Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.v10.i1.23.394
Year: 2024, Volume: 10, Issue: 1, Pages: 118-120
Case Report
Saswati Sen1 , Snehalata Dash1 , Akash Sidana1 , Anjali Goel1
1Department of Ophthalmology, KIMS Bhubaneswar, Patia, Bhubaneswar, Odisha, India
Address for correspondence:
Saswati Sen, Department of Ophthalmology, KIMS Bhubaneswar, Patia, Bhubaneswar, Odisha, India.
E-mail: [email protected]
Received Date:24 November 2023, Accepted Date:26 February 2023, Published Date:29 April 2024
Congenital anomalies in individuals, more often than not involve multiple organs. We present the case of a 26-year-old female who presented with headache and sleep disturbances as primary complaints. She was found to have a partially empty sella in association with iris and optic disc coloboma. Septo-optic dysplasia is commonly seen in patients with complete or partially empty sella where hypoplasia of optic nerve is seen. Association of iris coloboma and optic disc coloboma with partially empty sella has been reported rarely and was discovered in this patient.
Keywords: Insomnia, Coloboma, Congenital Anomalies, Optic Nerve Head, Empty Sella
Ocular manifestations in many instances can act as a window to diagnose several inborn and acquired systemic conditions 1, 2. Likewise many systemic disorders have several ophthalmic manifestations as well. Developmental anomalies when present usually involve one or more organs. Kallmann's syndrome, Septo-optic dysplasia, and Empty sella syndrome are disorders that affect the optic nerve significantly 1. But some chance findings may be seen associated with the common findings too. Once discovered, it should be kept in mind to look for all these features when we come across such cases. This may help diagnose, treat or explain the prognosis better to the patients.
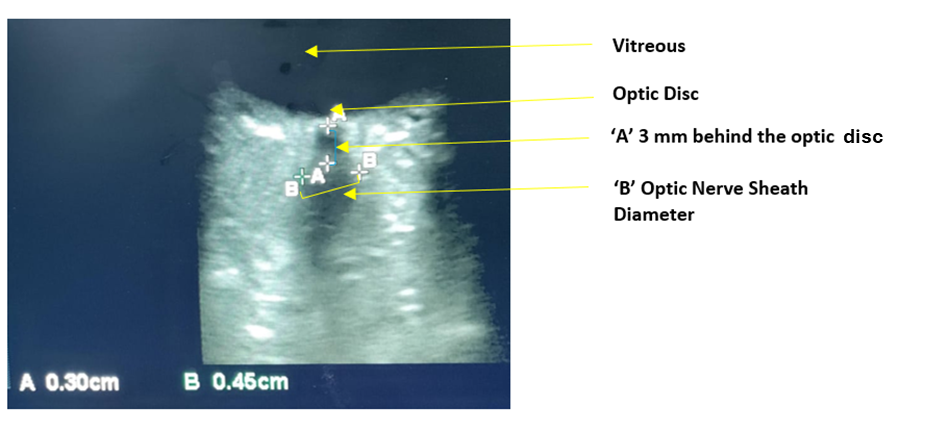
A 26-year-old female presented to the outpatient department of Ophthalmology with complaints of defective vision and headache. The headache was not associated with vomiting or any other aggravating or relieving factor. She gave a history of sleep disturbances for which she had consulted the physician. There was no history of any trauma, surgery or any treatment or hospitalization history before the presentation. She was asked to undergo an ophthalmology evaluation and advised blood investigations and imaging. On ocular examination, her anterior segment examination showed an iris coloboma in both eyes [Figure 1 A]. On fundus examination, there was coloboma of fundus involving the optic disc in both eyes [Figure 1 B]. Her best-corrected visual acuity was 6/36 in the right eye and 6/60 in the left eye. Intraocular pressures were 16 mm hg in both eyes. Blood investigations revealed prolactin levels of 68ng/ml and T3 level 0.96 ng /ml, T4 level 9.12 µg/ml, TSH level of 2,37µIU/ml. Liver function and renal function tests along with blood sugar levels were normal. Humphery visual field analysis showed superior arcuate defects with few inferior field loss in the right eye and severely depressed fields in the left eye. Magnetic resonance imaging showed a partially empty sella with indentation of the pituitary with cerebrospinal fluid (CSF) and excavation near the optic nerve head [Figure 2, Figure 3] . Ultrasound of the abdomen and pelvis showed no other abnormality. The patient was prescribed glasses, explained the visual prognosis and referred to a physician for treatment of abnormal hormone levels and sleep disturbances.


The cause-effect relationship between empty sella and visual deficiencies has been a topic of discussion amongst ophthalmologists. A partial empty sella may be seen in neuroimaging due to the partial absence of pituitary tissue or enlargement of sella turcica. The prevalence of partially empty sella has been found to be as high as 35%. This increases with age and is more common in women3 .Optic disc coloboma, on the other hand, is an excavation of the optic nerve head which occurs due to incomplete fusion of the proximal ends of the optic cup or due to incomplete migration of the neural crest cells. PAX 2 mutation causing abnormal astrocytic differentiation is said to play a role 4. Visual disturbances attributed to empty sella syndrome are primarily due to the compression of the optic nerves and the chiasma due to increased intracranial pressure of the CSF in the space which was supposed to be filled by the pituitary gland 5. These patients have pituitary hormone abnormalities as well. Optic nerve hypoplasia, papilloedema, glaucomatous optic atrophy are some of the findings associated with empty sella syndrome 1, 6. Optic disc coloboma may be associated with rhegmatogenous retinal detachment or congenital cysts of optic nerve locally or with systemic syndromes like CHARGE, Dandy-Walker, Goldenhar syndromes 7. The coloboma of the iris that is present in our case is usually seen in the inferonasal quadrant and is due to the failure of the embryogenic optic fissure to close during the fifth week of gestational life. Occasionally small iris tissue may be present as a bridge, which is known as 'bridge coloboma' as seen in our case. Since the optic fissure closes ventrally last, the colobomas are usually ventral. The association between iris and optic nerve coloboma can be thus correlated. The prevalence of optic disc anomalies is about 1.1% in the general population in south India as per a study by Bassi et al out of which coloboma constitutes around 0.08% 8. The association of empty sella with optic disc coloboma and iris coloboma could be a chance finding and points more towards congenital or developmental pathogenesis. The association with systemic abnormalities points towards genetic abnormality too. But in our case, no gross systemic abnormality was noted clinically and also as evidenced by the imaging reports. Normally due to the compression of pituitary stalk in these cases, dopamine does not reach the pituitary gland which may explain the hyperprolactinemia. In addition as per some studies, prolactin levels are found to be abnormal during the REM (Random eye movements) phase of sleep 9. The partial empty sella could cause pituitary and optic chiasma compression which in turn can cause compromise of the retinohypothalamic tract function. This tract helps the eyes convey information regarding day and night cycle to the hypothalamic nuclei 10. This could explain the complaints of sleep disturbances that the patient presented with. As per our knowledge, this coincidental association has not been reported in the literature and the symptoms of insomnia, headache, and visual disturbance have been well accounted for by the clinical and radiological findings.

When a number of conditions of various organs appear together, it may be called a syndrome. Some of these conditions appear frequently and some are rare. Though the cause-effect relationship between the two findings in our case is hard to establish, the developmental and congenital association between the two cannot be overlooked. A detailed evaluation of such cases helps in a better understanding of the disease process. When an iris coloboma is seen all other ocular structures need to be thoroughly examined for developmental anomalies and systemic examination should be meticulously done to exclude any syndrome or genetic abnormality. This by far is a unique association that has not been reported. Though it may be co-incidental it cannot be ignored. It will help in keeping our minds open for diagnostic surprises as well as in planning the counseling, management, and rehabilitation in cases of unexplained visual loss.
Subscribe now for latest articles and news.