Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.2021.v07i03.013
Year: 2021, Volume: 7, Issue: 3, Pages: 67-71
Original Article
Ravindra S Pukale1 , D Pragathi2
1Professor and Head, Department of Obstetrics and Gynaecology, Adichunchanagiri Institute of Medical Sciences, Adichunchanagiri University, Mandya, Karnataka, India,
2Postgraduate Student, Department of Obstetrics and Gynaecology, Adichunchanagiri Institute of Medical Sciences, Adichunchanagiri University, Mandya, Karnataka, India
Address for correspondence:
D Pragathi, Postgraduate Student, Department of Obstetrics and Gynaecology, Adichunchanagiri Institute of Medical Sciences, Adichunchanagiri University, Mandya, Karnataka, India. E-mail: [email protected]
Introduction : The novel CoronaVirus (SARS CoV 2) is a new strain of coronovirus causing COVID 19, first identified in Wuhan China it has become an unbating global health threat.1 The term Coronavirus derives from the Latin word corona, which means crown or halo.2 This SARS-CoV 2 has a high rate of transmission by respiratory droplets and through fomites. Most pregnant women present with mild symptoms and have a similar course of disease as non-pregnant adults. At present there is no such evidence that pregnant women are likely to become infected than any other adults. Aims and objectives : To determine the clinical course and fetomaternal outcome in pregnant women affected with COVID 19 infection. Materials and methods: This prospective study was done from March 2020 to May 2021 in Department of OBG at Adichunchanagiri Institute of Medical sciences, Bellur, Karnataka. After taking Institutional Ethics Committee clearance and informed written consent all cases of Pregnant women tested positive for SARS CoV 2 viruses are included in the study. Result: A total of 49 covid positive pregnant women were studied. Out of which 73.5% of the patients were asymptomatic, and among 13% of symptomatic patients, 12.2% of patients had fever, 7% had dry cough, and 2% had myalgia. There were 38 vaginal delivery (77.5%), 10 were Caesarean delivery (20.4%), and there was 1 still birth, 1 IUFD, 1 Maternal mortality, 1 incomplete abortion. Conclusion: The Covid 19 Pandemic had created dilemma in all areas of health including pregnant women due to limited knowledge. Covid-19 infection in pregnant women is same as that in general population. Our study concludes that majority of Covid-19 positive pregnant women had mild disease with good fetomaternal outcome.
Keywords: Pregnancy, COVID19, Fetomaternal outcome, Fetal distress, Vertical transmission
World Health Organisation (WHO) declared Corona virus disease (COVID-19) on March 11, a Public health emergency of International concern due to its outbreak in Wuhan China.
Corona viruses are enveloped RNA Viruses, which infects the host cells through Angiotensin converting enzyme 2 receptors present within Type 2 alveolar cells of lungs and aerodigestive tract. The first case in India was in Delhi on January 30, 2020. The COVID-19 infection has a high rate of transmission by Respiratory droplets and through fomites.
Due to the physiologic changes that occurs in Immune and Cardiopulmonary system makes the pregnant women more susceptible to infections. Certain studies are available regarding Covid-19 in pregnancy, but their results shows no significant evidence that pregnant women are more susceptible to corona virus infection. Also, a probable deferment in diagnosis and source control occurs in pregnant women, especially in women with only trivial upper respiratory tract symptoms like soreness and nasal congestion.[3] SARS-CoV-2 manifested the general symptoms of COVID-19, e.g., fever, cough, sore throat, myalgia diarrhea, malaise and shortness of breath.[4]
The first study describing the clinical characteristics and investigated the possibility of vertical transmission of SARS-CoV 2 in nine pregnant women with laboratory-confirmed COVID-19 infection demonstrated that the severity in pregnant women was similar to that in non-pregnant adults.[5]
SARS-CoV 2 was demonstrated in amniotic fluid, cord blood, and neonatal throat swab samples, there was evidence of vertical transmission. PCR-based methods are considered the gold standard for viral detection.[6] The decision regarding mode of delivery should consider the gestational age of the fetus and should be made by an obstetrician in collaboration with the neonatologist.[7]
To determine clinical course and fetomaternal outcome of Pregnant women infected with COVID 19.
This is a Prospective study of 49 cases of pregnant women with laboratory confirmed COVID19 infection from March-2020 to May 2021 in department of OBG at Adichunchanagiri Institute of Medical Sciences, B G Nagara, and Karnataka. After taking Institutional Ethics Committee clearance and informed written consent all cases of Pregnant women tested positive for SARS CoV 2 viruses are included in the study.
A Laboratory confirmed case of COVID-19 is defined as a positive result by Quantitative Reverse Transcriptase Polymerase Chain Reaction (qRT-PCR) assay of maternal pharyngeal and nasopharyngeal swab specimens.[8]
Safety measures like Personal Protective Equipment (PPE) including Jumpsuit, gloves, N-95 masks, face shield, googles were used in labour room and operation theaters by all health care professionals.
Chest CT scanning has high sensitivity for diagnosis of COVID -19. In Pregnant woman with suspected COVID-19 infection, a chest CT scan may be considered as a primary tool for the detection of COVID-19 in epidemic areas.[9]
Inclusion criteria: Laboratory confirmed positive case of COVID-19 infection in pregnant women
Exclusion criteria: Pregnant women with clinical signs and symptoms similar to SARS CoV-2, but the pharyngeal and nasopharyngeal swab were reported negative were excluded. Complete Obstetric history, clinical symptoms and signs, specific obstetric condition, obstetric examination, laboratory and radiologic investigations, treatment measures, complications and outcome data were collected.
Data on maternal and neonatal outcome including gestational age at delivery, mode of delivery, Indication for C-section, complications, neonatal birth weight and NICU admissions were analyzed.
Statistics is done using mean and proportions. To test the significance, Chi Square test is used. P value < 0.05 is considered statistically significant.
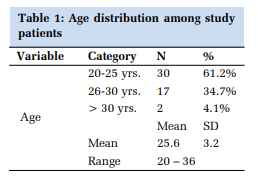
Among all the 49 patients, pregnant women reported mostly in third trimester and the mean maternal age was 25.6 yrs. as shown in Table 1.
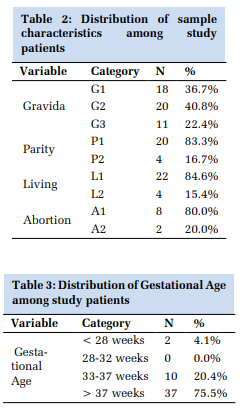
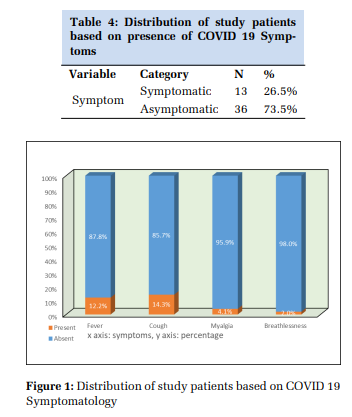
It was found that 36.7% women were primigravida, 20% were Gravida 2, and 11% were gravida 3 and 4 as shown in Table 2. Among 49 patients, on history taking it was found that 73.5% of the patients were asymptomatic, and among 26.5% of symptomatic patients as mentioned in Table 4,12.2% of patients had history of fever followed by dry cough in 14.3% of patients and myalgia in 4.1 % of patients at admission in hospital as mentioned in Figure 1.
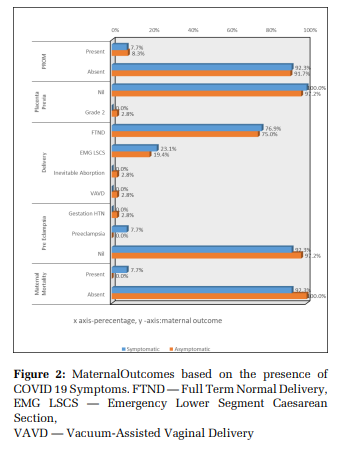
Among 49 patients, 4 patients presented with PROM, 2 patients had oligohydramnios, 2 patients had hypertension in pregnancy, one patient had Placenta Praevia, and one patient had intrauterine fetal demise, and one patient had still birth and one patient had incomplete abortion as shown in Figure 2 and Figure 3.
In this study of 49 cases, clinical characteristics of the women with covid-19 infection during pregnancy were similar to those of non-pregnant adults with Covid 19 infection. The gestational age at delivery varied from 29 weeks to 36 weeks with a mean of 33 weeks as mentioned in table 3, similar to a study done by Lina Antoun et al.[10] Pregnant women are particularly susceptible to respiratory pathogens and severe pneumonia because they are at an immunosuppressive state, and physiological adaptive changes during pregnancy can render them intolerant to hypoxia.[11] Other impairments of covid 19 infection are leucopenia, lymphocytopenia, mild thrombocytopenia, mild elevation of the liver enzymes and other acute infection markers. If an X-ray or CT scan is needed for a pregnant woman, abdominal shield must be used to protect the fetus from the radiation exposure. The most common symptoms were fever, cough, dyspnea, fatigue and myalgia. These results are similar to a study by J Juan et al.[12]The criteria for isolation of the covid 19 positive tested pregnant women and the general population are same. Co-infection with the other common respiratory pathogens often seen with the Covid 19 infection. Another study with obstetrics outcome of 108 women reported that majority of the women were delivered by caesarean section and there was one intrauterine and one neonatal death. There is no evidence that SARS-CoV can be vertically transmitted to the fetus. These results are similar to results of a recent study by Petra Zimmermann et al.[13] SARS Corona virus infection during pregnancy might cause Preterm birth, Intra uterine death, Intrauterine growth restriction as mentioned in figure 3.

The Covid 19 Pandemic had created dilemma in all areas of health including pregnant women due to limited knowledge. Covid-19 infection in pregnant women is same as that in general population. Our study concludes that majority of covid-19 positive pregnant women had mild disease with good fetomaternal outcome.
Study limitation: Sample size is small and Antenatal follow up of the COVID-19 positive pregnant women is incomplete because they have come for first visit to the hospital and after delivery they have not come for follow up.
Subscribe now for latest articles and news.