Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.2021.v07i02.009
Year: 2021, Volume: 7, Issue: 2, Pages: 47-60
Original Article
Preeti Kore1 , Renuka Metgud2 , Harpreet Kour3 , Preeti Bhupali4 , Snehal Dharmayat5 , Meenakshi Maste6 , Neha Dhaded7
1 Professor and Head, Department of Conservative Dentistry and Endodontics, KLE VK Institute of Dental Sciences, Kaher, Belagavi,
2 Professor, Department of Periodontics, KLE VK Institute of Dental Sciences, Kaher, Belagavi,
3 Assistant Professor, Department of Physiology, J.N Medical College, Kaher, Belagavi,
4Professor, Department of Medical Surgical Nursing, KLEU Institute of Nursing Sciences, Belgaum,
5 Associate Professor, Department of Community Based Rehabilitation, Kaher Institute of Physiotherapy, Belagavi,
6 Associate Professor, Department of Pharmaceutical Chemistry, KLE College of Pharmacy, Belagavi,
7 Reader, Department of Conservative Dentistry and Endodontics, KLE VK Institute of Dental Sciences, Kaher, Belagavi
Address for correspondence:
Dr. Harpreet Kour, Assistant Professor, Department of Physiology, J. N. Medical College, KLE Academy of Higher Education and Research, Nehru Nagar, Belagavi - 590 010, Karnataka, India. Phone: +91-9620850326. E-mail: [email protected]
Background and Objectives: Breast cancer is a global health concern. This study was conducted to assess the knowledge, beliefs, and awareness of breast cancer as well as to assess the knowledge on breast selfexamination (BSE) and clinical breast examination (CBE) in Belagavi.
Methods: The questionnaire-based pilot study was conducted among 20–70 years aged females without any history of breast cancer from rural and urban areas of Belagavi. Information about knowledge and beliefs about breast cancer was collected with a pre-tested, semi-structured questionnaire. Findings of BSEs and CBEs were recorded. Sample size for this pilot study was taken as 5% of the total sample size and therefore, 207 female staff from various educational institutions and a teaching hospital was enrolled for the study. Data were analyzed using the Chi-square test. P < 0.05 was considered statistically significant.
Results: Awareness of breast cancer was five-folds higher in urban than in rural areas. The odds of perception about breast cancer was 4.90 (confidence interval [CI] = l 2.2, 10.94) times higher in the urban than in the rural area. Similar results were seen for the BSEs with an odds ratio of 5.03 (CI = 1.18, 21.30).
Conclusion: Women from urban areas of Belagavi have a fair knowledge and awareness about breast cancer and are also fairly well versed with BSE technique. More awareness about breast cancer, its evaluation and need for early intervention need to be created among the rural population.
KEY WORDS: : Breast Cancer Awareness, Self-breast examination, Clinical Breast Examination
Breast cancer is the most common type of cancer among Indian women with age adjusted rates as high as 25.8/100,000 women and mortality being 12.7/100,000 women.[1] According to a survey conducted by Indian Council of Medical Research in the metropolitan cities during 1982–2005, the incidence of breast cancer has almost doubled.[2] Studies have reported that in every 4- min one woman is estimated to be diagnosed with breast cancer and in every 8- min one causality due to breast cancer is observed in India. In 2012, approximately 70,218 fatalities were recorded due to breast cancer in India, which was the highest in the world for that year.[3]
Risk factors for developing breast cancer are age, diet, waist-to-hip ratio, body mass index (BMI), highdensity lipoproteins, cholesterol, triglyceride level, more than three pregnancies, years of menstruation, atypical hyperplasia in the previous biopsy, and a history of carcinoma in relatives.[4] Several studies have reported that the early detection of breast cancer by screening is effective in the prevention of disease progression. Clinical breast examinations (CBE) like mammography are not feasible for developing countries due to economic constraints. Hence, advocating breast self-examination (BSE) and promoting awareness are recommended. BSE familiarizes women with both the appearance and the feel of their breasts and helps in detection of any abnormal changes in breasts as early as possible and raises the awareness about early detection of breast cancer, particularly among the rural areas.[5]
Around 20–30% of women wait for about 12 weeks or more after self-discovery of a breast symptom to meet a health-care provider for help, and such delays could lead to poor survival. Comprehension of the factors that influence patient delay is quintessential for the development of an effective and targeted health intervention program. These interventions could also plummet the incidence rates.[6]
This study proposed to evaluate the knowledge, attitude, and practices (KAP) of the participants. The knowledge possessed by a community refers to their understanding of any given topic. Attitude refers to their feelings towards this subject, as well as any preconceived ideas that they may have towards it. Practice refers to the ways in which they demonstrate their knowledge and attitude through actions. Understanding the levels of KAP is crucial to create awareness and customize the interventional programs for each community.[7] BSE is a simple, quick, safe, and non-invasive process.[8] CBE contributes to the early detection of breast cancer, identifies previously undetected masses, more so in women below 40 years in whom mammography is not recommended. It not only promotes the practice of BSE but also encourages subjects to evaluate their assessment of BSE.[9]
This pilot study was undertaken to assess knowledge, attitude, and practices of breast cancer among women of Urban and Rural regions of Belagavi.
A cross-sectional pilot study was taken up by regional Cell for Women, Belagavi District (Southern India).
According to census data 2011, total female population above 7 years was 20,54,090.[10] From Belagavi (rural and urban), 10 towns and 20 villages were randomly selected and from their 4000 samples were randomly selected using probability proportional to size sampling. Sample size for this pilot study was taken as 5% of the total sample size. Hence, 207 female staff from various educational institutions and a teaching hospital was enrolled for the study. The study was conducted from February 2019 to December 2019.
Females in the age group of 20–70 years were included and known cases of breast cancer were excluded from the study. Informed consent was taken in their local language from the subjects. Ethical clearance was obtained from the Institutional Ethical Committee (Ref. MDC/DOME/155 dated 05-11-2019).
A pre-tested, semi-structured questionnaire, and with 40 pertinent questions were structured with four sub-sections (Parts A to D). Part A included the baseline data (age, nativity, religion, diet- vegetarian/ non-vegetarian, parity, assessment of risk factors such as history of breast cancer in family, reproductive history, lactation history, history of contraceptive methods used, history of hormonal therapy, age of menarche, age of menopause, and alcohol and tobacco usage) was collected. Height was measured using the commercial Stadiometer to the nearest 0.5 cm. National Council of Health Center/World Health Organization reference data based on height for age was used for the present study to define stunting. Weight was recorded with digital scale with an accuracy of +100 g. BMI was calculated by Quetelet’s equation.[11,12] Health status of subjects was assessed taking a detailed history and by performing thorough clinical examination by principal investigator.
Part B scrutinized the knowledge of the participants with 15 relevant questions. Part C was assigned to document the clinical findings and Fine-Needle Aspiration Cytology (FNAC), reports if any. Part D was allotted to record notes and remarks (Annexure 1).
The questionnaire was taken from previous studies and modified as per the requirement and validated by this pilot study. The survey was carried out by a core team comprising two doctors and six nurses from the obstetrics/gynecology department. The questionnaire was duly filled by the core team using the interview method before clinical examination. The CBE was performed by the core team, which was trained and monitored by the subject experts. In the event of a clinical suspicious or ambiguity, the subjects were sent for FNAC investigation to the department of pathology.
Only the subjects who were aware regarding the selfexamination were included in this sub-section of the study. In the pro forma section II (Annexure II) question numbers 3, 4, 5, 6, 9, 10, and 11 were included to calculate the total score. For questions 4 and 5 option 2 were correct and for question 6 option one was correct, while for questions 9, 10, and 11 options 3, 3, and 1 were considered as correct answer, respectively.
Similarly, subjects who were aware about clinical examination were included in this sub-section of the study. In the pro forma’s section II (Annexure 1) question numbers 13 to 16 were included to calculate the total score. For question 13 option 2 was correct and for question 14 option 2 or 3 were correct, while for questions 15 and 16 option 1 were considered as the correct answer.
The scoring system implemented was as follows: When the answer was correct it was scored “2.” In the case of multiple choice questions, when multiple options were answered along with the correct answer, it was considered as partial knowledge and it was scored as “1.” To calculate the total score, the overall percentage was considered. Socio-economic status (SES) was classified based on modified Kuppuswamy socioeconomic scale.[13]
Descriptive analysis of the data was done using SPSS Statistics 23.0 and Excel. Continuous variables were presented in mean ± standard deviation form. Categorical variables were presented as frequency tables. Odds ratio has been used for the assessment of effect size of the test. Categorical variables were calculated using Chi-square test. P < 0.05 was considered as significant.
The study included 207 subjects in the age range of 20–70 years. The baseline characteristics of the cohort were documented. Subjects were grouped into four categories from 18 to 45 years based on age. A majority of the subjects (n = 74) were in the age of 36–45 years. The mean height was 5.12 ± 0.44 (in ft) and weight was 59.03 ± 10.29 (in kgs). As per the educational profile, 155 (74.88%) of the subjects in the study were well educated whereas 7 (3.38%) were illiterates and 99.03% were working women. As per SES, 16 (47.06%) were from middle class family in rural areas and 70 (40.46%) were from urban areas, followed by 15 (44.12%) from the lower middle class in rural area and 44 (25.43%) from the upper middle class in urban area. Least population was from the upper middle Class 1 (2.94%) from rural area and 28 (16.18%) were from upper class in urban area. A majority of the subjects in the sample were married, whereas 18.36% were single and the other 5.31% were divorced/widowed.
The risk factors for breast cancer were assessed. Among the total subjects screened, 13 (6.28%) had a family history of breast cancer. History of other cancers was reported in 18 (8.7%) women. History of fibrocystic and endometriosis diseases was reported in 9 (4.35%) and 4 women (1.93%), respectively. Thyroid hormone imbalance was noted in 23 (11.11%). About 3(1.73%) from urban area had previously noticed lumps in their breast while none of the subjects from rural place had noticed lumps in their breast. A majority of the subjects were not on any medication, whereas as 9 (4.35%) and 11 (5.31%) had taken drugs to prevent abortion and for regulating menstrual cycle, respectively.
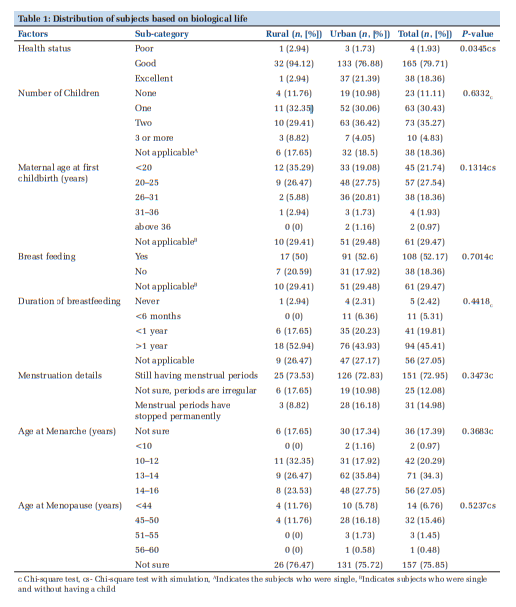
Using Chi-square test with simulation, health status of subjects was observed to be significantly associated with the geographic area (P = 0.0345) (Table 1).
Majority of the subjects in both rural and urban areas had good health. Using Chi-square test, distribution of women having children is approximately equal in rural and urban areas (P = 0.6332). In urban places, majority of subjects had their first child in the age group of 20–25 years followed by 26–31 age groups. Only two subjects in the urban area had their first child in the age of above 36 years whereas in rural areas, majority of the subjects had their first child at the age of “<20 years,” followed by “20–25” whereas none of the subjects in rural area had their child after 36 years.
Majority of the subjects (72.95%) were still menstruating normally whereas for 31 (14.98%) subject’s had attained menopause. For majority of the subjects, age of menarche was “13–14” years, followed by “14-16,” “10-12” and 36 (17.39%) of total subjects were not sure about their age of menarche. Majority of the subjects in the sample were not sure about their age of menopause (Table 1).
The participants from the urban area were well aware about self-examination (P<0.001) as well as about clinical examination (P=0.0039) (Table 1).
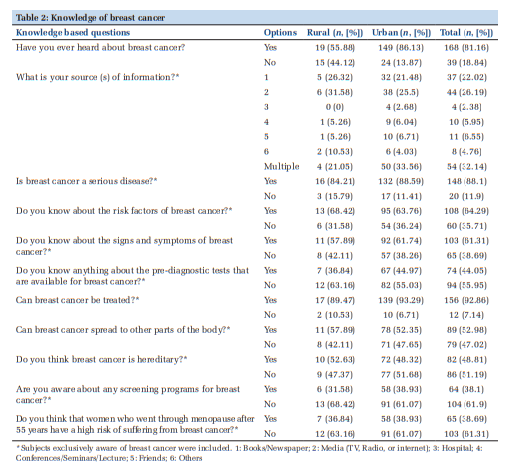
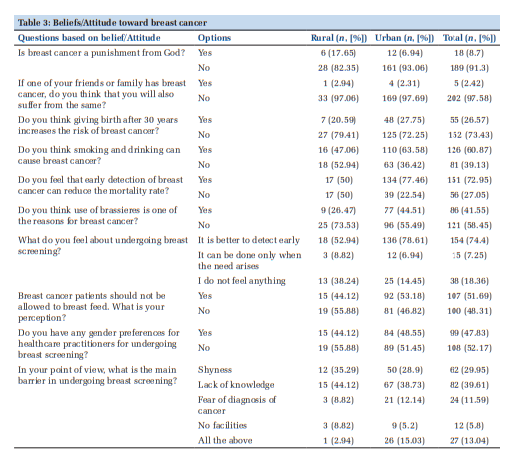
Majority of subjects had heard about breast cancer through media. Many subjects considered breast cancer as a serious disease (88.1%) while 64.29% subjects were aware about the risk factors. Around 61.31% population were aware regarding the symptoms of breast cancer. More than half of the population knew that breast cancer would spread to other parts of the body, and about the screening programs for breast cancer.
Using odds ratio, odds of perception about breast cancer was 4.90 [Confidence Interval (CI) 2.2, 10.94] times higher in the urban than in the rural area (Table 2).
Odds of believing “early detection of breast cancer can reduce mortality rate?” was 3.44 (CI: 1.61, 7.35) times higher in women living in the urban areas than rural areas. Using Chi-square test with simulation, the attitude about undergoing breast screening was significantly associated with the place of residence (P=0.005) (Table 3).
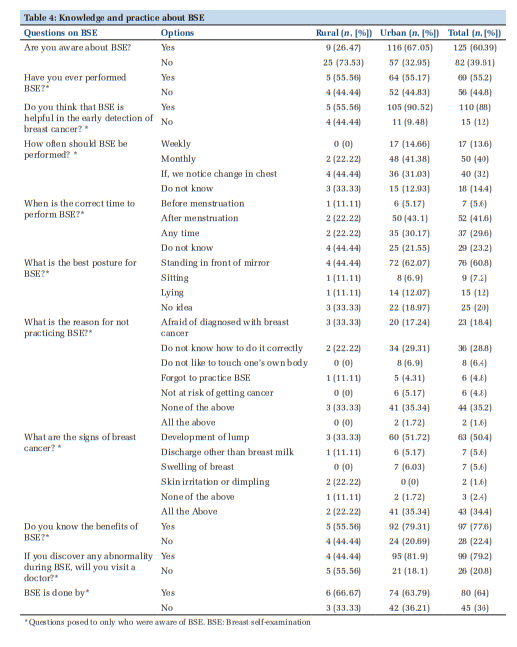
Among the study subjects, 125 (60.39%) were aware regarding BSE of which 69 (55.2%) had performed BSE at least once in their life. Percentage of subjects who performed BSE was approximately equal in rural and urban places of Belgaum. Among the subjects aware of BSE, 110 (88%) thought that it aided in the early detection of breast cancer. Among the study subjects, 50 (40%) recommended a monthly evaluation of BSE and 40 (32%) believed that self-examination is to be performed whenever one noticed any changes in the breast. Among the subjects who were aware of BSE, 97 (77.6%) were aware of the benefits about the BSE (Early detection of breast cancer). Furthermore, 99 (79%) agreed to consult a doctor if they found any abnormalities during the self-examination. About 80 (64%) among the total subjects, conducted the assessment themselves (Table 4).
Odds of women aware of about self-examination was 6.65 (CI: 2.48, 12.90) times higher in the urban area than in the rural area. Among the subjects who were aware about self-examination, odds of considering that BSE was helpful in the early detection of breast cancer was 7.64 (CI: 1.78, 32.69) times higher in urban area than rural area. Among the subjects aware of self-examination, odds of consulting a doctor in the case of discovering an abnormality during selfexamination, was 5.65 (CI: 1.40, 22.87) times higher in urban women when compared to rural women (Table 4).
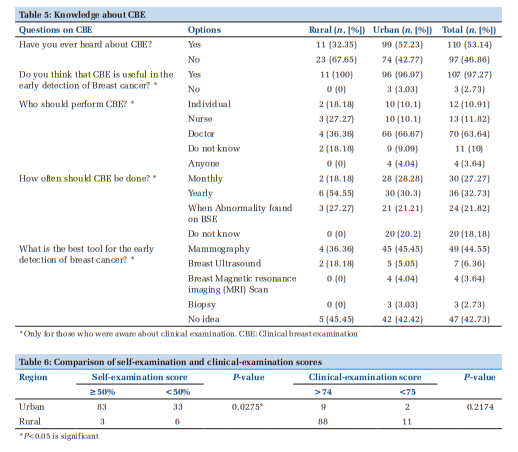
We observed that among a total of 207 subjects, 110 (53.14%) had heard about CBEs. Out of 34 subjects from the rural area, 11 (32.35%) were aware of CBE, whereas among 173 subjects from the urban area of Belgaum, 99 (57.23%) were aware about CBE. Almost all the subjects who had heard about CBE believed it to be a tool in the early detection of breast cancer. 70 (63%) of the subjects who were aware about CBE considered that a doctor should perform the clinical examination (Table 5).
Using Chi-square test with simulation, selfexamination score category was significantly associated with place of residence. Using odds ratio, the odds of having good scores of self-examinations was 5.03 (CI: 1.18, 21.30) times higher in urban area than in rural area. Using Chi-square test with simulation, clinical examination score was independent of place of residence (Table 6).
Breast cancer is the most common type of cancer in Indian women with a considerable mortality rate. It can be associated with the lack of awareness, knowledge, and practice about breast cancer. This study focused on the screening women from both urban and rural areas to assess the knowledge, awareness, and beliefs regarding breast cancer. Subject’s knowledge regarding BSE and CBE was also assessed in the study.
In the current study, 36–45 years were the most common age group whereas in a study conducted by Grunfeld et al. (2002), 25–34 years were found to be the most common age group.[6] This may be due to the variations from one region to another.
Most of the subjects from the current study were from the middle class (47.06%), while in a study conducted by Sehrawat et al. (2016), more subjects were found to be from the upper middle class (55.3%).[14]
The results of the Birhane et al. (2017) showed that knowledge and practices of BSE among female students were 64%, 30.25% had a good knowledge and 28.3% had performed BSE.[15] The varying results between the two studies may be due to the difference in the study population considered for the study. Respondents in some studies[16-18] had a good perception toward breast cancer while in the present study, a moderate knowledge about breast cancer was observed.
A study conducted by Kumarasamy et al. (2017), in rural area of India demonstrated that only 26% of the women were aware of BSE, of which 18% had examined their breasts, and 5% practiced it regularly.[19]
In the present study, a total of 53.14% were aware of CBE among which a majority (63.64%) of population believed that it should be performed by doctors. A study by Siddharth et al. (2016) found that all study participants are aware of CBE and all of them thought that CBE can be done by doctors only (100%) while none of them were aware of BSE.[20]
In the current study, most of the women from urban area were aware of CBE and had a positive approach toward it, while in a study by Sehrawat et al. (2016), in urban and rural areas of district Gurdaspur (Punjab) found that 46%% women were aware about CBE.[14]
The study assessed the basic knowledge of breast cancer among women and the extent of their beliefs regarding breast cancer, along with the knowledge and practice regarding SBE and CBE. It has, thus, served as an educational diagnosis of the community.
The study has its share of limitations. There was unequal distribution of subjects between the groups as more subjects belonged to the urban area. Future studies could recruit an equal number of participants from both urban and rural regions to obtain an accurate estimate.
Breast cancer is the most common cancer affecting women worldwide. There are many risk factors such as age, breast pathology (proliferative breast disease), family history, and genetic predisposition for the development of breast cancer. Mammography is the mainstay for the diagnosis of breast cancer; magnetic resonance imaging and ultrasound have emerged as useful diagnostic tools for breast cancer. Breast cancer can be treated and managed by a prudent multidisciplinary collaboration of surgeons, oncologists, radiation oncologists, nurses, geneticist, reconstructive surgeons, and patients.[21]
This study provides a hereto unexplored insight into the KAP regarding breast cancer among the women of urban and rural areas of a tier II city. It was observed that majority of the women in the urban area had more than a fair idea about breast cancer; its early evaluation methods, namely, BSE and CBE.
Subscribe now for latest articles and news.