Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.2021.v07i03.012
Year: 2021, Volume: 7, Issue: 3, Pages: 59-66
Original Article
Alok Kumar1 , Prerna Singh1 , Richa Sharma1
1The Faculty of Medical Sciences, We Care Medical Centre, The University of the West Indies (Cave Hill), Barbados, Barbados
Address for correspondence:
Alok Kumar, The Faculty of Medical Sciences, We Care Medical Centre, The University of the West Indies (Cave Hill), Barbados, Barbados. E-mail: [email protected]
Objectives: The main objective was to describe the enrollment dynamics, children demography and service uptake by children at a private pediatric primary health care center in the pluralistic health care settings of Barbados. Methods: This is a prospective clinical audit of children attending the We Care Medical Center, one of the private pediatric primary health care facilities in Barbados. The audit period dates from January 2006 through December 2018 and included children from birth to sixteen years who attend this center for their Well care and for a full range of Problem-focused care. Results: There were 16, 650 visits from 2818 children enrolled during 2006 through 2018. Overall, 11452 (68.8%) and 5198 (31.2%) visits were from children < 5 years and 5 to 15 years age groups respectively. Over the study period, 2770 (98.3%) children had 5 or more visits and 241 (8.5%) children had multiple (>16) repeat visits. Overall, 9993 (60%) of all visits were from children without any health insurance and 5599 (33.6%) of the visits were from children with health insurance. The three most common reasons for visits were Allergic Rhino-Conjunctivitis, Upper Respiratory tract infection and Asthma phenotypes in 25.7%, 19.1% and 19.0% respectively. Conclusions : A significant proportion of the children in this country received their primary care from a pediatrician and nearly two-thirds of these visits are paid for by the parents. Most visits were problem-focused. Allergic rhino conjunctivitis and Asthma phenotypes were among the most common reasons for the visits.
Keywords: Primary health care, Children, Private pediatric practice
Primary care is the foundation of pediatric care and the American Academy of Pediatrics advocates for the primary care practice to be the center of health supervision, screening, management of acute and chronic conditions, and care coordination for children.[1] Pediatricians deliver excellent healthcare to children and their role in reducing childhood mortality and morbidity is well-established.[2] Data on the pediatrician directed primary care for children including patient demography and health service utilization is lacking.[3] Studies based on US physician visit data from the 1970s indicate that a small proportion of children visited pediatricians for primary care and this proportion further decreases as they grew older; adolescents account for a relatively small proportion of pediatric patients.[4] However, the steady increase in the US pediatrician-child population ratio (PCPR) occurring since that time could have resulted in an increased number of visits to pediatricians by older children and adolescents.[5]
Barbados, an English-speaking Caribbean country, has a pluralistic health care system whereby people have a choice to utilize the health services in the public sector free of charge at the point of delivery, the private sector at a fee that is out-ofpocket, or through a number of the health insurance schemes available.[6,7] In this study — the first of its kind from this region — we describe the demography, visit frequency and reason for visits from children attending a private pediatric primary health care center in the pluralistic health care setting of Barbados
This is a prospective clinical audit of children attending the We Care Medical Center (WCMC), one of the private pediatric primary health care facilities in Barbados. This facility provides continuing primary health care to a cohort of children (< 16 years of age with few exceptions where older children with severe developmental delays are seen beyond 16 years) registered at this center. It is a solo pediatric practice. Registration is on a continuous basis. As new children are enrolled, those attaining the age of 16 years exit this center. The audit period dates from January 2006 through December 2018. All children from birth up to the sixteenth birthday were included for this audit. Children attend this center for their Well (Preventative health) care, which includes growth, development-monitoring and immunization. They also attend for a full range of Problem-focused (Curative) care for any acute illnesses, as well as, for follow up of any chronic medical illnesses. This center operates on two half days, from 8 AM to 12 Noon during the weekdays, and from 8 AM to 12 Noon on Saturdays. This center is operated by a single Pediatrician. Visits to this clinic are charged directly to the parents or guardian of the child, or to their health insurance, if they have one.
Data on the date of enrollment at this center, age of the child at enrollment and child’s gender were collected form the enrollment register maintained at the center. Demographic and health insurance profile for all of the visits at this facility as well as the medical information on diagnosis for all of the visits by the children were collected from their electronic medical records. All medical records of the children who visit this facility are stored in a password protected database, and only the attending physician has access to this electronic database. Patient’s data extracted for analysis were anonymized.
Outcomes measured included the demographic profile, number of visits including frequency of recurrent visits from the same child, payment methods (insurance versus out-of-pocket payment), reason (diagnosis given) for visit and the proportion of children who required referral for in-patient care. Number of children who had multiple repeat visits (16 or more visits) was also an outcome measure. The number ‘16’ was chosen to be the cut-off number as according to the local guideline this would be the minimum number of visits for health maintenance with 3 visits during the first year, two visits in the second year and then a single annual visit thereafter. The reason or reasons (diagnosis) for visit were broadly classified as Well-care/preventative care visits and problem focused/curative care visits. A provisional diagnosis of Asthma phenotypes were assigned to children who presented with wheezing, cough, chest tightness or short of breath on two or more occasions. Categorization into the different phenotypes was not possible in this setting. Diagnosis of Allergic Rhino Conjunctivitis (ARC) was assigned for children presenting with blockage or congestion of nasal passage, watery discharge from nose or eyes, excessive sneezing and/or itching of eyes or nose on two or more occasions.
IBM SPSS 27.0 statistical software package was used for data tabulation, generation of graphs and for statistical analysis. For all proportions, 95% Confidence Interval (CI) with continuity was calculated with continuity correction. Categorical data was compared for significant differences using the Odds Ratio with 95% confidence interval. A P value of <0.05 was considered significant.
This audit of children’s case records was done by the physician directly involved in their care. Ethical approval (IRB approval No. 2020/12/03) was obtained from the Institutional Review Board at We Care Medical Centre of the Medical Teaching Research And Consultation (MTRAC) Services Incorporated.
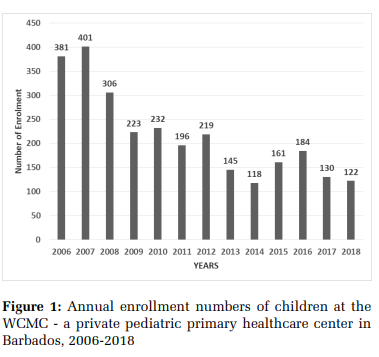
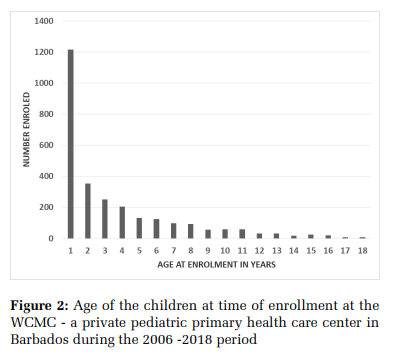
Over the 12-year audit period, a total of 2818 children, 1366 (48.5%; 95% CI = 46.6%, 50.3%) females and 1452 (51.5%; 95% CI = 49.7%, 53.4%) males, were enrolled for health care at the WCMC. The annual enrollment during the 12-year study period is shown in Figure 1. The mean annual enrollment was at 217 (Range 401 – 118). The age at the time of enrollment to this facility is shown in Figure 2. Overall, 1216 (43.1%; 95% CI = 41.3%, 45.0%) were enrolled during the first year of their life and of this 692 (24.6%; 95% CI = 20.2%, 28.5%) children enrolled during the first 3 months of their life. Of all the enrolled children, 804 (23.8%; 95% CI = 22.2%, 25.4%) had commercial health insurance, 2114 (75.0%; 95% CI = 73.4%, 76.6%) had no health insurance and in 34 (1.2%; 95% CI = 0.8%, 1.7%) cases there was no information on health insurance. Among those who had insurance, 691 (24.5%; 95% CI = 22.9%, 26.2%) children had an insurance that required the parents to make an upfront payment and then claim reimbursement and 113 (4.0%; 95% CI = 3.3%, 4.8%) had a health insurance which allowed direct charge to the insurance company and the children did not have to make upfront payment.
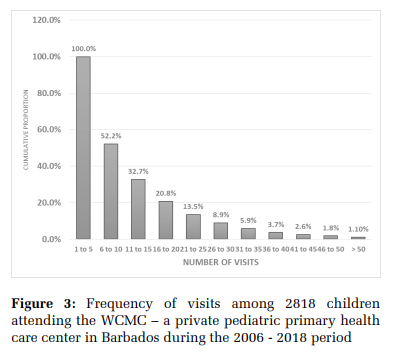
There were a total of 16, 650 visits form the 2818 children during the 12-year period. There were 7447 (44.7%; 95% CI = 44.0%, 45.5%) visits from females and 9203 (55.3%; 95% CI = 54.5%, 55.0%) visits from males. Overall 11452 (68.8%; 95% CI = 68.1%, 69.5%) visits were from children < 5 years and 5198 (31.2%; 95% CI = 30.5%, 31.9%) visits were from children in the age group 5 to 15 years. There were 3613 (21.7%; 95% CI = 21.1%, 22.3%) visits from children in the age group birth to <12 months. Figure 3 shows the frequency of visits from 2818 individual children to the WCMC during the 12 years study period. There were 21 (0.75%) and 37 (1.3%) who had just one and two visits respectively. Rest of the 2770 (98.3%; 95% CI = 97.7%, 98.7%) children had > 5 visits. Overall 241 (8.5%; 95% CI = 7.6%, 9.7%) had multiple (>16) repeat visits.
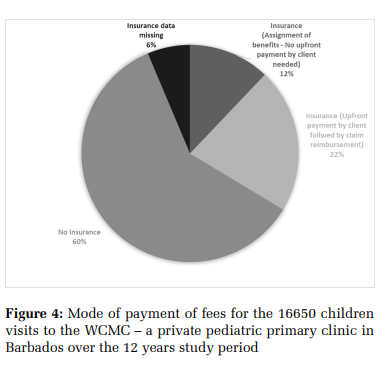
The mode of payment for the consultation fees from the children attending the WCMC over the study period is shown in Figure 4. Overall, 9993 (60%; 96% CI = 59.3%, 60.8%) of all visits during the study period were from children without any health insurance. A comparison of the frequency of visits and the availability of health insurance for the children attending the WCMC is shown in Figure 5. Overall, 13.5% of those without health insurance had multiple repeat visits while 35.2% of those having commercial health insurance had multiple repeat visits. This difference in the proportion of children with multiple repeat visits among those without insurance and those with insurance was statistically significant (OR = 3.1; 95% CI = 2.95, 3.45; P<0.0001).
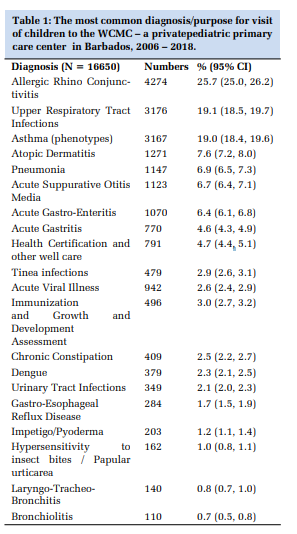
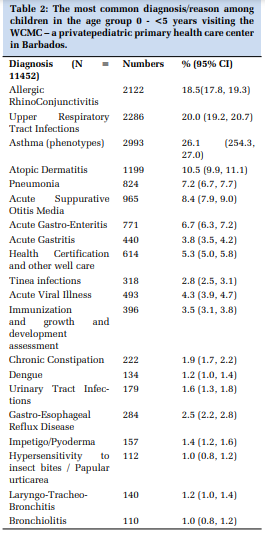
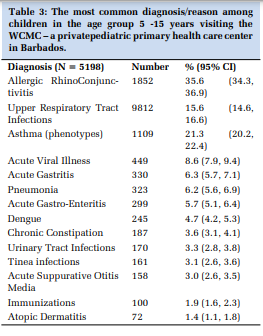
The diagnosis given for the 16,650 visits to this facility over the 12 years study period is shown in Table 1. Overall, the three most common reasons for visits were Allergic Rhino-Conjunctivitis, Upper Respiratory tract infection and Asthma phenotypes in 25.7% (95% CI = 25.0%, 26.2%), 19.1% (95% CI = 18.5%, 19.7%) and 19.0% (95% CI = 18.4%, 19.6%) respectively. Table 2 shows the diagnosis given for the 11,452 visits from children in the age group birth to <5 years. In this age group, the diagnosis of an asthma phenotype was associated with the diagnosis of an upper respiratory tract infection and/or pneumonia in 824 (27.5%; 95% CI = 25.9, 29.2%) visits and with the diagnosis of ARC in 713 (23.8%; 95% CI = 22.3%, 25.4%) of visits. The diagnosis given for 5,198 visits from children in the age group 5 to 15 years is shown in Table 3. In this 5 to 15 years age group, the diagnosis of an asthma phenotype was associated with a diagnosis or upper respiratory tract infection and/or pneumonia in 378 (34.1%; 95% CI = 31.3%, 37.0%) whereas the diagnosis of ARC was associate with the diagnosis of asthma in 829 (74.7%; 95% CI = 72.1%, 77.3%). Overall, during the 12-year study period, there were 15,020 (90.2%; 95% CI = 89.7%, 90.7%) visits for acute problem focused / curative care, 1,287 (7.7%; 95% CI = 7.3%, 8.1%) visits for well care / preventative care (immunization, health certification and well-baby visits for growth and development assessments) and 343 (2.1%; 95% CI = 1.8%, 2.3%) visits for follow up care for chronic diseases (also problem based). Among the 3,613 visits from under-1 year and 11,452 visits from children under-5 years of age, 497 (13.8%; 95% CI = 1.7%, 14.9%) and 1,010 (8.8%; 95% CI = 8.3%, 9.4%) were for well care.
Overall, from the 16,650 visits to this center, there were a total of 378 (2.3%; 95% CI = 2.1%, 2.5%) referrals to the QEH for hospitalization. From 11,452 visits in under 5 years children, 299 (2.6%; 95% CI = 2.3%, 2.9%) were referred for hospitalization whereas from the 5,198 visits in 5 to 15 years children, 79 (1.5%; 95%CI = 1.2%, 1.9%) were referred for hospital care. The Highest rate of hospitalization was seen among the 3,613 infants visits where 167 (4.6%; 95% CI = 4.0%, 5.3%) were referred for hospital care. The odds (Odds Ratio) of being referred for hospitalization in this age group was 3.13 (95% CI = 2.38, 4.11) when compared to visits from children in the age group 5 to 15 years. Of the infants who required referral for hospitalization, suspected sepsis (29.2%), acute gastroenteritis with severe dehydration or inability to tolerate oral fluid (20.6%) and asthma phenotypes with persistent wheezing, with or without pneumonia (18.7%) were the most common diagnosis and the reason for referral. In older children asthma phenotype with unresolved wheezing with or without pneumonia (76.5%) was the most common reason for referral.
The complimentary role of the public and the private health sector in the overall primary care of the people in this country is already documented.[5,6] However, the role of pediatricians and the utilization of pediatric primary care in the private health sector in this country has never been documented. Barbadians have a choice of accessing health care in the public health system which is free of charge, or in the private health care system where they pay for their service at the point of delivery. The comprehensive public health care system, through its network of primary health care centers popularly known as the Polyclinics spread across the island, provides a range of services for children including preventative care as well as curative care for acute and chronic conditions. The medical care in this setting is provided by doctors with MBBS degree, public health nurses and other paramedical staff only. In the private health care system, primary health care to children is provided by the private office/health centers of pediatricians of which there were 15 at the end of 2018. Some of these pediatricians also provide inpatient care to children at the only tertiary care hospital in this country and therefore their time in private office is limited. Of note, the PCPR for this country at the end of 2018 stood at 30 compared to the figure of 46.6 per 10000 children for the USA in 1992 (5). The private offices / heath centers of practitioners (doctors with MBBS degree only or doctors with additional higher degree in family medicine or emergency medicine) also provide primary care to the children of this country.[7]
The size of this solo pediatric practice at the WCMC, with close to three thousand enrolled children, is comparable to the number of children per pediatrician reported in studies from solo pediatric practices in the United States of America.[3,8,9] The mean annual enrolment of children at the WCMC constituted nearly one-twelfth of the mean annual live births in this country for the period extending from 2006 through 2018.[10] Given that there are another 14 such private pediatric practices, these figures would translate to a large proportion of children attending to pediatricians for their primary care in this country. A trend of an increasing proportion of children receiving their primary care form pediatricians have been previously reported.[11] Absence of pediatrician led services at the public health system may be a contributory factor for the high proportion of children seeking their primary care at the private pediatric clinics in this country.
We had a higher proportion of visits from infants as well those from under five years when compared with the finding from the United States of America.[9,12] However, Tsuda K et al. from Japan have reported a higher proportion of visits from infants in their solo pediatric practice.[13] The patient population seen in this setting declined steadily with advancing patient age.
Nearly two-thirds of the visits were paid for by the parents out-of-pocket as they had no health insurance coverage. This is in sharp contrast to the findings from developed countries where most children have health insurance coverage.[14] These findings from our study suggests that most parents are willing to pay for the health care of their children by a pediatrician. Overall, 8.5% of the children had multiple repeat (16 or more) visits and 1.1% had more than 50 visits during the 12 year follow up period. In a similar study from a solo private pediatric clinic in Japan, Tsuda K et al have reported 1.3% of their children having one or more visits per month on average during the three-year study period.[13] Of note, multiple repeat visits were significantly more likely form those who had health insurance than those without a health insurance.
Overall, only 7.7% of all the visits were for the well (preventative) care and the rest of the 92.3% of the visits were for problem-focused (curative) care. The proportion of well care visits in this study is lower than that reported in a recent study from the USA.[15] More importantly, even from among the under-1 year and under-5 year children visits, only 13.5% and 8.8% of the visits respectively, were for well care. These figures were much lower than those reported for these age groups from the USA.[15] Lower proportion of well care visits seen in out setting may be due to the fact that immunization services are freely available through the public health system and parents tend to use these services in preference to the private health system where these services tend to be more costly than the routine consultation for acute problem based visits. Another notable finding was that over ninety percent of all the visits to this center were for acute problems and less than 5 % of all visits were follow up visits for various chronic problems in children.
Overall, ARC, Upper Respiratory tract infections and asthma phenotypes were the three most frequent diagnosis given for the visits to this center. This was also true for the visits from under-5 year children as well as for the visits form children in the 5- 15 years age group. Similar findings have been reported in another study from a solo pediatric practice in Japan.[13] similarly, problems of the Respiratory system, especially infectious conditions, were reported as being the most common in other studies, but at a smaller proportion.[16–18] However, the most significant finding from this study was the high proportion of visits, especially from the older children, for where diagnosis of an asthma phenotype was unassociated with the diagnosis of infections of the respiratory tract but associated with a diagnosis of ARC. These are the children who are more likely to have an atopic asthma phenotype and are more likely to continue to wheeze as adults. These findings are in keeping with the high number of Emergency Room visits for acute asthma and the high proportion of infants and toddlers with recurrent wheezing reported from this country.[19,20]
Overall, less than 2.5% of all visits required referral for hospitalization. Asthma with unresolved wheezing with or without pneumonia was the most common reason for referral and accounted for over two-thirds of all referrals. These findings are in keeping with the findings from a previous study of hospitalization among children in this country where Asthma phenotypes one of the most common discharge diagnosis.[21]
This audit of the uptake of primary care by children attending a private pediatric center revealed that a significant proportion of children are enrolled for pediatrician-driven primary care from infancy. Over two-thirds of all the visits were from the under-5 year’s children. Close to two-thirds of these visits were paid for by out-of-pocket payment from their parent in absence of any health insurance. Over ninety percent of all visits in this setting were problem-focused.
The major limitation of this study was that the patients enrolled at this private self-paying medical center may have at times received care at the public health care Centre for want of funds or otherwise and therefore some of the data on the morbidity in this cohort of children followed up at this Centre may have been missed.
Subscribe now for latest articles and news.