Introduction
Fused kidneys are congenital anomalies that arise due to abnormalities in position, ascent, rotation, or vascular supply of kidneys, which can manifest as partially fused kidneys (e.g., horseshoe kidney) or completely fused kidneys (cake kidney, pancake, lump kidney, disc kidney, etc.) 1 Crossed fused renal ectopia results when the kidney fuses on the side opposite to the opening of its ureter into the urinary bladder. A Tandem kidney/L-shaped kidney is a form of crossed fused renal ectopia in which the transversely positioned ectopic kidney crosses the midline and merges with the lower pole of the normal kidney.2 Crossed fused renal ectopia can occur with cardiovascular, genitourinary, musculoskeletal, or gastrointestinal defects. This congenital defect has an occurrence of one in every 1000 live births. 3 Crossed renal ectopia is three times more common from the left to the right than from the right to the left. 4 The fusion abnormalities are of importance during surgical procedures while tracing the course of the ureter of the ectopic kidney and to avoid iatrogenic injuries.
Case report
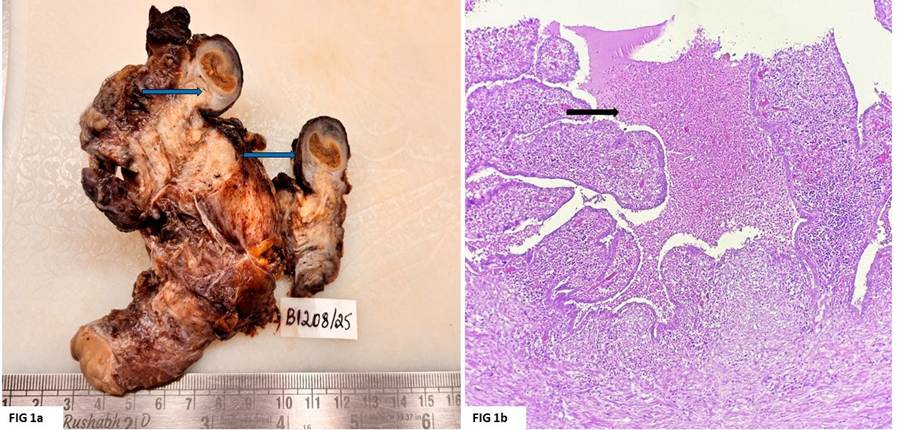
A 33-year-old female patient had abdominal discomfort and white vaginal discharge for the past two weeks. Abdominal tenderness was noted on physical examination and vital signs were normal. On ultrasonography, free fluid was discovered in the abdomen. The results of serum creatinine, and blood urea levels were within normal limits. The ultrasound confirmed the diagnosis of pelvic inflammatory disease (PID). Incidentally, the patient’s left kidney was found to cross the midline and fuse with the lower pole of the right kidney leading to the diagnosis of left crossed fused renal ectopia (CFRE) (Figure 1).

Discussion
Renal ectopia is a condition in which a kidney is present in a location other than its typical placement in the renal fossa of the posterior abdominal wall, which corresponds to vertebral levels T12-L3. Ectopic kidneys are frequently associated with malrotation. 3, 5
Crossed renal ectopia is an uncommon congenital anomaly in which a kidney moves across the midline to the contralateral side of the abdomen, first reported by Dominicus Pamaroulus in 1654. It has an estimated occurrence of 1 in 1000 live births, although its precise incidence is not known. It is largely an incidental finding when patients are evaluated for other conditions, or during antenatal or postnatal screening ultrasonography.6, 7, 8 85-90% of crossed renal ectopias appear fused either partially or fully with the contralateral kidney with a male preponderance. 8
Unilateral crossed renal ectopia, bilateral crossed renal ectopia, crossed fused renal ectopia, and crossed unfused renal ectopia are the four forms of crossed renal ectopia described in the literature. 3 Based on the relative position and site of fusion, there are six subtypes of crossed fused renal ectopia: 1. Inferior crossed fused renal ectopia - wherein upper pole of ectopic kidney fuses with the lower pole of normal kidney, 2. Superior crossed fused renal ectopia – the ectopic kidney is above the normal kidney, fuses with the upper pole of normal kidney, 3. Sigmoid or S-shaped kidney - hilum of ectopic kidney faces laterally while hilum of normal kidney faces medially. When fused, this appears like the letter 'S.' 4. Lump kidney - the kidneys have a broader margin of fusion than disc kidneys, and both renal pelvises face ventrally. 5. Disc kidney - significant fusion along the medial margins of the kidney, resulting in a disc-like shape. 6. Tandem kidney (L-shaped kidney) - the ectopic kidney is positioned horizontally. It represents the letter 'L' when it merges with the bottom pole of the orthotopic kidney.3 An anterior and/or posterior notch, two distinct collecting systems and empty contralateral renal fossa are characteristic ultrasonographic findings of crossed fused renal ectopias. 6, 7 (Figure 2) depicts the schematic representation of the classification of crossed renal ectopia and the subtypes of crossed fused renal ectopia.

Embryological Basis of Crossed Renal Ectopia
The kidneys ascend from the pelvis to the retroperitoneum on either side of the dorsal aorta during weeks 6 to 9 of intrauterine life. The blood supply is derived via the median sacral, internal iliac, common iliac, and dorsal aorta, which correlates to the level of ascension.3 Blood supply of the ectopic kidney originates more commonly from the contralateral side but can also arise from the ipsilateral side.7 As the ascent progresses, the caudal vessels degenerate. During weeks 6 to 9 of intrauterine life, the kidneys ascend and rotate ventromedially, such that the renal pelvis shifts from an anterior to a medial position.3 Both ascent and rotation take place simultaneously; non-ascent is commonly associated with non-rotation/malrotation of the kidney. The theories to explain crossed fused renal ectopia3 are:
-
Mechanical theory: During their cranial ascent, kidneys pass via the prongs of the two umbilical arteries. Any alteration in the position of the umbilical arteries might cause the kidneys to fuse.
-
The theory of abnormal caudal rotation: In scoliosis, due to lateral rotation of the embryo's caudal end, the ureter crosses the midline and is transpositioned next to the opposite nephrogenic blastema during kidney ascent.
-
The ureteral theory: According to this theory, the ureter is primarily responsible for crossed and fused kidneys. If the ureter migrates to the opposite side, it induces metanephric blastema on the crossed side to differentiate into kidneys. Under such circumstances, the metanephros of the normal side regresses due to a lack of induction.
-
Teratogenic theory: Teratogens have been associated with fused kidney anomalies, notably in a horseshoe kidney.
-
Genetic theory: The sonic hedgehog gene (Shh) is important for the positioning of the kidney. Disruptions in Shh gene regulation can cause renal fusion abnormalities.
|
Author name |
Crossed fused renal ectopia (CFRE) / Its subtype |
No. of cases / Ratio / Percentage |
|
Türkvatan et al. 2009 9 |
CFRE |
1:1300-1:7500, 0.08% - 0.01% |
|
Fused CFRE (85%) |
1:1000, 0.068% - 0.0085% |
|
|
Unfused CFRE (10%) |
0.008% - 0.001% |
|
|
Cake kidney |
<30 known cases till date |
|
|
L shaped kidney |
Two cases |
|
|
NeMoyer R et al. 2017 2 |
Left CFRE |
One case |
|
Unilateral CFRE |
1:75000 |
|
|
Sharma R et al. 2009 10 Solanki et al. 2013 |
Inferior CFRE |
One case Six cases |
|
Patel et al. 2008 Yin et al. 2014 Akdogan et al. 2015 5 |
Superior CFRE |
One case One case One case |
|
Babu CSR et al. 2015 3 |
Lump Kidney |
3 cadaveric dissections |
|
Pupca et al. 2014 Sharma V et al. 2014 |
L shaped kidney |
One case Two cases One case |
|
Rahim et al. 2020 8 |
CFRE with fused supernumerary kidney |
One case 1:26750 |
In 50% of cases of renal agenesis or ectopia, the "Lying down" adrenal sign is observed, in which the adrenal gland appears flattened and lies down on the psoas major muscle, in contrast to its typical inverted V or Y shape (visualized by ultrasonography). Renal dysplasia which occurs after the glands have developed normally under appropriate pressure from the once growing kidneys has been hypothesized to be the reason for the typical form of the adrenal gland.11 The heterotopic kidneys are usually hypoplastic and hypofunctional compared to their orthotopic counterparts.6, 7 Adrenal glands appear to be normal in this case of the tandem kidney.
Crossed fused renal ectopia can be associated with urinary and extra-urinary abnormalities such as anorectal anomalies (imperforate anus), vaginal agenesis, penile duplication, cryptorchidism,6 intestinal malrotation, VACTERL association (vertebral defects, anal atresia, cardiac defects, tracheoesophageal fistula, renal anomalies, and limb abnormalities), and TAR syndrome (Thrombocytopenia with the absence of Radius),3 meningomyelocele, spinal cord tethered syndrome, etc. Double nutcracker syndrome has been found to be associated with the tandem kidney.1 In this condition, the renal veins wrap the abdominal aorta anteriorly and posteriorly. A case of a tandem kidney was associated with venous malformation of the right internal iliac vein and right external iliac vein draining independently into the left common iliac vein.4 Most renal abnormalities can be evaluated using Multi-Detector Computed Tomographic (MDCT) urography.9
Renal complications such as vesicoureteral reflux, urinary tract infection, calculus, hydronephrosis, megaureter, ureteropelvic junction obstruction,6 cystic dysplasia, neoplasms such as Wilm's tumor, transitional cell carcinoma, and renal cell carcinoma are predisposed by crossed renal ectopias.6, 10 Crossed fused renal ectopia should be examined and followed upon to better patient care and minimize complications. Timely intervention and management personalized based on the patient’s presenting symptoms and complications lead to better patient outcomes. 6, 7