority of the population is exposed to C. neoformans, but most of the infections are asymptomatic. However, infections can persist in a latent stage, which can be reactivated when the host immune system is compromised. The most common manifestation is meningoencephalitis. Pneumonia, skin lesions, and involvement of bone, liver, lymph nodes, urogenital tract, and adrenal glands are other, although rare, manifestations. The prostate serves as a reservoir for infection. The common underlying immune suppression includes human immunodeficiency virus (HIV) infection, solid organ transplantation, immunosuppressive therapy, sarcoidosis, genetic immune deficiency syndrome, haematopoietic malignancies, cancer chemotherapy, and hepatic failure. 1 Cases of cryptococcal meningitis in immunocompetent patients are rarely reported. Those with HIV infection are commonly affected by C. neoformans, whereas C. gatti typically infects immunocompetent individuals. 2
The organism enters the human respiratory tract via inhalation and multiplies in the pulmonary alveoli. 3 The organism has a tropism for the central nervous system (CNS) because cerebrospinal fluid (CSF) has very low complement activity and is a favourable medium for replication. In the serum, organisms activate alternate complement pathways, thereby inhibiting cryptococcal growth. The organism produces mannitol, which can cause brain oedema and inhibit phagocytes. 4 Compared to bacterial meningoencephalitis, inflammation in cryptococcal meningoencephalitis is mild, with diffuse involvement of the brain. Occasionally, localized cryptococcomas can occur.
The clinical presentation of cryptococcal meningoencephalitis varies. Patients can present with long-standing symptoms lasting several months, or can present with acute illness lasting a few days. However, the majority of patients have a sub-acute onset. Fever (in less than 50% of patients), headache, lethargy, personality changes, visual disturbances, and memory loss are observed. According to Hussain et al, the time of onset of cryptococcal meningoencephalitis in solid organ transplant recipients was 21 months after transplantation. 5 Additionally, the type of immunosuppressive agent was found to influence the predominant clinical manifestations; CNS infection was observed predominantly in non-tacrolimus-based immunosuppression. 5 Liver transplant recipients have a higher risk of disseminated cryptococcal infections with fungemia. 5
Cryptococcal meningitis should be suspected in immunocompromised patients with fever, headache, or any central nervous system symptoms or signs. Immunocompetent patients with subacute or chronic meningitis should also be evaluated for cryptococcal meningitis. A definite diagnosis can be established with CSF study. If the patient has focal neurological deficits, lumbar puncture (LP) should be performed only after imaging. The opening pressure is usually high, but when compared to HIV-positive patients, HIV-negative patients do not show much elevation. Cell count is increased, and mononuclear cells predominate in both HIV and non-HIV patients. Elevated protein and low sugar levels are other features. India ink stain shows encapsulated yeast, and fungal culture yields growth in 3–5 days. Additionally, cryptococcal antigen can be detected with latex agglutination assay, enzyme-linked immunosorbent assay, or lateral flow assay.
Similar to other infections, both the innate and adaptive immune systems play a role in the regulation of cryptococcal infections. In the nonspecific innate immune responses, phagocytic cells and complement systems are major players in addition to physical barriers, such as skin and nasal mucosa. Upon entering the lungs, yeasts are recognised by host innate immune cells, such as dendritic cells and alveolar macrophages, which ingest and destroy invading cryptococci. Epithelial cells and endothelial cells also act as physical barriers. Moreover, endothelial cells augment the activity of polymorphs. 2
Adaptive immunity plays a major role in overcoming cryptococcal infection. Although cryptococci are facultative intracellular pathogens, antibody-mediated immune mechanisms are also required for effective clearance. This is supported by the fact that cryptococcal infections occur in primary or acquired B cell defects. In addition, antibodies against cryptococcal polysaccharides and proteins are seen in individuals without an active infection, suggesting latent, asymptomatic, or cleared infections. 2
The increased occurrence of cryptococcal meningitis in HIV patients, steroid recipients, transplant recipients, and leukaemia and lymphoma patients suggests that cell-mediated immunity plays a major role in the progression of infection. 6 CD4+ cells, CD8+ cells, natural killer (NK) cells, and NKT cells exert antimicrobial activity against cryptococci. CD4+ and CD8+ cells produce granulysin, a pore-forming protein that helps in cryptococcal clearance. 7 In addition, they produce pro-inflammatory cytokines that recruit and activate other phagocytes to kill cryptococci. Perforin is the main mediator of NK cell effectiveness in cellular killing. 8 In addition to direct killing, cytokine-mediated killing is also important for fungal clearance. Both interferon gamma (IFNγ) and tumour necrosis factor α (TNFα) play a role in fungal clearance. Regulatory T cells promote protection against cryptococci by suppressing detrimental Th2 immune responses. γδ T cells are also involved in the protective immune response against cryptococci. IFNγ in the Th1 response induces the development of classically activated macrophages (M1-type) which are associated with intracellular killing and protection against cryptococci. Interleukin 4 (IL-4) in the Th2 response induces alternatively activated macrophages (M2) which favour intracellular replication and leads to further progression of the infection.
Antigen-presenting cells in the lungs carry the cryptococcal antigen to draining lymph nodes, inducing the proliferation of CD4+ and CD8+ cells. CD4+ cells differentiate into effector subsets with unique cytokine profiles, including Th1, Th2 and Th17 cells. The host T helper subset and its associated cytokines are important in the progression and outcome of cryptococcal infection; Th1 and Th17 profiles are associated with clearance of cryptococcal infection, while Th2 profiles are associated with cryptococcal dissemination. Once active, CD4+ T cells promote B cell proliferation, activation of macrophages, and proliferation of CD8+ cells, thus facilitating effective fungal clearance. 2
Lymphopenia has been described from the very beginning of the COVID-19 pandemic as an associated marker of COVID-19 infection. 9 The severity of COVID-19 infection was reported to be directly linked to the severity of lymphopenia, especially in the elderly population. Influences of pro-inflammatory cytokines, such as TNF-α and IL-6, virus-induced suppression of T cell and NK cell cytotoxic activities, exhaustion of CD4+ and CD8+ cells, T cell invasion, and interference in T cell expansion by SARS-CoV-2, are well described; these essentially impair the qualitative and quantitative function of lymphocytes. 9
Case 1 — A 55 yr old female was admitted with a history of headache, irregular fever and vomiting of one-month duration followed by altered behaviour for a week. She was absolutely healthy prior to the onset of symptoms. There was no prior history of COVID-19 infection, and she was not vaccinated against COVID-19. General examination showed a confused patient (12 on the Glasgow Coma Scale) and central nervous system examination showed neck stiffness. All other systems were normal. LP was performed (Table 1). CSF culture had C. neoformans growth and liposomal amphotericin B was initiated. On day 11 of amphotericin administration, the patient developed papular eruptions over the chest and back with associated itching. Amphotericin was stopped, and fluconazole 800 mg tablet was started. Her CBC showed persistent lymphopenia (Table 1).
|
Investigations |
Day 1 of admission |
Day 3 |
Day 7 |
Day 30 |
|
Hemoglobin, g/dL |
9.3 |
8.2 |
8.5 |
|
|
Total leukocyte count(per μL) |
14300 |
13070 |
10600 |
7300 |
|
Differential Count (%) |
P86, L9, M5 |
P87, L7, M6 |
P93, L5, M2 |
P76, L20, M4 |
|
Platelet(x105 per μL) |
5.79 |
4.60 |
2.72 |
2.79 |
|
ESR (mm/hr) |
110 |
|
|
75 |
|
Serum CRP, mg/L |
49 |
|
41 |
|
|
Urea(mg/dL) |
32 |
10 |
10 |
|
|
Creatinin(mg/dL) |
0.5 |
0.5 |
0.5 |
|
|
Serum Sodium, mEq/L |
130 |
|
|
|
|
Serum Potassium, mEq/L |
3.4 |
|
|
|
|
LFT |
Normal |
|
|
Normal |
|
Blood Glucose, mg/dL |
177 |
|
|
128 |
|
HbA1c % |
5.8 |
|
|
|
|
CSF |
|
|
|
|
|
Opening pressure |
150 mm H2O |
|
|
|
|
Protein |
150mg/dL |
|
|
|
|
Sugar |
48mg/dL |
|
|
|
|
Cells |
50/µL, N70%, L30% |
|
|
|
|
|
|
|
|
|
|
India ink stain |
Fungal yeast seen |
|
|
|
|
Fungal culture |
Cryptococci grown |
|
|
|
|
HIV / HBsAg / HCV ELISA |
Negative |
|
|
|
|
CD3 |
333 (Normal 570-2400/cu.mm) |
|
|
|
|
CD4 |
234 (430-1800/cu.mm) |
|
|
|
|
CD8 |
99(210-1200/cu.mm) |
|
|
|
|
CD19 |
27 (91-610/cu.mm) |
|
|
|
|
CD56 |
63 (78-470/cu.mm) |
|
|
|
Chest radiography and ultrasonography findings were normal. In view of persistent lymphopenia, a COVID-19 antibody test was performed and was found positive. Lymphocyte subset analysis performed using flow cytometry showed absolute lymphocytopenia. The patient responded to fluconazole treatment and was discharged on fluconazole. On one-month follow-up, her CBC was returning to normal and her lymphocyte count was also improving.
Case 2 — A 47 yr old male who had a category A COVID-19 infection two months back, was admitted with a history of headache and vomiting for 1 month. On examination, he was conscious but disoriented. His pulse rate was 68 beats/min, blood pressure was 110/70 mm Hg, and saturation was 99% in room air. The systemic examinations were within normal limits, except for neck stiffness.
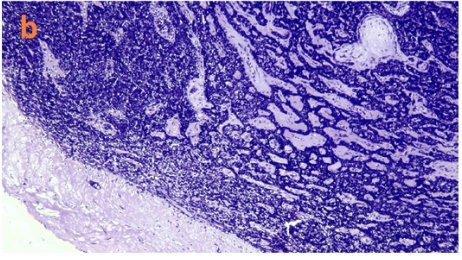
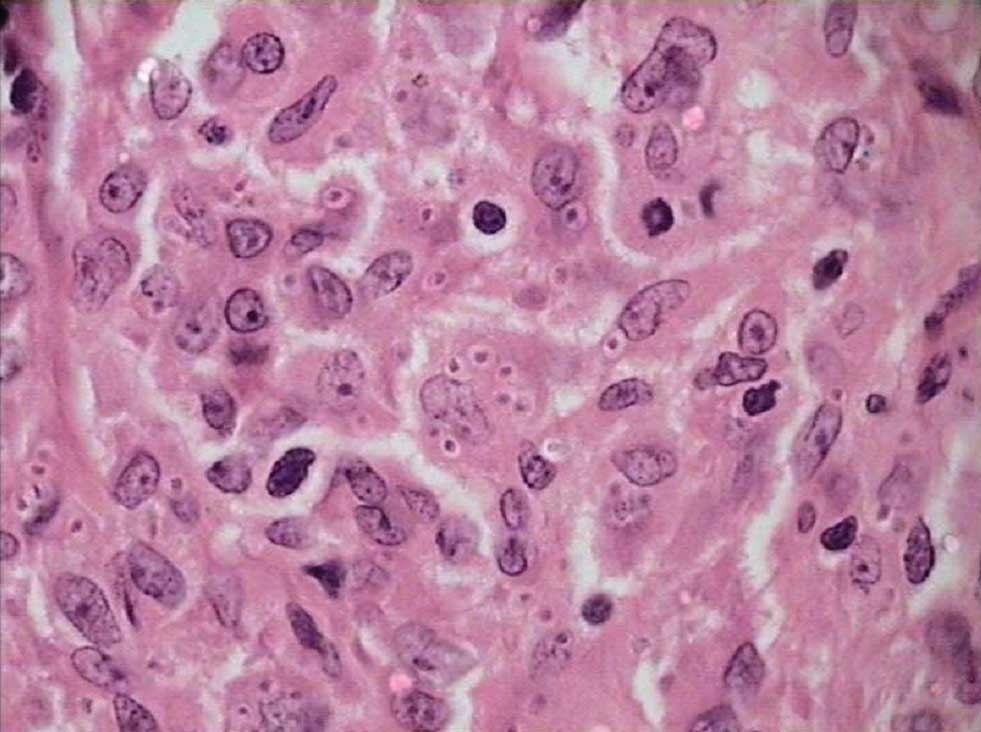
LP was performed and the opening pressure was low. Cell count showed lymphocytosis. Protein levels were high, while sugar levels were low (Table 2). India ink preparation showed cryptococci. CSF Gram staining showed gram-positive round budding yeast, and CSF cryptococcal antigen was also positive. CSF culture yielded cryptococci (Figure 1).

|
Investigations |
Day 1 admission |
Day 3 |
Day 7 |
Day 20 |
|
Hemoglobin, g/dL |
11 |
8.2 |
8.3 |
8.8 |
|
Total leukocyte count (per μL) |
5800 |
4900 |
4000 |
4200 |
|
Differential Count (%) |
N80,L11,M9 |
N82, L9,M9 |
|
|
|
Platelet(x105 per μL) |
0.48 |
0.05 |
0.12 |
0.95 |
|
ESR (mm/hr) |
14 |
|
|
|
|
Urea (mg/dL) |
32 |
10 |
10 |
10 |
|
Creatinin(mg/dL) |
0.5 |
0.5 |
0.5 |
0.8 |
|
Serum Sodium, mEq/L |
130 |
|
|
134 |
|
Serum Potassium, mEq/L |
3.4 |
|
|
3.9 |
|
LFT |
Normal |
|
|
Normal |
|
Blood Glucose, mg/dL |
99 |
110 |
|
128 |
|
Hb A1c ( %) |
5.8 |
|
|
|
|
HIV / HBsAg / HCV ELISA |
Negative |
|
|
|
|
CSF Opening pressure Protein Sugar Cells India ink stain Fungal culture |
Day 1 100 cm H2O 290mg/dL 8mg/dL NIL Fungal yeast seen Cryptococci grown |
Day 14 110 cm H2O 275mg/dL 34mg/dL 117/µL L 80, N20 Few yeast cells seen No growth in culture |
|
|
|
CD3 CD4 CD8 CD19 CD56 |
312 (Normal 570-2400/cu.mm) 34 (430-1800/cu.mm) 254 (210-120/cu.mm) 149 (91-610/cu.mm) 86 (78-470/cu.mm) |
|
|
|
The patient was started on liposomal amphotericin B, but his cell count started to decline, hence, he was switched to fluconazole 800 mg. Peripheral smear examination showed thrombocytopenia and bone marrow examination showed focal megaloblastic changes, hence, vitamin B12 supplementation was initiated. The patient showed significant improvement. Since the patient had cryptococcal meningitis, he was evaluated for immunosuppression. A CD4+ cell count of 55 was noted. HIV antibody test and HIV RNA polymerase chain reaction were negative. Because CBC showed persisting lymphopenia one month after COVID-19 recovery, lymphocyte subset analysis was performed (Table 2). In view of profound CD4+ cell depletion, cotrimoxazole prophylaxis was initiated. The patient had hyponatraemia during hospitalisation, which improved with treatment. Magnetic resonance imaging showed a leptomeningeal enhancement and contrast-enhancing lesion over the left hemi-pons, suggestive of cryptococcoma. IgG Toxoplasma test results were negative. The patient showed a good response to the treatment.
Case 3 — A 49 yr old female was admitted with a history of headache of 2 weeks’ duration. She initially received analgesics from a local hospital. The patient had a category A COVID-19 infection, one month prior to the onset of headache, and was quarantined at home. Physical examination revealed an obese, delirious patient. Examination of skin showed scar marks of exaggerated insect bite reaction. CNS examination revealed right lateral rectus palsy and neck stiffness. LP was performed, and both opening pressure and cell count were high, protein level was elevated, and sugar was low, corresponding to blood sugar (Table 3). CSF gram staining revealed gram-positive yeasts, and India ink showed numerous cryptococci with negative staining capsules. The patient’s HIV test result was positive, and the CD4+ count was very low. The patient was initiated on intravenous amphotericin and flucytosine along with anti-oedema measures but succumbed to the illness on the 4th day of hospitalisation. There was no evidence of any other opportunistic infection.
|
Investigations |
|
|
Hemoglobin, g/dL |
9.5 |
|
Total leukocyte count (per μL) |
3200 |
|
Differential Count (%) |
N72,L24,M4 |
|
Platelet(x105 per μL) |
1.20 |
|
ESR (mm/hr) |
78 |
|
Urea (mg/dL) |
24 |
|
Creatinin(mg/dL) |
0.84 |
|
Serum Sodium, mEq/L |
32 |
|
Serum Potassium, mEq/L |
4.2 |
|
LFT |
Normal |
|
Blood Glucose, mg/dL |
169 |
|
HIV HBsAg / HCV ELISA |
Positive Negative |
|
CSF Opening pressure Protein Sugar Cells India ink stain Fungal culture |
280 cm H2O 100 mg/dL 49mg/dL 1500/micro L All lymhocytes Fungal yeast seen Cryptococci grown |
|
CD4 |
11/cu.mm |
Following the COVID-19 pandemic, the world of infectious diseases has changed into pre-COVID and post-COVID eras. The aetiology, pathophysiology, and clinical spectrum of various clinical syndromes has changed after the COVID-19 pandemic. Each syndrome complex should be approached with a broad spectrum of differential diagnoses and clinical investigations should be planned accordingly.
In this study, we describe three cases of cryptococcal meningitis which presented with fever, headache, and altered behaviour. On evaluation, only one patient had a classical predisposing condition, in this case HIV infection, which was diagnosed while evaluating meningitis. HIV alters Th1 Th2 balance with higher IL4 activity than IFNγ. Additionally, CD4+T cell granulysin-mediated killing of cryptococci does not occur in HIV infection. 6, 7 Even with a very low CD4+ count, the patient was asymptomatic. Whether preceding COVID-19 has any role in precipitating this opportunistic infection by rapidly depleting CD4 cells is yet to be determined. During this pandemic, we observed that Pneumocystis pneumonia also precipitated soon after COVID-19 infection in asymptomatic HIV-infected individuals. CD4+ count less than 50 is a high-risk factor for severe cryptococcal meningoencephalitis with high fatality. Other predictors of poor outcome include high CSF cryptococcal antigen level (titre> 1:1024 by latex agglutination assay, > 1:4000 by lateral flow assay), low body weight, poor CSF inflammatory response (< 20 cells/µL), and altered mental status on presentation. 10 An abnormal mental status indicates increased intracranial pressure.
The other two patients did not present with any described risk factors for cryptococcal meningitis. One of them had isolated CD4+ cytopenia and the other had pan-lymphocytopenia due to COVID-19 infection. To date, there have been no reports regarding the average duration of lymphopenia in post-COVID-19 patients. Hence, these patients were kept under follow-up. Patient with CD4+ cytopenia had a normal lymphocyte count after two months of follow-up.
Qin et al. demonstrated a dysregulated immune system in a cohort of 452 patients with COVID-19 infection. The major observation in the study was profound lymphopenia, and a reduction in CD4+ lymphocyte count was more evident in severe cases. However, no significant change in the number of CD8+ and B cells was noted. Moreover, they reported that the percentage of naïve helper T cells increased, while the number of memory helper T-cells, suppressor T-cells, and Treg cells decreased. The authors concluded that the reduction in the immune response resulted in excessive inflammation, a characteristic of severe COVID-19 infection. 11 On the contrary, the patients described in the present study did not have severe COVID-19 infections and did not require hospitalisation. Hence, there is a possibility that even mild cases of COVID-19 can develop lymphopenia and serious opportunistic infections.
COVID-19 infection dysregulates the immune system, and the extent is still not fully understood. The associated therapy-induced suppression, such as steroid and tozulizumab, is highlighted more frequently. Common viral, bacterial, and fungal infections can occur due to the use of immunosuppressants in COVID-19 infections. However, all three patients in this series were not on immunosuppressants and two had only mild COVID-19 infection, while one was asymptomatic. Hence, we suggest that post-COVID-19 patients should be vigilantly monitored for opportunistic infections which are not usually considered in ordinary people.
Only very few cases of cryptococcal meningitis have been reported in the post-COVID-19 individuals. One report was of a patient with renal transplant with decompensated cirrhosis and COVID-19 in whom Cryptococcus was identified in the blood and ascitic fluid 12. Another report was on a patient with cryptococcemia in COVID-19 infection, who received tozulizumab and steroids at a high dose. 13 The patients described in the present study did not have an underlying immunosuppressed state, except for one patient who had HIV. Hebah et al. reported a case of severe cryptococcal meningitis that developed in a previously healthy patient one week after treatment of SARS-CoV-2 infection with dexamethasone. 14 Diana Alegre-González et al. also reported a case of disseminated cryptococcal infection following severe COVID-19 infection treated with immunosuppressants. 15
To maintain normal immunity in any person, a balanced CD4+/CD8+ ratio, and Th1, Th2, and Th17 responses are needed. Any alternation renders the person at risk for various infections, including opportunistic infections. COVID-19, by itself, is well known to produce a disequilibrium of immunity and hence is associated with increased vulnerability to numerous infections. Moreover, various drugs used for severe infections also result in immune suppression. This factor should be considered when following up on post-COVID-19 patients. In addition, when unusual infections occur in the normal population, even if a history of COVID-19 is not obtained, a post-COVID-19 state should be ruled out by performing an antibody test, if the individual is not vaccinated. Previous reports have highlighted the reversal of immune suppression following recovery from COVID-19 infection, but the patients described in the present study showed persistent lymphopenia. This factor highlights the significance of prolonged observation of post-COVID-19 individuals, and further studies are needed in this regard to determine the duration of persistent lymphopenia in post-COVID-19 infection.
Subscribe now for latest articles and news.