Journal of Medical Sciences and Health
Year: 2022, Volume: 8, Issue: 1, Pages: 35-41
Original Article
Suhasini Dehury1, Haribhakti Seba Das2, Abhipsa Patra3, Rashmita Pradhan4
Irritable Bowel Syndrome (IBS) is a functional bowel disorder characterized by abdominal pain or discomfort and altered bowel habits in absence of detectable structural abnormalities with worldwide incidence of 10-20%. According to Rome IV criteria subtypes of IBS can be IBS-D, IBS-C and IBS-M. Both non pharmacological and pharmacological therapy are available for IBS. Earlier Peppermint Oil (PO) was used in different types of abdominal pain. An oral formulation of PO is used in patients of IBS to improve symptoms. Hence the study was conducted to assess the efficacy of Peppermint Oil in IBS patients.METHOD: A prospective randomized, placebo-controlled study of 6month was done in Dept. of Pharmacology and Gastroenterology, SCBMCH, Cuttack. A total of 60 IBS patients(18-60yr) were included in the study. They were divided randomly into two groups by lottery system. Gr-1 received PO 180mg TDS 60 min before breakfast, lunch, dinner and Gr-2 received placebo. The baseline and follow-up parameters of Total IBS symptom Score (TISS) were recorded at 0hr, 24hr and 4wks of treatment in both groups and Pain was assessed using Numeric Rating Scale. Statistical analysis were done using Mann-Whitney Test and Wilcoxon signed ranked Test. RESULTS: There was significant reduction in TISS and PAIN score at 24hr and 4weeks with Peppermint Oil from the baseline with Placebo.CONCLUSION : Peppermint oil was found to be effective in IBS patients.
Keywords: Irritable Bowel Syndrome, Peppermint Oil, Total IBS symptom score, Numeric Pain rating scale
Irritable Bowel Syndrome (IBS) is a common functional bowel disorder with a Worldwide prevalence of 10 -15%.[1–3] Prevalence in India is 4% - 7%[4] and there is female predominance affecting in late 4th decade of life. [2] According to ROME IV Criteria IBS is defined as, patients having recurrent abdominal pain (≥1day/week on average, in the previous 3 months) with an onset of ≥ 6 months before making the diagnosis.[5] In most of the patients, abdominal pain is mostly associated with at least two of the following three symptoms: -1) Pain related todefecation 2) Change in stool frequency 3) Change in form of stool. [6,7] Basing upon signs and symptoms IBS can be classified as three subtypes: 1) IBSC constipation; 2) IBS-D diarrhoea and 3)IBS-M mixed types. [8] Management of IBS is still a clinical challenge to the physicians.[9] Both non pharmacological and pharmacological treatments are the main stay of treatment options available to Patients of IBS. Non pharmacological strategy includes life style modification, dietary alteration and exercise,[10] whereas Pharmacological treatment includes use of Anticholinergics, Antidiarrheal, Prokinetic agents and newer drugs like Rifaximine, Alosetron, and Lubiprostone.[11–14] But, Pharmacotherapy of IBS is still far from satisfaction[7] . Peppermint Oil (PO) and its active ingredient L-menthol was approved in Europe and America as frontline IBS pharmacotherapy.[15,16] Due to its diverse receptor interactions it produces variety of pharmacological actions, which may found to be beneficial in treatment of IBS.[17]
The calcium channel blocking property of peppermint oil causes smooth muscle relaxation,[18,19] with the help of TRPA1 and TRPM8 agonistic properties it can modulate visceral sensations.[20,21] In addition to above cited activities it also has antimicrobial, anti-fungal and by anti-inflammatory properties which helps in modulating immune system.[18,22,23] But there remains paucity of Indian data regarding the effectiveness of Peppermint Oil for improving symptoms in IBS patients. With the above background the study was undertaken to assess the effectiveness of Peppermint Oil in patients with IBS with the following objectives:
1. To compare the Effect of Peppermint Oil with Placebo on Total IBS Symptom Score (TISS).
2. To compare the Effect of Peppermint Oil with Placebo on Pain using Numeric Pain rating Scale (NRS).
This randomized, open label, prospective, Placebo controlled Study was conducted in the Department of Pharmacology and Gastroenterology, SCB Medical college and hospital, Cuttack for a period of six Months (June - November 2018). The ethical clearance was taken from institutional ethics committee bearing the clearance number ECR/84/Inst/OR/2013/RR-20. Patients with IBS attending the Gastroenterology OPD of SCBMCH satisfying inclusion and exclusion criteria were included in the study after taking informed consent.
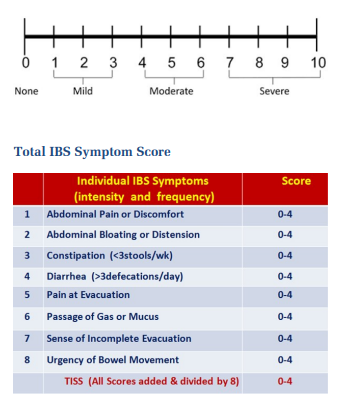
All patients with any of the three subtypes of IBS between 18-60 years of both genders, with an average daily IBS related abdominal pain rating ≥4 on 0- 10 scale (Numeric Rating Scale) and a Total IBS Symptom Score (TISS) ≥2 on a 0-4 scale were included in the study.
Patients with history of any Organic Gastrointestinal Disorder including Intestinal Obstruction, Adhesions, Perforation, Toxic Megacolon, Fecal Impaction, Alcohol Abuse, Ischemic Colitis, Cholecystitis, Cholecystectomy were excluded from the study.
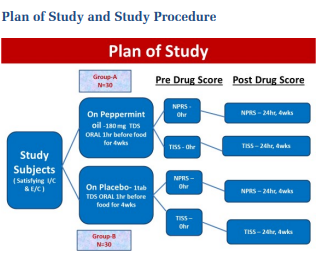
Sixty Patients registered in Gastroenterology OPD (Friday & Monday of every week) with IBS were randomly divided into two groups adopting the lottery method by a faculty of Department of Community Medicine of SCB MCH,
Cuttack, who was not involved in the conduction of the research work. Group -1 received peppermint oil orally at a dose of 180mg TDS 60minutes before breakfast, lunch and dinner. Group-2 received placebo in the same manner. Baseline data were noted. A Follow up was done after 24hr and 4wk of treatment period. Pain and symptoms were measured on morning before medication at 0hr as pre drug score and after 24hr & 4wk of medication as post drug score. Consent was taken in written form from all the eligible participants using the available consent form both in English and local language i.e Odia (Both the forms are given as attachments). All data were recorded in pre designed Case Study Proforma.
Peppermint oil the extract of Mentha plant and it contains menthol and other ingredients, among all the active ingredient is L- Menthol.[18] The formulation of PO used in the current study was enteric coated capsule 30 mg/cap manufactured by Healthvit drugs and chemicals. Placebo used in this study contains 100% dietary fibre[24] and available in the market as Psyllium husk.
Baseline characteristics like age, gender, IBS types were summarized using number and percentage whereas TISS and NPRS were summarized as mean±SD. TISS and NPRS were noted as mean±SD for follow up after treatment and compared statistically. Then appropriate statistical tests e.g Chi square test, Wilcoxon signed rank test and Mann Whitney test were used for data comparison.
Wilcoxon signed rank test was used for intra group comparison from baseline and Mann Whitney test was used for inter group comparison between PO and Placebo group.
Results from previous clinical trials[6,24–28] of PO for IBS were used for sample size determination. This study was planned to have > 95% power to show 1-point difference in changes from baseline symptoms between the PO group and Placebo group. This calculation assumes two- sided tests at 0.05 alpha level and common standard deviation of 1.0. With this 60 patients were eligible for randomization. Randomization was done using lottery method, where those coming under heads included in PO group and those coming under tails included in Placebo group. This was open label i.e no blinding was done. The sampling method used was simple random sampling.
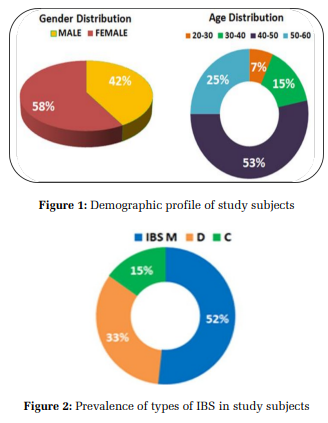
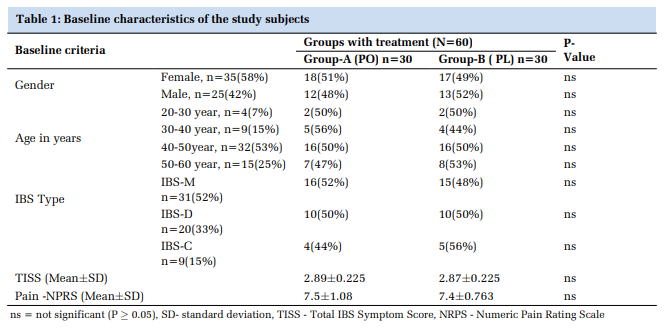
Patients: The patients satisfying the inclusion criteria were randomized to PO (n=30) or placebo (n=30) treated groups. They were well distributed in both PO and Placebo treated group. No significant difference between baseline data was found in patients of both the groups (Table 1). Mean age was 36.4 years (standard deviation ± 16.8) with a range of 20 to 60 years. 58% were female and 42% were male (Figure 1). 52% of patients had IBS-M and 33% of patients had IBS-D and 15% had IBS-C (Figure 2). Baseline TISS and Pain scores along with the follow up data after treatment of 24hrs and 4weeks with PO and Placebo are shown in Table 2 and Table 3.
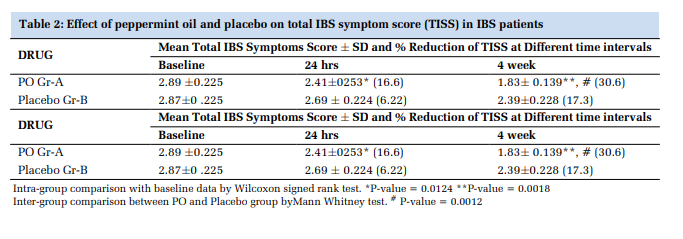
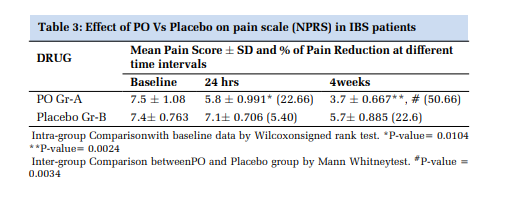
The TISS and pain score were calculated at base line considered as pretreatment score. The 24hrs and 4weeks values were taken after randomization and administration of first dose and subsequent dose were taken as post treatment score. The primary end point, the decrease (improvement) in TISS and Pain score at 4weeks compared to baseline, were 30.6% and 50.66% in patients randomized to PO (Group-A) compared to 17.3% and 22.6% in patients randomized to placebo (Group-B). The improvement was found to be statistically significant. Similarly, at 24hrs, the decrease in TISS and pain score from base line were 16.6% and 22.66% respectively in GroupA and 6.22% and 5.4% in Group-B. In Group-A, the improvement was significantly higher than Group-B.
The study revealed, a predominance of mixed variety of IBS (52%) (fig-1a) with a female preponderance (58.3%) (fig-2). These findings were consistent with Cash BD et.al.[24] The total study population were divided into two groups as PO treated group (groupA) and placebo treated group (Group-B). The IBS
patients in group-A with PO treatment showed a statistically significant decrease in TISS score after 24 hrs (16.6%) and four weeks (36.65%) in comparison to its baseline values and placebo treated IBS patients i.e group-B. The scores were significantly reduced in PO treated (P value = 0.0018) patients. The above findings were corroborated with the findings of Cappello G et.al[6] , Cash BD et.al[24] and Capanni M et.al.[25] There was also significant improvement in TISS when compared between PO and Placebo treated group after 4weeks of treatment (P= 0.0012). This finding was similar to the findings of Cash BD et.al[24] and Pittler MH et.al.[27]
Pain was a primary symptom in our study patients. In addition to PO treated IBS Patients experienced a relief of abdominal pain after 24hrs. There was reduction in pain score after 24 hrs as well as after 1month of treatment with PO. With treatment for four weeks, there was a statistically significant reduction of pain score (50.66%) (*p value= 0.0024) observed in PO Group, when compared with placebo treated Group (fig- 4). These findings were consistent with the results of Liu JH et.al[26] and Dew MJ et.al.[28] In our study, there was significant reduction in pain after 4weeks of treatment with PO (P value= 0.0024) which was similar to findings of Rees WD et.al[29] and Merat S et.al[30]
, here the only difference was with study period which were 2weeks in Rees WD et.al. and 8weeks in Merat S et.al.
The possible mechanism of PO on relieving TISS and abdominal pain may be due to its smooth muscle relaxing effect,[18,19] anti-microbial effect and TRPA1 and TRPM8 agonist properties.[20,21] Peppermint oil appears to be well- tolerated treatment for symptomatic improvement in IBS. Peppermint oil’s main efficacy in IBS is through its ability to act as a spasmolytic agent, altering smooth muscle contraction in the GI tract. In addition, peppermint oil has also been shown to have activity as an antiinflammatory and anti-microbial agent suggesting respective potential efficacy modulating cytokine inflammatory pathways and/or gut micro biome effects on dietary exposures, intestinal sensory afferents or intestinal motility.[18,22,23]
Our study also has some limitations having small sample size, open label and short study period. So, in future, more of the multicentric studies with large sample size and with double blinding methods are required to have more accurate results. While longterm data on the efficacy of peppermint oil is not available, still clinicians may consider peppermint oil as a treatment option for those suffering from IBS.
Our study results demonstrated that the enteric coated capsule formulation of peppermint oil was associated with a rapid symptomatic improvement of symptoms associated with patients of different types of IBS. This was based on the significant change of TISS and Pain scale from baseline and after the treatment with PO over a period of 24hr and 4weeks of therapy. This formulation of Peppermint oil can be a promising addition for effective and rapidly acting pharmacotherapy for patients with IBS.
Subscribe now for latest articles and news.