Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.v8i1.21.107
Year: 2022, Volume: 8, Issue: 1, Pages: 73-77
Review Article
R S Jyothi1 , B Manjula2 , K Gurupadappa3
1Assistant Professor, Department of Biochemistry, Shimoga Institute of Medical Sciences, Shimoga, Karnataka, India, 2Research Scientist I, Multidisciplinary Research Unit, Shimoga Institute of Medical Sciences, Shimoga, Karnataka, India, 3HOD, Department of Biochemistry, Shimoga Institute of Medical Sciences, Shimoga, Karnataka, India
Address for correspondence: R S Jyothi, Assistant Professor, Department of Biochemistry, Shimoga Institute of Medical Sciences, Shimoga, Karnataka, India. E-mail: [email protected]
Background: Several studies have suggested that hepatic and renal abnormalities are seen in COVID-19 patients. So in this study; we are evaluating the hepatic, renal and inflammatory bio-makers in mild and severe group of COVID-19 patients. Objective: To evaluate and compare the hepatic, renal and some inflammatory biomarkers in mild and severe group of COVID-19 patients. Methods: It was a single-centric retrospective study. This study included a total number of 199 RT-PCR confirmedCOVID-19 patients. These patients were divided into the mild group (n=96) and severe group (n=103) depending on the requirement of intensive care unit. We evaluated and compared the hepatic, renal and some inflammatory biomarkers between the mild and severe groups. Statistical analysis was done using a statistical package for the social sciences (SPSS). Results: Out of 199 cases, 68.3% were male and 31.7% were female. The mean age of the study population was found to be 52.4±14.6 years. Statistically, a significant difference at 5%(p=0.001) was observed for creatinine, urea, direct bilirubin, ferritin, aspartate amino-transferase, total protein, and albumin levels between the mild and severe group except for uric acid, total bilirubin, alanine-transaminase, alkaline phosphatase and lactate dehydrogenase. Conclusion: Our study shows hepatic and renal abnormalities are observed in COVID-19 infection. However, the percentage of hepatic and renal abnormalities was more in the severe group compared to the mild group. Further extensive studies should be carried out with a larger population with multi-centric studies in Karnataka.
Keywords: COVID-19, Hepatic, Renal
Coronavirus disease 2019 (COVID-19) caused by severe acute respiratory syndrome-corona virus 2 (SARS-CoV-2) was first identified in Wuhan, China. It has rapidly developed into a global outbreak characterized by human-to-human transmission. [1] Globally it has caused a total of 418,650,474 confirmed cases, including 5,856,224 deaths as of February 18, 2022 and in India it has caused a total of 42,780,235 confirmed cases, including 510,905 deaths as of February 18, 2022.[2] In Karnataka, the total confirmed cases were 39,36,586, including 39,795 deaths as February 19, 2022. Whereas in Shivamogga district the total confirmed cases were found to be 83,115 including 1126 death as of February 19, 2022.[3] Currently, the real-time reverse transcriptase-polymerase chain reaction (RT-PCR) from nasopharyngeal swabs and broncho-alveolar lavage fluids is used for diagnosis. However, some hematology and biochemical parameters were elevated in COVID-19 patients. Several studies reported that though COVID-19 infection primarily affects lungs, liver, kidney and even heart are affected in later stages.[4,5] Many studies have observed hepatic and renal abnormality in COVID-19 patients.[6,7] Further, moderate micro-vesicular steatosis, mild lobular and portal activity found in the liver biopsy specimens of dead patients indicated the involvement of SARS-CoV-2 in liver damage.[8,9]
However, studies regarding the hepatic and renal abnormalities in COVID-19 infection are less in the Indian population compared to other developed countries. In this study, we are evaluating and comparing hepatic, renal and inflammatory biomarkers in mild and severe COVID-19 patients of the Shivamogga region.
It was a single-centric retrospective study design carried out in tertiary 950 bedded district teaching hospital. The duration of the study was6 months (December 2019 to May 2020). The study participants were COVID-19 patients admitted and treated in this time period. Inclusion criteria was RT-PCR confirmed COVID-19 patient’s between25 - 75 years. Exclusion criteria: 1) Patients with a previous history of diabetes mellitus, liver and kidney disease. 2) Patients with history of coronary artery disease. 3) The patients with incomplete medical records. 4) Patient with less than 25 years. A total number of 199 cases were included in this study. Out of these 199 cases, 136 were male and 63 were female. The cases were recruited into 3 age groups (≥40, 40-60 and ≥60 years). We then classified these cases into mild and severe group depending on the requirement of intensive care unit (ICU) treatment. Patients who required ICU care were in the severe group and who did not require ICU care during hospitalization were in the mild group. For this study ethical clearance was obtained from the Institutional Ethics Committee of ShivamoggaInstitute of Medical Sciences, Shivamogga.
Data of age, gender and laboratory findings such as urea, creatinine, uric acid, total and direct bilirubin, total protein, serum albumin, aspartate aminotransferase (AST), alanine transaminase (ALT), alkaline phosphatase (ALP), lactate dehydrogenase (LDH) and ferritin was collected.5 ml of venous blood collected under all aseptic precautions was used for analysis. All laboratory parameters were analyzed by most recommended and standard methods using system pack by Erba Biochemical auto-analyzer XL640. Urea, creatinine and uric acid were analyzed by Urease- L-glutamate dehydrogenase (GLDH) method, Jaffe’s method and Uricase method respectively.
Bilirubin was estimated by Diazo method, AST and ALT by modified International Federation of Clinical Chemistry (IFCC) method. Total protein and albumin were estimated by Biuret and bromocresol green (BCG) dye method respectively. LDH was estimated by UV kinetic-Deutsche Gessel schaftfür Klinische Chemie (DGKC) method and Ferritin by turbidimetric method. The data obtained was entered into Microsoft Excel and analyzed using SPSS software version 22. Descriptive statistics such as frequencies and percentages; mean and standard deviation were calculated. Inferential statistics like the chi-square test were applied. The statistical significance at 5% level was calculated.
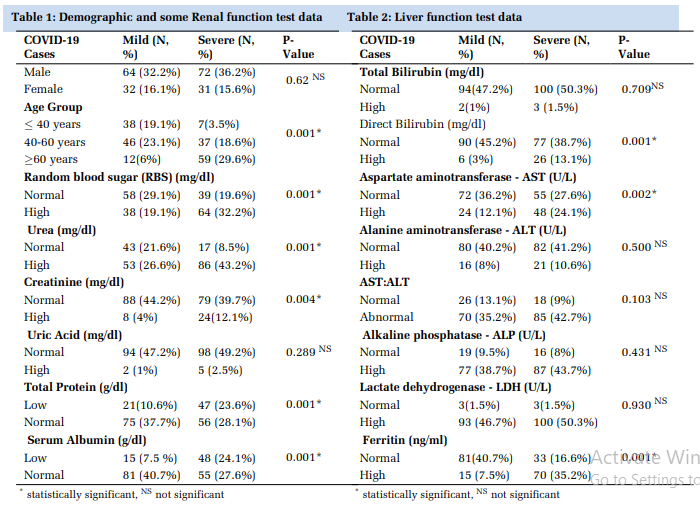
In this study, we classified the cases into two groups as mild and severe depending on the requirement of ICU care during their hospitalization. Out of 199 patients, 48.2% were under the mild and 51.8% were under the severe group. In mild group 32.3% were males and 16.1% were females. In severe group, 36.2% were males and 15.6% were females. The p value at 5% significance for comparison of male and female between mild and severe group was 0.62 which was not significant.We had recruited the cases into 3 age groups (≤40, 40-60, and ≥60 years). The mean age of the study population was found to be 52.4 ± 14.6 years. The percentage of COVID19 patients was more in the 40-60year age group compared to other age groups. However, in severe group, the percentage of cases was more in ≥60 years age group (Table 1).
The percentage of high level of serum creatinine, urea, and uric acid was observed in 4%, 26.6%, and 1% of cases in mild group, whereas in severe group the percentage of high levels of serum creatinine, urea, and uric acid was observed in 12.1%, 43.2%, and 2.5% of cases. Statistically, a significant difference was observed for creatinine (p=0.004) and urea (p=0.001) levels between the mild and severe group except for uric acid (p=0.289) (Table 1).
The percentage of high levels of total bilirubin, direct bilirubin, ferritin, AST, ALT, ALP and LDH was observed in 1%, 3%, 7.5%, 12.1%, 8%, 38.7% and 46.7% of cases in mild group, whereas in severe group the percentage of high levels of total bilirubin, direct bilirubin, ferritin, AST, ALT, ALP and LDH was observed in 1.5%, 13.1%, 35.2%, 24.1%, 10.6%, 43.7% and 50.3% of cases(Table 1 and Table 2). Statistically significant difference was observed for levels of direct bilirubin (p=0.001), ferritin (p=0.001) and AST (p=0.002) between the mild and severe group except for total bilirubin (p=0.70), ALT (p=0.50), ALP (p=0.43) and LDH (p=0.93) (Table 1 and Table 2). The percentage of low levels of total protein and albumin was observed in 10.6% and 7.5% of cases in mild group, whereas in the severe group the percentage of low levels of total protein and albumin observed in 23.6% and 24.1%of cases. Statistically, a significant difference at 5% was observed for levels of total protein (p=0.001) and albumin (p=0.001) between the mild and severe group (Table 1).
In this study, we classified the patients into two groups as mild and severe depending on the requirement of ICU care. Out of 199 patients, 48.3% were under the mild and 51.8% were under the severe group. Previous studies stated that people more than 40 years of age have a higher risk of COVID19 infection.[10,11] . In our study, the percentage of COVID-19 infection was more in 40-60 years. However, in severe group the cases were more in ≥60 year age group compared to other age groups.
This might be due to compromised nutrition, life style, psychological conditions and decline of natural immunity in older age group.
Renal abnormalities: Several studies reported that people with COVID-19 were at a significant risk of acute kidney injury. The incidence of renal abnormalities ranges from 0.5-36.6%.[12] Some studies reported that in severe acute respiratory syndrome (SARS) patients impaired glomerular filtration occurs, manifested by elevated blood creatinine and urea nitrogen levels.[13]
In our study, elevated levels of urea and creatinine were noted in COVID19 individuals except for uric acid. The elevated levels of urea and creatinine show a statistically significant at 5% between mild and severe COVID-19 infection except for uric acid. These findings support that during infection, the virus damages the renal cells resulting in abnormalities in renal biochemical markers.
Hepatic abnormalities: Some studies reported that people with COVID-19 were at a significant risk of the development of hepatic disorders. The incidence of hepatic disorders/abnormalities ranges from 15- 65%.[14] This wide range could be due to varying laboratory reports, regional variations, etc. The liver function enzymes (AST, ALT, and ALP) levels were elevated due to hepatic injury in these patients. Studies reported that elevation of liver enzymes occur in a median of 15% to 58% in COVID-19 patients.[15]
In our study, the elevated AST, ALT and ALP levels were observed but a statistically significant at 5% between mild and severe COVID-19 infection was obtained for only AST. These findings support that during infection, there is hepatic injury resulting in abnormalities in liver enzymes.
Total bilirubin: Total bilirubin is a component of the liver function test. The bilirubin levels were elevated or altered in patients with COVID-19 infection. Studies reported that the elevated levels of total bilirubin ranged from 2.2-37.5% in COVID19 patients.[16,17] In our study also, we observed the elevated levels of total bilirubin, but statistical significance at 5% was not obtained between mild and severe COVID-19 infection.
Serum Total protein and albumin: Albumin is synthesized from hepatic cells and it will play an important role in maintaining body nutrition and osmotic pressure.[18] According to some studies there is significant decrease in albumin levels of COVID19 patients. It could be due to systemic inflammation and hepato-cellular injuries.[19]
In our study also the total protein and albumin levels were decreased and showed the statistical significance at 5% (p value 0.001) between mild and severe group.
LDH Levels: Lactate dehydrogenase (LDH) is one of the inflammatory biomarkers. Numerous studies reported the elevated levels of LDH in COVID19 patients. It ranged from 29.5-100% in their study[19]
In our study, the LDH level was elevated in 97% of cases. In the mild group the elevation of LDH was in 46.7% of cases whereas 50.3% of cases in severe group. This result implies that during viral infection, the inflammation process is triggered with the release of pro-inflammatory molecules.
Ferritin levels: Ferritin is an iron-containing blood protein. In iron deficiency, the levels of ferritin decrease whereas in liver disease, rheumatoid arthritis and other inflammatory conditions the ferritin levels were elevated[20] Previous studies and meta-analyses reported that, thee levated levels of ferritin in COVID-19 patients[21,22] Even in our study, the ferritin level was elevated in 42.7% of patients. In the mild group the elevation of ferritin was seen in 7.5%of cases and in the severe group it was elevated in 35.2% of cases. Elevated levels of ferritin show statistical significance at 5% between mild and severe COVID-19 infection. These findings suggest the importance of ferritin levels in assessing the severity of the disease.
It is a retrospective analysis of the data collected from a single center. All inflammatory biomarkers were not investigated.
Our study suggests that the hepatic, renal and inflammatory biomarkers are elevated in COVID19 patients. The percentages of hepatic and renal abnormalities were more in the severe group compared to the mild group. So evaluations of these laboratories biochemical parameters are more significant in assessing the severity of infection in COVID-19 patients.
Acknowledgment: Authors acknowledge the warriors, lab technicians and multidisciplinary research unit of ShivamoggaInstitute of Medical Sciences, Shivamogga.
Subscribe now for latest articles and news.