Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.v9i3.23.219
Year: 2023, Volume: 9, Issue: 3, Pages: 355-357
Case Report
Sucheta Bansal1 , Brijesh Thakur1 , Sanjay Sadhu2 , Sadaf Khan1
1Department of Pathology, Shri guru ram rai institute of medical and health sciences, Dehradun, Patel Nagar, 248001, Uttarakhand, India,
2Department of Plastic Surgery, Shri guru ram rai institute of medical and health sciences, Dehradun, Patel Nagar, 248001, Uttarakhand, India
Address for correspondence:
Sucheta Bansal, Department of Pathology, Shri guru ram rai institute of medical and health sciences, Dehradun, Patel Nagar, 248001, Uttarakhand, India.
E-mail: [email protected]
Received Date:11 August 2023, Accepted Date:19 December 2023, Published Date:28 December 2023
Inflammatory linear verrucous epidermal nevus (ILVEN) is a rare variant of epidermal nevus characterized by psoriasiform epidermal hyperplasia, pruritic, warty lesions, in a linear configuration, following the lines of Blaschko. We report a rarer incidence of ILVEN in a young adult female presented with pruritic linear focally warty lesion over dorsum of right foot since birth. Histopathological examination of excision biopsy was suggestive of ILVEN. Although generally considered benign, 15-20% ILVEN cases can show malignant transformation. Despite variable treatment options, treatment is custom-made depending upon the nature and extent of the lesion. Therefore, the correct diagnosis of ILVEN is vital for choosing early and prompt treatment planning.
Keywords: Adult, ILVEN, Female, Epidermal, Nevus
Epidermal nevus is a cutaneous hamartoma or congenital malformation of the epidermal cells. Inflammatory linear verrucous epidermal nevus (ILVEN) is a rare variant of epidermal nevus characterized by psoriasiform epidermal hyperplasia, pruritic, warty lesions, in a linear configuration, following the lines of Blaschko i.e. embryonic lines situated along the planes of ectodermal cleavage 1. About 75% of these cases present during the first five years of life, most often in the first 6 months 1. Although uncommon, cases with adult onset have also been reported. Typically, these lesions are unilateral, show female preponderance (4:1) 2, 3. Incidence of ILVEN is estimated to be 1-3 neonates/1000 live births 3.
Here, we describe a rare presentation of ILVEN in a 25 years old female from a hilly region.
A 25-years-old female presented to the plastic surgery OPD with erythematous, scaly, pruritic, linear plaque over the dorsum of right foot, which was progressively increasing and present since birth (Figure 1 a). On systemic examination, no other associated abnormality or similar lesion over other sites was noticed. No significant past medical and family history was documented. Routine investigations were within normal limits. Surgical excision of lesion was planned.
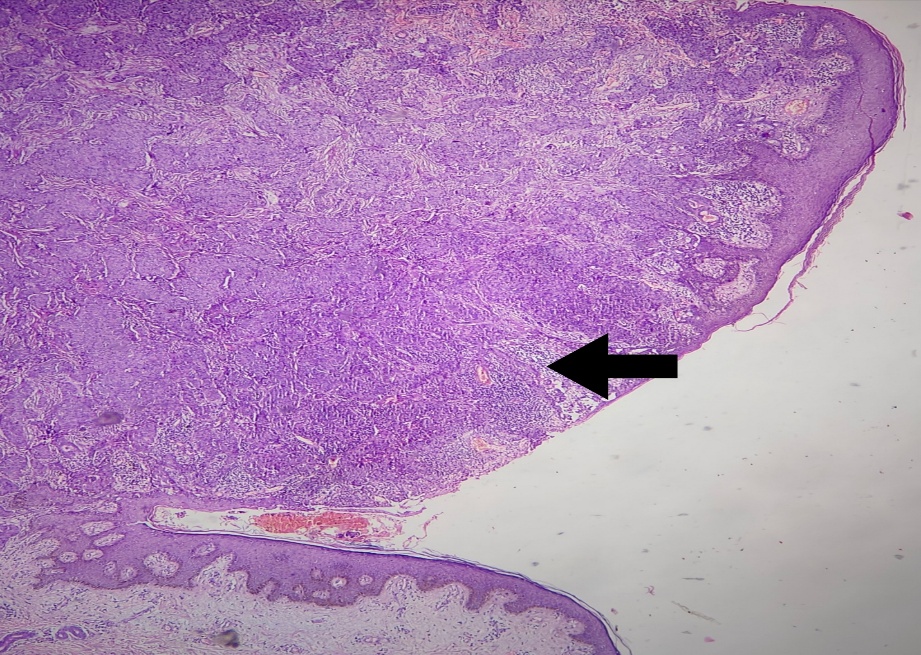
Excised skin covered lesional tissue piece measuring 4.5x2.0x1.0 cm. was received for histopathological examination. Skin surface showed verrucous areas grossly. Representative sections were taken and processed as per standard laboratory protocol. Microscopic examination revealed epidermis exhibiting hyperkeratosis, psoriasiform hyperplasia, papillomatosis, regular acanthosis and elongation of rete ridges (Figure 1 b). Vertical tiers of parakeratosis, orthokeratosis and alternating hypergranulosis as well as hypogranulosis were present (Figure 1 c & d). Focal intracorneal pustules and areas of suprapapillary thinning were noted (Figure 1 e). There was presence of moderate interface lymphoplasmacytic inflammatory infiltrate, along with mild perivascular infiltrate in the reticular dermis. Morphological diagnosis of ILVEN was considered. She had an uneventful follow up period of 2 months till the commencement of this case report.


ILVEN was initially described by Unna in 18962, 3 which constitutes approximately 6% of all epidermal nevi 4. The classic clinical criteria for diagnosing ILVEN was first given by Altman and Mehregan in 1971 and subsequent modifications came from Morag and Metzker in 1985 4, 5. These characteristics include early age of onset, predominance in females, frequent involvement of the left lower limb, pruritus and distinctive psoriasiform appearance, and resistance to therapy 3, 6.
It is usually sporadic; however familial cases have also been reported 1, 2. Although its exact etiology is still debatable, ILVEN is thought to be caused by somatic heterozygous mutations of GJA1, a gene encoding a gap junction protein and also known as connexin 43. The GJA1 gene mutations result in genetic mosaicism and upregulation of interleukin 1, interleukin 6, tumor necrosis factor α, and intercellular adhesion molecules 3, 4, 5. Sanger sequencing of the affected epidermis or immunohistological analysis using anti-GJA1 antibody can be done to detect these mutations. Exposure to ultraviolet rays and chemical carcinogens has been implicated as potential risk factors 3.
Clinically, it presents with pruritic, erythematous and verrucous papules, in a linear distribution following Blaschko’s lines. Lesions are usually unilateral and solitary, most often on the lower half of the body; especially lower limb, as seen in our case 7. Some authors also described more frequent left sided involvement 6, however, the same was not in our case. The length of the lesion is variable, although confined, but in some cases it may be extensive or multifocal. Genital or mucosal involvement are rather rare but have been reported 2, 3.
The lesions usually show a chronic and progressive course characterized by periodic inflammatory breakthroughs associated with increased pruritus and rarely with superadded infections. The disease can stabilize or may show a spontaneous regression. These ILVEN’s have been seen associated with skeletal-articular defects, CNS deformities and visceral hypoplasias, which are usually ipsilateral 2, 3.
Histological features include hyperkeratosis, acanthosis, papillomatosis, with a psoriasiform epidermal hyperplasia or even Munro’s micro-abscesses. Some cases show focal thickening of the granular layer with columns of parakeratosis. Basal layer can occasionally show increased melanin pigment, correlating clinically with the tan or brown-colored lesions. Characteristically, a sharply demarcated alternation of parakeratosis and orthokeratosis is seen in the cornified layer. The parakeratotic areas are slightly raised overlying agranular/hypogranular layer, while the orthokeratotic areas are relatively depressed with underlying hypergranulosis 7, 8. All these findings were well appreciated in our case. More importantly, the lesional margins are sharply demarcated from the adjacent normal epithelium on microscopic examination 3, 6.
Although generally considered benign, 15-20% i.e. 1 in 5 affected individuals of ILVEN can show malignant transformation 3. Basal cell carcinoma, squamous cell carcinoma and keratoacanthoma have been reported to develop in these lesions 3, 6. This is heralded by rapid growth or superficial ulceration of the lesion.
Clinically, ILVEN can mimic linear Darier disease, linear porokeratosis, linear lichen planus, linear psoriasis, and the verrucous stage of incontinentia pigmenti, other epidermal nevi, nevoid psoriasis, and lichen striatus 1, 2. In contrast to the linear epidermal nevus, lesions are usually erythematous and pruriginous. Spontaneous regression and absence of pruritus distinguish ILVEN from lichen striatus. ILVEN is often difficult to differentiate from psoriasis. The orthokeratotic areas show increased involucrin expression while parakeratotic areas are negative for involucrin stain, this pattern of staining helps in differentiating the ILVEN from psoriasis 1, 7. Psoriasis can occur in a nevoid forms, however, these are usually asymptomatic and typically respond to antipsoriatic treatment. Refractoriness to treatment is a defining feature of ILVEN.
Although, diagnosis of ILVEN is interesting, it is challenging from a dermatologist point of view; as there are no absolute effective medical therapies available. Wide range of therapeutic options includes topical corticosteroids, dithranol and retinoids, topical vitamin D analogues, 5-FU and calcineurin inhibitors 1. Physical modalities include surgical excision, cryotherapy, photodynamic and laser therapy, and are considered better by some dermatologists 2.
Despite variable treatment options, treatment is custom made depending upon the nature and extent of the lesion. Therefore, the correct diagnosis of ILVEN is vital for choosing early and prompt treatment planning.
Subscribe now for latest articles and news.