Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.v12.i2.26.54
Year: 2026, Volume: 12, Issue: 2, Pages: 178-190
Review Article
Krishnaa S Upadhye 1, Paritosh Tayade 2
1Director, Clinical Pharmacology & Drug Development, Krescent Medical Research Pvt. Ltd., Pune, Maharashtra, India.
2Clinical Pharmacology & Drug Development, Krescent Medical Research Pvt. Ltd., Pune, Maharashtra, India.
Address for correspondence: Krishnaa S Upadhye, Director, Clinical Pharmacology & Drug Development, Krescent Medical Research Pvt. Ltd., Pune, Maharashtra, India.
E-mail: [email protected]
Received Date:05 February 2026, Accepted Date:22 May 2026, Published Date:12 June 2026
Inter-individual variability in response to anaesthetic and analgesic drugs remains a major challenge in perioperative medicine, often leading to unpredictable efficacy and adverse events despite standardized dosing. Pharmacogenomics provides a mechanistic framework to explain this variability by linking genetic differences to drug metabolism, transport, and receptor sensitivity. This review summarizes current evidence on pharmacogenomic influences in anaesthesia, focusing on clinically relevant gene–drug interactions involving propofol, opioid analgesics, and neuromuscular blocking agents. A targeted literature search of PubMed, Embase, and the Cochrane Library identified 28 relevant studies for qualitative synthesis. Evidence indicates that polymorphisms in genes such as CYP2B6, UGT1A9, OPRM1, CYP2D6, and BCHE significantly influence drug response, including variability in anaesthetic dose requirements, analgesic efficacy, and risk of adverse events. The strongest clinical evidence exists for opioid metabolism and succinylcholine-related apnea, while evidence for adjunct agents remains limited and heterogeneous. Although pharmacogenomics holds promise for individualized perioperative care, routine clinical implementation is constrained by limited high-quality trials, cost, and logistical challenges. Future research should focus on prospective studies and integration with clinical decision-support systems to enable precision anaesthesia.
Key Message: Although variability in anaesthetic and analgesic response is common, pharmacogenomic application remains limited. This review identifies clinically relevant gene–drug interactions and highlights pathways for safe, individualized perioperative anaesthetic practice.
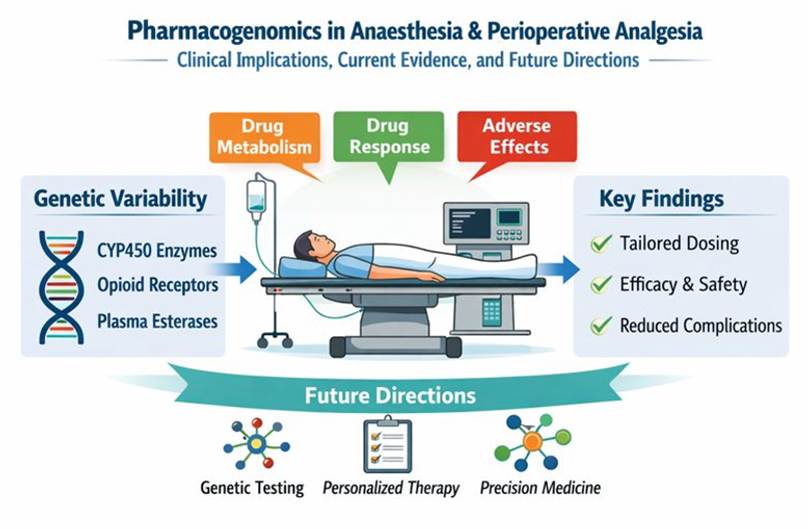
This graphical abstract summarizes how pharmaco- genomic variability influences anaesthetic and perioperative analgesic drug response. Genetic differences affecting drug metabolism, transport, and receptor sensitivity contribute to variability in efficacy, safety, and recovery, informing future precision-based perioperative anaesthesia.
Inter-individual variability in response to anaesthetic and analgesic drugs remains a major challenge in perioperative practice. Even when standardized protocols are followed, patients may demonstrate substantial differences in anaesthetic depth, analgesic requirements, hemodynamic stability, and recovery profiles. This variability is clinically significant, as both under- and over-dosing of anaesthetic agents are associated with adverse outcomes, including intraoperative awareness, hypotension, delayed emergence, postoperative delirium, and inadequate pain control[1-3]. Intravenous anaesthetic agents such as propofol, opioid analgesics, and neuromuscular blocking agents are particularly susceptible to such variability due to their narrow
therapeutic indices and complex pharmacokinetic–pharmacodynamic relationships[4].
Conventional anaesthetic dosing strategies are primarily based on demographic and physiological parameters such as age, body weight, sex, and organ function. Although these factors explain part of the variability, they do not adequately account for the wide inter-individual differences observed in drug response. Clinical monitoring tools, including processed electroencephalography and hemodynamic parameters, enable real-time titration of anaesthetic depth but remain reactive rather than predictive[5]. As a result, anaesthetic management often involves empirical dose adjustments, which may increase the risk of adverse outcomes, particularly in vulnerable populations such as elderly patients and those with multiple comorbidities[6].
Pharmacogenomics has emerged as a key factor contributing to variability in drug response by linking genetic variation to differences in drug metabolism, transport, and receptor sensitivity. In the case of propofol, polymorphisms in enzymes such as CYP2B6 and UGT1A9 influence drug clearance and plasma concentrations. For opioid analgesics, genetic variations in the μ-opioid receptor gene (OPRM1) affect receptor binding and analgesic efficacy, while CYP2D6 polymorphisms significantly alter the metabolism of drugs such as codeine and tramadol. Similarly, genetic variation in the butyrylcholinesterase (BCHE) gene is well established as a cause of prolonged neuromuscular blockade following succinylcholine administration[7-9]. These gene–drug interactions provide a biological basis for the variability observed in perioperative anaesthesia.
The application of pharmacogenomics in anaesthesia offers several potential advantages. It may enable individualized drug selection and dosing, improve therapeutic efficacy, and reduce the risk of adverse drug reactions. This approach is particularly relevant in high-risk populations, including elderly patients, critically ill individuals, and those undergoing major surgical procedures. However, several limitations currently restrict its routine clinical implementation. These include the cost of genetic testing, limited availability of rapid point-of-care genotyping, lack of large prospective clinical trials, and challenges in integrating genetic data into perioperative workflows[10-12].
Given these considerations, there is a need for a structured evaluation of existing evidence and its clinical relevance. The objective of this review is to provide a comprehensive and evidence-based overview of pharmacogenomics in anaesthesia and perioperative analgesia, with a specific focus on key drug classes, including propofol, opioid analgesics, and neuromuscular blocking agents. In addition, this review discusses clinical implications, current practice, limitations of available evidence, and future directions for integrating pharmacogenomics into perioperative care.
Literature search strategy
A targeted literature review was conducted to identify relevant evidence on pharmacogenomic influences on anaesthetic and perioperative analgesic drug response. Electronic searches were performed in PubMed, Embase, and the Cochrane Library from database 2019 to 2025. The search strategy used combinations of keywords and controlled vocabulary related to pharmacogenomics, pharmacogenetics, anaesthesia, perioperative analgesia, propofol, opioids, neuromuscular blocking agents, and sedative–analgesic adjuncts. In addition, reference lists of key articles were manually screened to identify potentially relevant studies not captured through database searches, in accordance with established guidance for transparent literature searching[11, 12].
Study selection and eligibility criteria
The database search yielded 1,060 records, including 412 from PubMed, 538 from Embase, 74 from the Cochrane Library, and 36 from manual reference screening. Prior to screening, 286 records were removed, comprising 220 duplicate records, 60 records marked as ineligible by automation tools, and 6 records removed for other predefined reasons, consistent with contemporary recommendations on the use of automation in evidence synthesis. The remaining 774 records underwent title and abstract screening, during which 450 records were excluded for lack of relevance. Of the 324 reports sought for retrieval, 209 could not be retrieved, leaving 115 full-text articles assessed for eligibility. Studies were excluded at full-text review if they were non-human or in vitro investigations, case reports or small case series, exploratory genetic association studies without clinical outcomes, or articles lacking sufficient methodological detail. Ultimately, 28 studies met the eligibility criteria and were included in the review, with the study selection process depicted using a PRISMA-style flow diagram[11].
Data extraction
Data were extracted manually from included studies and encompassed study design, patient population, anaesthetic or analgesic agent evaluated, genetic variants investigated, and clinically relevant outcomes such as drug dose requirements, anesthetic depth, analgesic efficacy, recovery characteristics, and adverse events. Where multiple publications addressed similar gene–drug interactions, the most comprehensive or methodologically robust study was prioritized, following established principles for clinical evidence appraisal.
Narrative data synthesis approach
Given the heterogeneity in study designs, genetic variants assessed, drug classes evaluated, and outcome measures reported, a narrative synthesis approach was employed. Quantitative pooling and meta-analysis were not performed. Findings were synthesized qualitatively with emphasis on biological plausibility, consistency of evidence, and relevance to perioperative anaesthetic practice. This approach aligns with recommended methodologies for narrative reviews and avoids inappropriate statistical aggregation of heterogeneous data[13, 14].
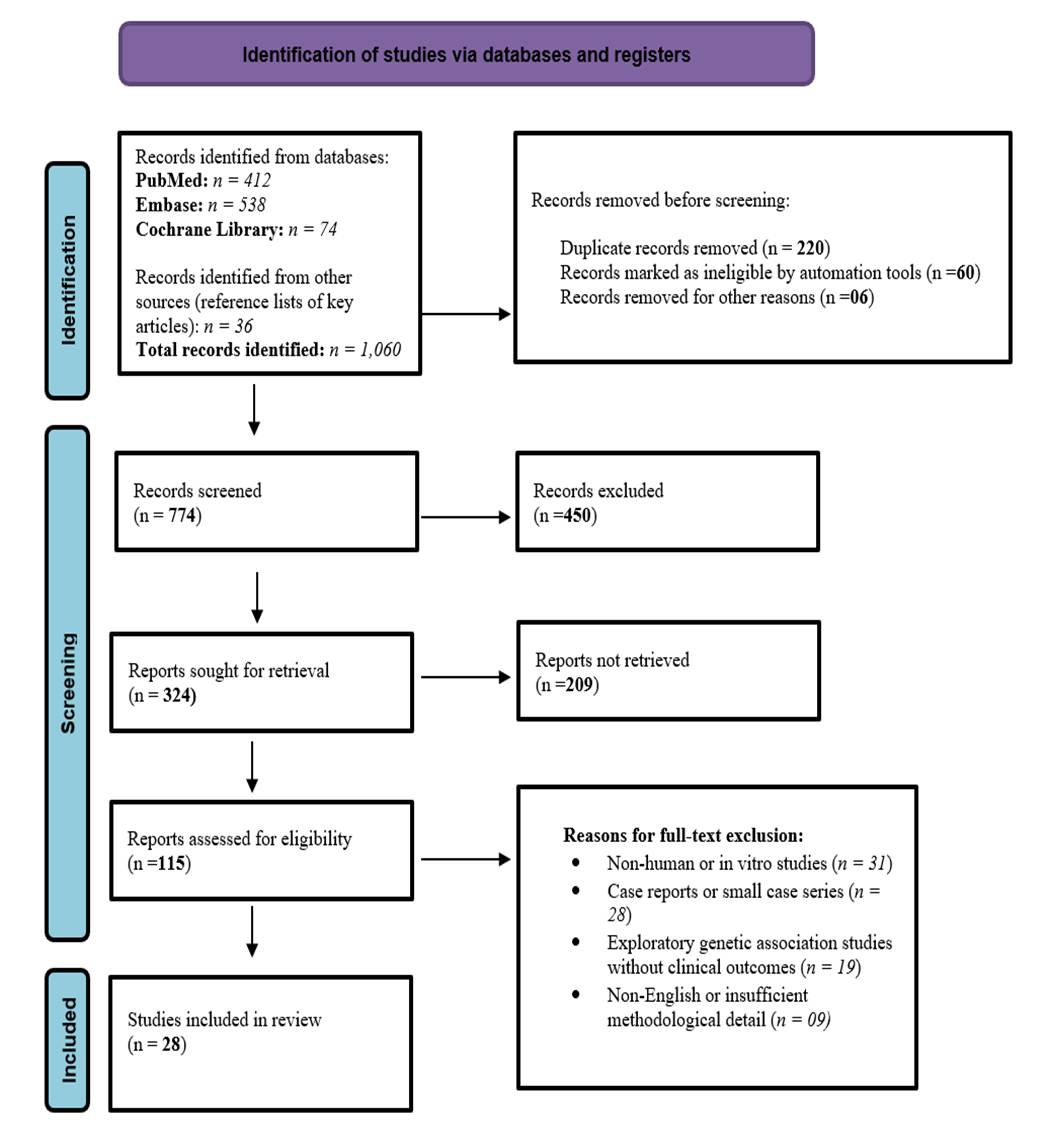
PRISMA-style flow diagram illustrating the identification, screening, eligibility assessment, and inclusion of studies evaluating pharmacogenomic influences on anaesthetic and perioperative analgesic drug response. Records were identified through database searches of PubMed, Embase, and the Cochrane Library. Following removal of duplicates, titles and abstracts were screened, and full-text articles were assessed for eligibility based on predefined inclusion and exclusion criteria. Studies meeting eligibility criteria were included for qualitative narrative synthesis.
Propofol
Genetic determinants: Propofol is the most widely used intravenous anaesthetic agent for induction and maintenance of general anaesthesia. It undergoes extensive hepatic metabolism primarily through glucuronidation by uridine 5′-diphospho-glucuronosyltransferase (UGT1A9) and oxidative metabolism mediated by cytochrome P450 enzymes, particularly CYP2B6 and CYP2C9[15, 16]. Genetic polymorphisms in these enzymes contribute significantly to inter-individual variability in propofol clearance and plasma concentrations.
Among these, CYP2B6 polymorphisms have been most extensively studied. The CYP2B6*6 allele is associated with reduced enzymatic activity, leading to decreased metabolic clearance and higher propofol exposure[17]. Clinical pharmacokinetic studies have demonstrated that individuals carrying reduced-function CYP2B6 variants require lower infusion rates to achieve comparable anaesthetic depth[18]. Variants in CYP2C9 may further influence oxidative metabolism, particularly in individuals with combined polymorphisms[19].
| Gene | Key polymor- phism |
Functional effect |
Clinical implication |
Ref. |
|---|---|---|---|---|
| CYP2B6 | *6 (516G>T, 785A>G) | Reduced metabolism | Higher plasma levels, lower dose requirement | [17, 18] |
| CYP2C9 | *2, *3 | Reduced oxidative metabolism | Modest reduction in clearance | [15, 19] |
| UGT1A9 | −440C>T, −331T>C | Altered glucuronidation | Variability in elimination and recovery | [15, 16] |
| GABRA1 / GABRA2 | SNPs | Altered receptor sensitivity | Variability in anaesthetic depth | [20, 21] |
| ABCB1 | 3435C>T | Altered drug transport | Variability in CNS exposure | [24] |
Note: The asterisk (*) indicates allele nomenclature used to describe specific genetic variants (haplotypes) in pharmacogenomics.
[Table. 1] summarizes key genetic polymorphisms influencing propofol pharmacokinetics and pharmacodynamics. Variants in metabolic enzymes (CYP2B6, CYP2C9, UGT1A9) primarily affect drug clearance and plasma concentrations, while polymorphisms in receptor (GABRA1/GABRA2) and transporter (ABCB1) genes contribute to variability in anaesthetic sensitivity, depth, and central nervous system exposure.
Genetic determinants and mechanisms
In addition to propofol, pharmacogenomic variability has been described for other intravenous anaesthetic agents, although evidence is comparatively limited. Thiopental metabolism is influenced by CYP2C19 polymorphisms, with poor metabolizers demonstrating prolonged sedation[28]. Etomidate has been associated with variability in adrenal suppression linked to CYP11B1-related pathways[29].
Ketamine metabolism is mediated primarily by CYP2B6 and CYP3A4, and genetic variation in these enzymes may result in reduced clearance and prolonged pharmacological effects[30]. Similarly, midazolam metabolism is influenced by CYP3A5 polymorphisms, where reduced enzymatic activity may lead to prolonged sedation and delayed recovery[31].
Clinical implications
The clinical impact of pharmacogenomic variability in these agents includes differences in duration of action, recovery profiles, and susceptibility to adverse effects. However, compared with propofol, the evidence remains limited and inconsistent. Most studies are based on small cohorts or non-perioperative settings, limiting generalizability.
At present, pharmacogenomic testing is not routinely used to guide the administration of these agents. Further research is required to establish clinically meaningful genotype–phenotype relationships and to evaluate the potential role of genotype-guided dosing strategies.
| Drug | Gene | Effect | Clinical implication |
Ref. |
|---|---|---|---|---|
| Thiopental | CYP2C19 | Reduced metabolism | Prolonged sedation | [28] |
| Etomidate | CYP11B1 | Altered steroid synthesis | Variable adrenal suppression | [29] |
| Ketamine | CYP2B6 / CYP3A4 | Reduced metabolism | Prolonged action, psychomimetic effects | [30] |
| Midazolam | CYP3A5 | Reduced clearance | Delayed recovery | [31] |
[Table. 2] outlines pharmacogenomic factors associated with commonly used intravenous anaesthetic agents other than propofol. Genetic variability in drug-metabolizing enzymes influences duration of action, recovery profiles, and risk of adverse effects, although current clinical evidence remains limited and does not support routine genotype-guided dosing.
Genetic determinants
Opioid analgesics remain a cornerstone of perioperative pain management; however, significant inter-individual variability exists in both analgesic efficacy and adverse effect profiles. A major contributor to this variability is genetic variation in the μ-opioid receptor gene (OPRM1), which encodes the primary pharmacological target of most opioids.
The most extensively studied polymorphism, OPRM1 A118G (rs1799971), has been associated with altered receptor expression and ligand binding affinity. Carriers of the G allele typically demonstrate reduced receptor function, which may result in decreased analgesic response[32, 33]. Clinical studies have consistently reported higher opioid dose requirements and increased use of rescue analgesia in such individuals following surgical procedures[34]. Meta-analyses further suggest that this polymorphism contributes to variability in postoperative pain scores and opioid consumption, although its clinical effect size remains modest and influenced by surgical and therapeutic factors[35].
In addition to receptor-related variability, genetic differences in drug metabolism play a central role in opioid response. The cytochrome P450 enzyme CYP2D6 is responsible for the bioactivation of several opioids, including codeine and tramadol. Variations in CYP2D6 result in distinct metabolizer phenotypes, ranging from poor to ultra-rapid metabolizers, which significantly influence drug efficacy and toxicity[37, 38].
Pharmacogenetic mechanisms
Pharmacogenetic variability in opioid response arises from multiple mechanisms, including receptor sensitivity, drug metabolism, and transport across the blood–brain barrier.
CYP2D6 polymorphisms are particularly important in clinical practice. Poor metabolizers exhibit reduced conversion of prodrugs such as codeine and tramadol into their active metabolites, leading to inadequate analgesia. In contrast, ultra-rapid metabolizers may produce excessive active metabolites, increasing the risk of opioid toxicity, including respiratory depression[37-39]. These findings have led to regulatory warnings and recommendations against the use of certain opioids in high-risk genotypes[40].
Polymorphisms in CYP3A4 and CYP3A5 may influence the metabolism of opioids such as fentanyl and oxycodone, contributing to variability in drug clearance and duration of action, although the clinical evidence is less consistent[41].
Drug transporters also play a role in opioid pharmacodynamics. Variants in the ABCB1 gene, encoding P-glycoprotein, may affect drug transport across the blood–brain barrier, thereby altering central nervous system exposure and influencing both analgesic efficacy and adverse effects[42]. Additionally, polymorphisms in genes such as COMT may modify pain perception and opioid requirements by affecting catecholamine metabolism[35, 45].
Clinical implications
Genetic variability in opioid pharmacokinetics and pharmacodynamics has important implications for perioperative analgesia and patient safety. Differences in receptor sensitivity and metabolic capacity can lead to variability in opioid dose requirements, analgesic effectiveness, and risk of adverse events, including respiratory depression, excessive sedation, and postoperative nausea and vomiting[43].
Genotype-guided opioid prescribing has been proposed as a strategy to improve safety and efficacy. The Clinical Pharmacogenetics Implementation Consortium has issued evidence-based recommendations for CYP2D6-guided opioid use, particularly for codeine and tramadol, providing a framework for personalized analgesic therapy[44].
In current clinical practice, pharmacogenomic testing is not routinely performed in anaesthesia. However, it may be considered in selected high-risk patients, such as those with a history of opioid-related adverse effects or inadequate analgesic response. Integration of pharmacogenomic data with clinical monitoring and multimodal analgesic strategies may enhance perioperative pain management while minimizing risk[45].
| Opioid | Gene | Functional effect |
Clinical implication |
Ref |
|---|---|---|---|---|
| Morphine | OPRM1 | Reduced receptor expression (A118G) | Reduced analgesia, higher dose requirement | [32-35] |
| Morphine | ABCB1 | Altered BBB transport | Variable CNS exposure, sedation | [41, 42] |
| Fentanyl | CYP3A4 / CYP3A5 | Reduced metabolism | Prolonged effect, respiratory risk | [41, 43] |
| Oxycodone | CYP2D6 | Reduced activation | Reduced analgesia or toxicity | [37, 38] |
| Tramadol | CYP2D6 | Impaired activation | Poor analgesia or increased toxicity | [37-40] |
| Codeine | CYP2D6 | Altered bioactivation | Treatment failure or toxicity | [38-40] |
| Multiple opioids | OPRM1 | Altered receptor sensitivity | Variable opioid requirement | [32, 36] |
| Multiple opioids | COMT | Altered pain modulation | Increased pain sensitivity | [35, 45] |
Despite promising evidence, routine implementation of pharmacogenomic-guided opioid therapy is limited by variability in study findings, lack of large prospective trials, and logistical challenges. Further research is required to establish its clinical utility and cost-effectiveness in perioperative settings.
[Table. 3] summarizes key pharmacogenomic factors influencing opioid analgesic efficacy and safety. Variants in receptor genes (OPRM1), drug-metabolizing enzymes (CYP2D6, CYP3A4/5), and transporters (ABCB1) contribute to variability in analgesic response, opioid requirements, and risk of adverse effects, supporting the potential role of individualized opioid therapy.
Genetic determinants
Neuromuscular blocking agents (NMBAs) are essential in anaesthetic practice for facilitating tracheal intubation and optimizing surgical conditions. Among these, succinylcholine is widely used for rapid sequence induction due to its rapid onset and short duration of action. However, significant inter-individual variability in recovery from neuromuscular blockade has been well documented, primarily due to genetic variation in the butyrylcholinesterase (BCHE) gene[46].
Butyrylcholinesterase is responsible for the hydrolysis of succinylcholine. Functional polymorphisms in the BCHE gene result in reduced or absent enzyme activity, leading to prolonged neuromuscular blockade and apnea following standard dosing. Several phenotypic variants, including atypical, fluoride-resistant, and silent forms, have been described, all of which are associated with delayed recovery[47].
In contrast, pharmacogenomic data for non-depolarizing neuromuscular blocking agents such as rocuronium, vecuronium, and cisatracurium remain limited. Although genetic factors have been proposed to influence drug disposition, their clinical significance is less clearly established[49].
Pharmacogenetic mechanisms
The pharmacogenetic variability of succinylcholine is primarily driven by reduced enzymatic hydrolysis due to BCHE deficiency. Patients with deficient or dysfunctional enzyme activity exhibit prolonged persistence of succinylcholine at the neuromuscular junction, resulting in sustained depolarization and extended paralysis. The severity of this effect varies depending on the specific genotype and degree of enzyme deficiency[46-48].
For non-depolarizing NMBAs, proposed mechanisms include genetic variation in hepatic transporters and metabolizing enzymes that may influence drug clearance. Polymorphisms in genes such as ABCB1 and CYP3A4/5 have been suggested to affect rocuronium pharmacokinetics; however, findings are inconsistent and lack robust clinical validation[49].
Agents such as cisatracurium undergo Hofmann elimination, a non-enzymatic process dependent on physiological conditions rather than genetic factors. As a result, pharmacogenomic influence on these agents is minimal, highlighting the predominance of non-genetic determinants in their metabolism[50].
Clinical implications
Pharmacogenomic variability in NMBAs has the greatest clinical relevance in the context of succinylcholine use. Patients with BCHE deficiency may experience prolonged neuromuscular blockade and apnea, which can lead to delayed recovery and require extended mechanical ventilation if not promptly recognized[48].
Preoperative identification of at-risk individuals, including those with a personal or family history of prolonged paralysis following anaesthesia, is essential. In such cases, succinylcholine should be avoided, and alternative neuromuscular blocking agents should be considered[51].
When prolonged neuromuscular blockade occurs unexpectedly, management is primarily supportive and includes continued ventilation and sedation until neuromuscular function returns. Quantitative neuromuscular monitoring plays a critical role in early detection and safe recovery[52].
For non-depolarizing agents, pharmacogenomic-guided dosing is not currently recommended due to insufficient evidence. The availability of reversal agents such as sugammadex has improved the safety profile of aminosteroid NMBAs, although genetic factors influencing reversal response remain poorly defined[53].
Overall, while pharmacogenomics plays a well-established role in succinylcholine response, its clinical application in other neuromuscular blocking agents remains limited.
[Table. 4] summarizes known and proposed pharmacogenomic factors influencing the response to neuromuscular blocking agents. Clinically significant genetic variability is well established for succinylcholine through butyrylcholinesterase deficiency, whereas evidence for pharmacogenomic effects on non-depolarizing neuromuscular blockers remains limited and inconsistent. Vigilant neuromuscular monitoring and individualized clinical management remain central to perioperative safety.
| Agent | Gene | Functional effect |
Clinical implication |
Ref |
|---|---|---|---|---|
| Succinylcholine | BCHE | Reduced enzyme activity | Prolonged paralysis, apnea | [46, 47] |
| Succinylcholine | BCHE variants | Severe enzyme deficiency | Markedly prolonged blockade | [47, 48] |
| Rocuronium | ABCB1 (proposed) | Altered transport | Variable duration (uncertain) | [49] |
| Rocuronium | CYP3A4 / CYP3A5 | Altered metabolism | Possible prolonged effect | [49] |
| Cisatracurium | — | Non-enzymatic metabolism | Predictable recovery | [50] |
| Vecuronium | SLCO1B1 (proposed) | Altered hepatic uptake | Possible variability | [49] |
| Rocuronium (reversal) | — | Variable response | Monitoring required | [52, 53] |
Genetic determinants
Adjunct analgesics and sedatives are widely used in perioperative practice to enhance analgesia, reduce opioid requirements, and improve recovery outcomes. However, inter-individual variability in response to these agents is commonly observed.
Dexmedetomidine, a selective α2-adrenergic receptor agonist, has been associated with genetic variability in receptor function. Polymorphisms in α2 adrenergic receptor genes, particularly ADRA2A and ADRA2C, have been implicated in differences in sedative response and hemodynamic effects[54, 55].
Ketamine, an NMDA receptor antagonist, is primarily metabolized by CYP2B6 and CYP3A4. Genetic variability in these enzymes may influence drug clearance and plasma concentrations[58]. In addition, polymorphisms affecting NMDA receptor subunits (e.g., GRIN genes) have been proposed to contribute to variability in analgesic and dissociative effects[59].
Intravenous lidocaine, increasingly used in perioperative analgesia, is metabolized mainly by CYP1A2 and CYP3A4. Genetic variation in these enzymes may affect plasma levels and toxicity risk, although clinical evidence remains limited[60].
Pharmacogenetic mechanisms
Pharmacogenomic variability in adjunct agents is mediated through both pharmacokinetic and pharmacodynamic mechanisms.
For dexmedetomidine, genetic variation in ADRA2A and ADRA2C may alter receptor sensitivity, influencing sedative depth and susceptibility to adverse effects such as bradycardia and hypotension[56].
For ketamine, CYP2B6 and CYP3A4 polymorphisms may lead to reduced metabolic clearance, resulting in higher plasma concentrations and prolonged pharmacological effects. Variability in NMDA receptor function may further contribute to differences in analgesic response and psychomimetic effects[58, 59].
For lidocaine, polymorphisms in CYP1A2 and CYP3A4 may influence drug metabolism during prolonged infusion, potentially affecting both efficacy and risk of systemic toxicity[60].
Despite these mechanistic insights, the relationship between genotype and clinical response remains inconsistent, reflecting the influence of multiple interacting factors in perioperative settings.
Clinical implications
The clinical relevance of pharmacogenomics in adjunct analgesics and sedatives remains limited compared with primary anaesthetic agents and opioids. While genetic variability may contribute to differences in drug response, current evidence is insufficient to support routine genotype-guided dosing in clinical practice[57].
Adjunct agents are typically administered as part of multimodal anaesthetic regimens, making it difficult to isolate the specific contribution of genetic factors to
clinical outcomes. Additionally, most available studies are small, heterogeneous, and often conducted outside the perioperative setting, limiting generalizability[61].
Nevertheless, pharmacogenomic insights may be useful in selected clinical scenarios, such as unexplained variability in drug response or increased susceptibility to adverse effects. At present, these findings primarily inform research rather than routine perioperative decision-making.
Strengths and limitations of current evidence
The pharmacogenomic evidence for adjunct analgesics and sedatives demonstrates strong biological plausibility and is supported by emerging translational research. However, several limitations persist.
Most studies are underpowered and exhibit significant heterogeneity in study design, patient populations, dosing regimens, and outcome measures. Furthermore, the use of multimodal analgesic strategies introduces confounding factors that complicate interpretation of genotype–phenotype relationships.
Consequently, current evidence does not support routine pharmacogenomic testing for adjunct agents in anaesthesia. Well-designed prospective perioperative studies are required to establish clinically meaningful applications and evaluate the impact of genotype-guided strategies on patient outcomes[62].
[Table. 5] summarizes pharmacogenomic factors associated with commonly used adjunct agents in perioperative practice. While genetic variability in metabolic enzymes and receptor pathways may influence drug response, current evidence is limited and insufficient to support routine genotype-guided clinical application.
| Drug | Gene / Target | Functional effect | Clinical implication | Evidence |
|---|---|---|---|---|
| Dexmedetomidine | ADRA2A | Altered receptor sensitivity | Variability in sedation, bradycardia | Limited - moderate |
| Dexmedetomidine | ADRA2C | Altered sympathetic modulation | Variable hemodynamic response | Limited |
| Ketamine | CYP2B6 | Reduced metabolism | Increased plasma levels, prolonged effects | Moderate |
| Ketamine | CYP3A4 | Variable metabolism | Inter-individual variability in response | Limited - moderate |
| Ketamine | GRIN (NMDA receptor) | Altered receptor function | Variability in analgesia and dissociation | Limited |
| Lidocaine (IV) | CYP1A2 | Altered metabolism | Variability in plasma levels | Limited |
| Lidocaine (IV) | CYP3A4 | Reduced clearance | Potential toxicity risk | Limited |
| Multimodal use | Multiple pathways | Confounding genetic effects | Difficult to isolate impact | Low |
Current clinical practice
At present, pharmacogenomic testing is not routinely implemented in anaesthesia practice. Clinical decision-making continues to rely primarily on patient characteristics, physiological monitoring, and clinician experience. However, genotype-guided recommendations are available for selected drug classes, particularly opioids, where CYP2D6 testing may inform drug selection and dosing.
In most perioperative settings, pharmacogenomic information is used selectively rather than universally, typically in patients with unexplained variability in drug response or a history of adverse drug reactions. Despite increasing awareness, integration into routine anaesthetic workflows remains limited due to logistical, economic, and evidentiary constraints.
Preoperative feasibility and workflow integration
Successful integration of pharmacogenomics into anaesthesia practice depends on its incorporation into existing preoperative workflows. Elective surgical pathways provide the most feasible setting, allowing genetic testing to be performed during pre-anaesthetic evaluation alongside routine investigations.
Integration of genotype information into electronic health records and anaesthesia information systems is essential to ensure availability at the point of care[63]. Importantly, pharmacogenomic data should be presented in a clinically interpretable format with decision-support tools, rather than as raw genetic results, to facilitate practical application.
Turnaround time and clinical decision-making
Turnaround time is a key determinant of clinical utility. Conventional laboratory-based genotyping may require several days, limiting its use in urgent or emergency procedures. However, advances in rapid genotyping and point-of-care testing have reduced turnaround times to hours in some settings[64].
Pre-emptive pharmacogenomic testing represents a practical approach, where genetic data are obtained in advance and stored for future use across multiple perioperative encounters[65]. Clinical decision-making should integrate pharmacogenomic information with patient-specific factors, drug selection, and real-time physiological monitoring, rather than relying solely on genotype data.
Cost-effectiveness and infrastructure requirements
Cost and infrastructure requirements remain important considerations for widespread implementation. Although pharmacogenomic testing involves upfront investment, potential long-term benefits include reduced adverse drug reactions, improved drug efficacy, and shorter recovery times[66].
Implementation requires access to certified laboratories, trained personnel, clinical decision-support systems, and secure data management frameworks. Healthcare institutions with high surgical volumes and standardized perioperative pathways may be better positioned to adopt pharmacogenomic strategies effectively[67].
Ethical, regulatory, and consent considerations
Ethical and regulatory considerations are central to the implementation of pharmacogenomics in clinical practice. Key issues include informed consent, data privacy, and appropriate use of genetic information. Patients should be informed about the scope, limitations, and potential implications of genetic testing beyond the perioperative period[68].
Regulatory frameworks increasingly support the responsible use of pharmacogenomics when applied in an evidence-based and clinically justified manner[69]. Ongoing clinician education and multidisciplinary collaboration are essential to ensure ethical, safe, and effective integration into anaesthetic practice.
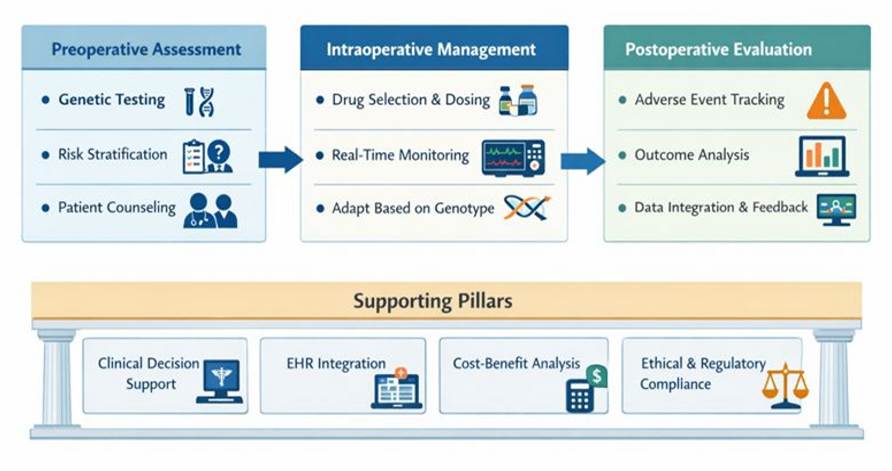
[Fig. 2] Illustrates a conceptual framework for integrating pharmacogenomic information into perioperative anaesthesia practice. Preoperative assessment includes genetic testing, risk stratification, and patient counseling. Intraoperative management incorporates genotype-informed drug selection and dosing, supported by real-time physiological monitoring. Postoperative evaluation focuses on adverse event surveillance, outcome assessment, and data feedback to inform future care. The framework is supported by clinical decision support systems, electronic health record integration, cost–benefit considerations, and ethical and regulatory compliance.
Point-of-care pharmacogenomic testing
The future clinical application of pharmacogenomics in anaesthesia will depend on the availability of rapid and accessible genetic testing. Advances in microarray-based and cartridge-driven platforms have significantly reduced turnaround times from days to hours, improving feasibility in perioperative settings, particularly for elective procedures[70].
Pre-emptive pharmacogenomic testing, performed prior to surgical scheduling and integrated into electronic health records, may represent the most practical approach. This strategy allows genotype data to be reused across multiple perioperative encounters without the need for repeated testing, thereby enhancing clinical utility and cost-effectiveness[71].
Integration with EEG-guided anaesthesia and PK–PD modeling
Integration of pharmacogenomic data with real-time monitoring and pharmacokinetic–pharmacodynamic (PK–PD) modeling represents a promising direction for precision anaesthesia. Genetic variability influencing drug metabolism and receptor sensitivity may contribute to differences in electroencephalographic responses and anaesthetic depth.
Combining genotype information with EEG-derived indices and physiological parameters may enable more accurate prediction of anaesthetic requirements and reduce the risk of excessive depth or burst suppression[72, 73]. However, these integrative approaches require validation through well-designed prospective clinical studies before routine implementation.
Role of artificial intelligence and clinical decision-support systems
Artificial intelligence (AI)–based clinical decision-support systems have the potential to translate complex pharmacogenomic data into actionable clinical recommendations. Machine learning models integrating genetic, clinical, and monitoring data may assist clinicians in optimizing drug selection and dose titration in real time[74].
Such systems should function as decision-support tools rather than autonomous systems, ensuring that clinical judgment and oversight remain central to patient care[75].
Priorities for future perioperative clinical trials
Future research should prioritize large, pragmatic perioperative trials evaluating genotype-guided strategies for commonly used agents such as propofol and opioids. These studies should focus on clinically meaningful endpoints, including anaesthetic stability, recovery characteristics, adverse drug events, and patient-centered outcomes.
Standardization of study design, outcome measures, and reporting will be essential to enable comparison across studies and strengthen the evidence base. Well-designed multicenter trials are required to establish the clinical utility and cost-effectiveness of pharmacogenomics in perioperative practice[76, 77].
This review highlights the emerging role of pharmacogenomics in explaining inter-individual variability in response to anaesthetic and analgesic drugs. Among the drug classes evaluated, the strongest clinical evidence exists for opioid pharmacogenetics and succinylcholine metabolism. Variants in CYP2D6 and OPRM1 have demonstrated consistent associations with opioid efficacy and safety, and genotype-guided recommendations have been proposed by organizations such as the Clinical Pharmacogenetics Implementation Consortium[78]. Similarly, BCHE polymorphisms are well established as a cause of prolonged neuromuscular blockade following succinylcholine administration[79].
In contrast, pharmacogenomic evidence for propofol and adjunct agents remains less consistent. Although associations between CYP2B6 polymorphisms and propofol metabolism have been reported, findings are heterogeneous and derived primarily from small or single-center studies[80]. Evidence for adjunct agents such as dexmedetomidine, ketamine, and lidocaine is largely based on mechanistic data and limited clinical studies, restricting their immediate clinical applicability.
Several limitations are evident across the current literature. Studies are often underpowered, heterogeneous in design, and lack standardization in outcome measures. Furthermore, anaesthetic response is influenced by multiple interacting factors, including patient characteristics, surgical variables, and environmental conditions, complicating the interpretation of pharmacogenomic effects. Similar challenges have been highlighted in recent reviews on perioperative pharmacogenomics and precision anaesthesia[81].
Despite these challenges, pharmacogenomics represents a promising approach for advancing precision anaesthesia. Integration with physiological monitoring, pharmacokinetic modeling, and clinical decision-support systems may enhance its clinical utility. Future research should focus on well-designed prospective trials to validate genotype-guided strategies and determine their impact on clinically meaningful perioperative outcomes.
Pharmacogenomics provides a biologically plausible explanation for inter-individual variability in response to anaesthetic and analgesic drugs, particularly for propofol, opioids, and succinylcholine. Evidence is strongest for opioid metabolism and BCHE-related neuromuscular blockade, while data for other agents remain limited and heterogeneous.
The main strengths of current evidence include clear mechanistic insights and growing clinical relevance for selected drugs. However, limitations such as small study sizes, lack of standardized outcomes, and limited prospective trials restrict widespread clinical application.
At present, pharmacogenomics is best applied selectively in high-risk patients or specific drug scenarios. Future progress will depend on large clinical trials, improved accessibility of genetic testing, and integration into perioperative decision-making systems.
Acknowledgments: The author expresses sincere gratitude to Krescent Medical Research Pvt. Ltd. for their invaluable guidance and support throughout the preparation of this manuscript.
Contributors: All authors contributed substantially to the conceptualization, drafting, and critical revision of this manuscript. Dr. Krishnaa S. Upadhye conceptualized the study, defined the design and intellectual content, conducted comprehensive literature searches, supervised clinical and experimental aspects, acquired relevant data, and took the lead in manuscript preparation, editing, and review. Dr. Upadhye also served as the guarantor for the integrity and accuracy of the work.
Ethical Approval Considerations: Institutional Review Board approval is not required for this study.
Consent to Participate: Patient consent is not required as there are no patients in this study.
Declaration of Conflicting Interest: Dr. Krishnaa S. Upadhye is the Director – Clinical Pharmacology & Drug Development at Krescent Medical Research Pvt. Ltd. This affiliation has been disclosed to the journal and the publisher. Krescent Medical Research Pvt. Ltd. had no role in the conceptualization, writing, or approval of this manuscript, and no funding was received from the company for this work. The views expressed in this review article are solely those of the author and do not necessarily reflect the views of Krescent Medical Research Pvt. Ltd.
Funding Statement: The authors have not declared a specific grant for this research from any funding agency in the public, commercial, or not-for-profit sectors.
1. Anesthesia and Cancer Recurrence. Anesthesiology. 2019; 130 (1). Available from: https://doi.org/10.1097/aln.0000000000002506
2. State-of-the-art anesthesia practices: a comprehensive review on optimizing patient safety and recovery. BMC Surgery. 2025; 25 (1). Available from: https://doi.org/10.1186/s12893-025-02763-6
3. Postoperative delirium: why, what, and how to confront it at your institution. Current Opinion in Anaesthesiology. 2020; 33 (5). Available from: https://doi.org/10.1097/aco.0000000000000907
4. Clinical Pharmacokinetics and Pharmacodynamics of Propofol. Clinical Pharmacokinetics. 2018; 57 (12). Available from: https://doi.org/10.1007/s40262-018-0672-3
5. Implication of age-related changes on anesthesia management. Saudi Journal of Anaesthesia. 2023; 17 (4). Available from: https://doi.org/10.4103/sja.sja_579_23
6. Anesthesia for geriatric patients. Anesthesia for Spine Surgery. 2011; 77 (2). Available from: https://pubmed.ncbi.nlm.nih.gov/21368727/
7. Pharmacogenomics of analgesics in anesthesia practice: A current update of literature. Journal of Anaesthesiology Clinical Pharmacology. 2018; 34 (2). Available from: https://doi.org/10.4103/joacp.joacp_319_17
8. Personalized Anesthetic Pharmacology. Personalized Medicine in Anesthesia, Pain and Perioperative Medicine. 2021; Available from: https://doi.org/10.1007/978-3-030-53525-4_3
9. Progress, Challenges, and Prospects of Research on the Effect of Gene Polymorphisms on Adverse Reactions to Opioids. Pain and Therapy. 2022; 11 (2). Available from: https://doi.org/10.1007/s40122-022-00374-0
10. Pharmacogenomics in anesthesia: tailoring anesthetic agents to genetic variations. Journal of Surgical Case Reports and Images. 2025; 8 (1). Available from: https://doi.org/10.31579/2690-1897/228
11. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021; Available from: https://doi.org/10.1136/bmj.n71
12. Cochrane Handbook for Systematic Reviews of Interventions. Chichester: Wiley. 2019; Available from: https://doi.org/10.1002/9781119536604
13. Time to challenge the spurious hierarchy of systematic over narrative reviews?. European Journal of Clinical Investigation. 2018; 48 (6). Available from: https://doi.org/10.1111/eci.12931
14. Lack of transparency in reporting narrative synthesis of quantitative data: a methodological assessment of systematic reviews. Journal of Clinical Epidemiology. 2019; 105 Available from: https://doi.org/10.1016/j.jclinepi.2018.08.019
15. Efficacy and safety of ciprofol versus propofol: a systematic review and meta-analysis. Frontiers in Pharmacology. 2023; 14 Available from: https://doi.org/10.3389/fphar.2023.1225288
16. Metabolic Profiles of Propofol and Fospropofol: Clinical and Forensic Interpretative Aspects. BioMed Research International. 2018; 2018 Available from: https://doi.org/10.1155/2018/6852857
17. Impact of the Cytochrome P450 2B6 (CYP2B6) Gene Polymorphism c.516G>T (rs3745274) on Propofol Dose Variability. European Journal of Drug Metabolism and Pharmacokinetics. 2016; 41 (5). Available from: https://doi.org/10.1007/s13318-015-0289-y
18. Effects of CYP2B6 Genetic Variants on the Propofol Dose and Response among Jordanian Arabic Patients Undergoing General Anesthesia. Current Drug Metabolism. 2022; 23 (14). Available from: https://doi.org/10.2174/1389200224666230130110350
19. Relationships between CYP1A2, CYP2C9, CYP2C19, CYP2D6 and CYP3A4 metabolic phenotypes and genotypes in a Nicaraguan Mestizo population. The Pharmacogenomics Journal. 2021; 21 (2). Available from: https://doi.org/10.1038/s41397-020-00190-9
20. Understanding the GABAA Receptor: Implications for Anesthesia and Beyond. Journal of Neuroanaesthesiology and Critical Care. 2023; 10 (03). Available from: https://doi.org/10.1055/s-0043-1778075
21. GABRA1 and GABRB2 Polymorphisms are Associated with Propofol Susceptibility. Pharmacogenomics and Personalized Medicine. 2022; 15 Available from: https://doi.org/10.2147/pgpm.s348170
22. Electroencephalogram monitoring during anesthesia and critical care: a guide for the clinician. Journal of Clinical Monitoring and Computing. 2024; 39 (2). Available from: https://doi.org/10.1007/s10877-024-01250-2
23. Intraoperative hypotension and the risk of postoperative adverse outcomes: a systematic review. British Journal of Anaesthesia. 2018; 121 (4). Available from: https://doi.org/10.1016/j.bja.2018.04.036
24. Clinical Importance of Potential Genetic Determinants Affecting Propofol Pharmacokinetics and Pharmacodynamics. Frontiers in Medicine. 2022; 9 Available from: https://doi.org/10.3389/fmed.2022.809393
25. Hemodynamic Effect of Different Doses of Fluids for a Fluid Challenge: A Quasi-Randomized Controlled Study. Critical Care Medicine. 2017; 45 (2). Available from: https://doi.org/10.1097/ccm.0000000000002067
26. CYP2B6 Genotype Guided Dosing of Propofol Anesthesia in the Elderly Based on Nonparametric Population Pharmacokinetic Modeling and Simulations. International Journal of Clinical Pharmacology & Toxicology. 2017; 6 (1). Available from: https://doi.org/10.19070/2167-910x-1700041
27. Personalized Medicine and Genomics: Challenges and Opportunities in Assessing Effectiveness, Cost-Effectiveness, and Future Research Priorities. Medical Decision Making. 2010; 30 (3). Available from: https://doi.org/10.1177/0272989x09347014
28. The pharmacogenetics of Medications Used in General Anesthesia. Pharmacogenomics. 2018; 19 (3). Available from: https://doi.org/10.2217/pgs-2017-0168
29. Osilodrostat for the treatment of Cushing syndrome: an update. Expert Review of Endocrinology & Metabolism. 2026; 21 (2). Available from: https://doi.org/10.1080/17446651.2026.2615346
30. Pharmacogenetic and drug interaction aspects on ketamine safety in its use as antidepressant ‐ implications for precision dosing in a global perspective. British Journal of Clinical Pharmacology. 2022; 88 (12). Available from: https://doi.org/10.1111/bcp.15467
31. Pharmacokinetics, Pharmacodynamics, and Side Effects of Midazolam: A Review and Case Example. Pharmaceuticals. 2024; 17 (4). Available from: https://doi.org/10.3390/ph17040473
32. Can Opioid-Free Anaesthesia Be Personalised? A Narrative Review. Journal of Personalized Medicine. 2023; 13 (3). Available from: https://doi.org/10.3390/jpm13030500
33. OPRM1, OPRK1, and COMT genetic polymorphisms associated with opioid effects on experimental pain: a randomized, double-blind, placebo-controlled study. The Pharmacogenomics Journal. 2020; 20 (3). Available from: https://doi.org/10.1038/s41397-019-0131-z
34. OPRM1 A118G Polymorphism and Ondansetron Efficacy for Postoperative Nausea and Vomiting in Laparoscopic Gynaecological Surgery: A Retrospective Cohort Study. Therapeutics and Clinical Risk Management. 2025; 21 Available from: https://doi.org/10.2147/tcrm.s551616
35. Association of Genetic Variants with Postsurgical Pain: A Systematic Review and Meta-analyses. Anesthesiology. 2023; 139 (6). Available from: https://doi.org/10.1097/aln.0000000000004677
36. Review of Opioid Pharmacogenetics and Considerations for Pain Management. Pharmacotherapy: The Journal of Human Pharmacology and Drug Therapy. 2017; 37 (9). Available from: https://doi.org/10.1002/phar.1986
37. CYP2D6 phenotypes and opioid metabolism: the path to personalized analgesia. Expert Opinion on Drug Metabolism & Toxicology. 2022; 18 (4). Available from: https://doi.org/10.1080/17425255.2022.2085552
38. Opioid Monitoring in Clinical Settings: Strategies and Implications of Tailored Approaches for Therapy. International Journal of Molecular Sciences. 2024; 25 (11). Available from: https://doi.org/10.3390/ijms25115925
39. Pharmacogenomics in Pain Management: A Review of Relevant Gene-Drug Associations and Clinical Considerations. Annals of Pharmacotherapy. 2021; 55 (12). Available from: https://doi.org/10.1177/10600280211003875
40. Challenges with Implementing the Centers for Disease Control and Prevention Opioid Guideline: A Consensus Panel Report. Pain Medicine. 2019; 20 (4). Available from: https://doi.org/10.1093/pm/pny307
41. The Role of Clinical Pharmacogenetics and Opioid Interactions in Pain Management: Current Evidence and Future Perspectives. Pharmaceutics. 2026; 18 (1). Available from: https://doi.org/10.3390/pharmaceutics18010059
42. Pharmacogenomics of ABCB1 in opioid response. The Open Pain Journal. 2020; 13 (1). Available from: https://doi.org/10.2174/1876386302013010007
43. Opioid metabolism and clinical aspects. European Journal of Pharmacology. 2015; 769 Available from: https://doi.org/10.1016/j.ejphar.2015.10.049
44. Appraisal and development of evidence-based clinical decision support to enable perioperative pharmacogenomic application. The Pharmacogenomics Journal. 2021; 21 (6). Available from: https://doi.org/10.1038/s41397-021-00248-2
45. Effect of a Postoperative Multimodal Opioid-Sparing Protocol vs Standard Opioid Prescribing on Postoperative Opioid Consumption After Knee or Shoulder Arthroscopy. JAMA. 2022; 328 (13). Available from: https://doi.org/10.1001/jama.2022.16844
46. BCHE variants and prolonged neuromuscular blockade. Pharmacogenomics and Personalized Medicine. 2020; 13 Available from: https://doi.org/10.2147/pgpm.s263741
47. The Role of OMICS (Genomics, Epigenetics, Transcriptomics, Proteomics and Metabolomics) in Personalized Anesthesia and Perioperative Medicine. Personalized Medicine in Anesthesia, Pain and Perioperative Medicine. 2021; Available from: https://doi.org/10.1007/978-3-030-53525-4_2
48. Butyryl-cholinesterase deficiency: A case report of delayed recovery after general anaesthesia. Toxicology Reports. 2021; 8 Available from: https://doi.org/10.1016/j.toxrep.2021.06.016
49. Polymorphisms contribute to differences in the effect of rocuronium in Chinese patients. Basic & Clinical Pharmacology & Toxicology. 2022; 130 (1). Available from: https://doi.org/10.1111/bcpt.13682
50. Renew JR, Naguib M, Brull S. Clinical use of neuromuscular blocking agents. 2019.
51. Pseudocholinesterase deficiency and succinylcholine. Pharmacotherapy. 2025; 45 (9). Available from: https://doi.org/10.1002/phar.70048
52. Neuromuscular block management: evidence-based principles and practice. BJA Education. 2024; 24 (1). Available from: https://doi.org/10.1016/j.bjae.2023.10.005
53. Adeyinka A, Layer DA. Neuromuscular blocking agents. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024.
54. Recent Advances in the Clinical Value and Potential of Dexmedetomidine. Journal of Inflammation Research. 2021; 14 Available from: https://doi.org/10.2147/jir.s346089
55. Pharmacogenetic and pharmacokinetic factors for dexmedetomidine-associated hemodynamic instability in pediatric patients. Frontiers in Pharmacology. 2025; 15 Available from: https://doi.org/10.3389/fphar.2024.1515523
56. Genetic polymorphisms are associated with individual susceptibility to dexmedetomidine. Frontiers in Genetics. 2023; 14 Available from: https://doi.org/10.3389/fgene.2023.1187415
57. Pharmacogenomics in Anesthesia. Pharmacogenomics in Clinical Practice. 2023; Available from: https://doi.org/10.1007/978-3-031-45903-0_10
58. Regulation of cytochrome P450 gene expression by ketamine: a review. Expert Opinion on Drug Metabolism & Toxicology. 2018; 14 (7). Available from: https://doi.org/10.1080/17425255.2018.1487397
59. Genetic Variation and Sex-Based Differences: Current Considerations for Anesthetic Management. Current Issues in Molecular Biology. 2025; 47 (3). Available from: https://doi.org/10.3390/cimb47030202
60. Silva A, Mourão J, Vale N. Precision medicine and lidocaine pharmacokinetics. International Journal of Molecular Sciences. 2025;26(4):1506.
61. A critical approach to research on perioperative pain management. British Journal of Anaesthesia. 2025; 134 (3). Available from: https://doi.org/10.1016/j.bja.2024.11.004
62. Personalized Perioperative Opioid Strategies in Children: Focus on Methadone, Pharmacogenomics and Prevention of Persistent Postoperative Opioid Use. Children. 2025; 12 (12). Available from: https://doi.org/10.3390/children12121660
63. It Is in Our DNA: Bringing Electronic Health Records and Genomic Data Together for Precision Medicine. JMIR Bioinformatics and Biotechnology. 2024; 5 Available from: https://doi.org/10.2196/55632
64. Point-of-Care Diagnostics: Recent Developments in a Connected Age. Analytical Chemistry. 2017; 89 (1). Available from: https://doi.org/10.1021/acs.analchem.6b04630
65. Advancing Pharmacogenomics from Single-Gene to Preemptive Testing. Annual Review of Genomics and Human Genetics. 2022; 23 (1). Available from: https://doi.org/10.1146/annurev-genom-111621-102737
66. The Landscape of Medical Agents: A Survey. Authorea Preprints. 2025; Available from: https://doi.org/10.36227/techrxiv.176581395.56964766/v3
67. Medical Laboratories in Healthcare Delivery: A Systematic Review of Their Roles and Impact. Laboratories. 2025; 2 (1). Available from: https://doi.org/10.3390/laboratories2010008
68. Role of pharmacogenomics testing in enhanced recovery pathways. Pharmacogenomics and Personalized Medicine. 2019; 12 Available from: https://doi.org/10.2147/pgpm.s198224
69. Pharmacogenomics in practice: a review and implementation guide. Frontiers in Pharmacology. 2023; 14 Available from: https://doi.org/10.3389/fphar.2023.1189976
70. Genomics Testing and Personalized Medicine in the Preoperative Setting. Surgical Oncology Clinics of North America. 2020; 29 (1). Available from: https://doi.org/10.1016/j.soc.2019.08.006
71. A Web-Based Pharmacogenomics Search Tool for Precision Medicine in Perioperative Care. Journal of Personalized Medicine. 2020; 10 (3). Available from: https://doi.org/10.3390/jpm10030065
72. Personalized anesthesia and precision medicine: a comprehensive review of genetic factors, artificial intelligence, and patient-specific factors. Frontiers in Medicine. 2024; 11 Available from: https://doi.org/10.3389/fmed.2024.1365524
73. Accurate Machine Learning-based Monitoring of Anesthesia Depth with EEG Recording. Neuroscience Bulletin. 2025; 41 (3). Available from: https://doi.org/10.1007/s12264-024-01297-w
74. Artificial intelligence revolutionizing anesthesia management: advances and prospects in intelligent anesthesia technology. Frontiers in Medicine. 2025; 12 Available from: https://doi.org/10.3389/fmed.2025.1571725
75. Algorithm-Based Clinical Decision Support: Evolving Regulatory Landscape and Best Practices for Local Oversight. Annual Review of Biomedical Data Science. 2025; 8 (1). Available from: https://doi.org/10.1146/annurev-biodatasci-103123-094601
76. Perioperative Patients With Hemodynamic Instability: Consensus Recommendations of the Anesthesia Patient Safety Foundation. Anesthesia & Analgesia. 2024; 138 (4). Available from: https://doi.org/10.1213/ane.0000000000006789
77. Standardizing endpoints in perioperative research. Canadian Journal of Anesthesia/Journal canadien d'anesthésie. 2016; 63 (2). Available from: https://doi.org/10.1007/s12630-015-0565-y
78. Standardizing terms for clinical pharmacogenetic test results: consensus terms from the Clinical Pharmacogenetics Implementation Consortium (CPIC). Genetics in Medicine. 2017; 19 (2). Available from: https://doi.org/10.1038/gim.2016.87
79.
Genetic Testing for BCHE Variants Identifies Patients at Risk of Prolonged Neuromuscular Blockade in Response to Succinylcholine
. Pharmacogenomics and Personalized Medicine. 2020; 13 Available from: https://doi.org/10.2147/pgpm.s263741
80. Impact of the Cytochrome P450 2B6 (CYP2B6) Gene Polymorphism c.516G>T (rs3745274) on Propofol Dose Variability. European Journal of Drug Metabolism and Pharmacokinetics. 2016; 41 (5). Available from: https://doi.org/10.1007/s13318-015-0289-y
81. Personalized anesthesia and precision medicine: a comprehensive review of genetic factors, artificial intelligence, and patient-specific factors. Frontiers in Medicine. 2024; 11 Available from: https://doi.org/10.3389/fmed.2024.1365524
Subscribe now for latest articles and news.