Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.2021.v07i03.018
Year: 2021, Volume: 7, Issue: 3, Pages: 109-111
Case Report
Diksha1 , Rashmi Sriram2 , Harshavardhan Gowda3 , Rajendra Okade4
1Postgraduate Student, Department of Dermatology, BGS Global Institute of Medical Sciences, Bangalore,
2Assistant Professor, Department of Dermatology BGS Global Institute of Medical Sciences, BGS Global Institute of Medical Sciences, Bangalore,
3Senior Resident, Department of Dermatology, BGS Global Institute of Medical Sciences, Bangalore,
4Professor and Head, Department of Dermatology, BGS Global Institute of Medical Sciences, Bangalore
Address for correspondence:
Rashmi Sriram, Assistant Professor, Department of Dermatology BGS Global Institute of Medical Sciences, BGS Global Institute of Medical Sciences, Bangalore. E-mail: [email protected]
Cheilitis Granulomatosa (CG) is a chronic progressive swelling of the lip due to granulomatous inflammation of unknown cause. When it is a part of a triad of recurrent lip edema, facial paralysis and scrotal tongue (lingua plicata) it’s called as Melkersson–Rosenthal syndrome (MRS). Seen mostly in young adults with a variable presentation; earliest cutaneous manifestation being a sudden diffuse or nodular swellings involving the lip (upper>lower). Labial swelling and facial swelling is also seen. Less commonly, the forehead, eyelids or one side of the scalp can also be involved.
Cheilitis Granulomatosa (CG) is a rare and unique disorder first described by Miescher in 1945.[1] It is clinically and histologically indistinguishable from orofacial granulomatosis introduced by Wiesenfeld, in which there may be orofacial lesions in addition to labial swelling.[2,3] Itis an incomplete variant of Melkersson-Rosenthal syndrome (MRS) where there is a triad of recurrent lip edema, facial paralysis and scrotal tongue (lingua plicata). In Miescher cheilitis, the granulomatous changes are confined to the lip, and hence is regarded as a monosymptomatic form of Melkersson–Rosenthal syndrome. We present a case of CG in a Forty-year- old female patient who came to the Dermatology OPD with the complaints of swelling of the lips from the past two months.
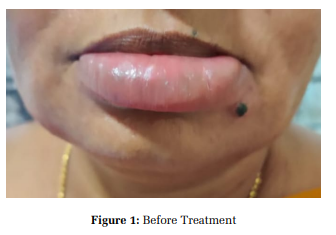
A Forty-year-old female presented with a persistent and painful swelling of lower lip since past two months (Figure 1). It was associated with dryness of the lips since two months and itching of the lower lips since one month. There was a history of consumption of an ayurvedic medication (Rye grass) for 4 months before the onset of lesion. On examination the patient had a diffused erythematous swelling over the lower lip not associated with scaling and ulcerations. Neither facial nerve palsy nor fissuring of the tongue was present.
No lesions were seen intraorally. Chest x-ray and Mantoux test was normal, food allergy test (normal range - <0.1 Ku/L) was positive for the following food products
Chicken Meat: 0.4, Shrimp/Prawns:0.1, Wheat:0.1,Milk:0.1, Baker Yeast-1.10, Tomato0.1,Corn/Maize-0.1, Carrot-0.1, Banana-0.3,Rice-0.1, Rye Grass-0.5, Oat-0.1, IgE Total Antibody-436 IU/mL (normal range 0-378 IU/mL).
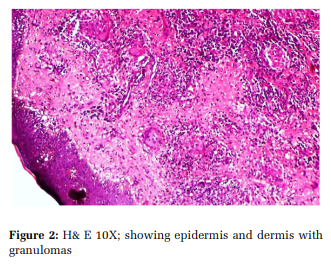
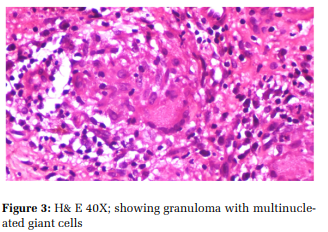
Lip biopsy revealed epidermis with mild spongiosis, acanthosis and basal mixed inflammation, composed of small well-formed non caseating epithelioid granuloma, foreign body and langhans type giant cells, lymphocytes and plasma cells. Pigment incontinence noted (Figure 2 and Figure 3)
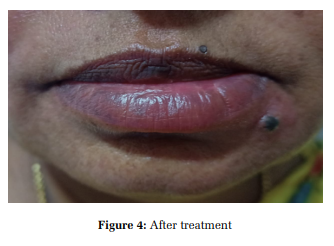
Patient was advised to avoid above mentioned food allergens and was treated with 65mg minocycline for 2 months and intralesional Triamcinolone Acetonide 10 mg/ml weekly once for 4 weeks following which there was complete resolution. (Figure 4)
CG is a chronic progressive swelling of the lip due to granulomatous inflammation of unknown cause. It has various presentation when seen as a triad of recurrent orofacial swelling, relapsing facial paralysis and fissuring of the tongue (lingua plicata) it is termed as MRS. The presence of CG without lingua plicata or facial palsies it is termed as Miescher syndrome or Miescher’s Cheilitis. [1] Wiesenfield introduced the concept of Orofacial granulomatosis (OFG).[2,3]Today both CG and MRS are considered subsets of OFG. Certain reports suggest some cases may demonstrate an autosomal dominant inheritance pattern.[4] Other authors have proposed a wide range of causes including allergic reactions like –cobalt,[5] food additives such as cinnamic aldehyde.[6,7] Dietary antigens such as Butylated hydroxyanisole, Dodecyl gallate, Menthol, Monosodium glutamate, Contact antigens (e.g. gold, mercury). It is also seen as autoimmune mechanism, as an association with sarcoidosis[8] and Crohn’s disease[9] and even as a oral manifestation of systemic diseases. In our case the patient had a swelling of lower lip associated with pain and itching; there was a history of usage of ayurvedic medicine (Rye grass). Lip biopsy revealed mild spongiosis, acanthosis, small wellformed non caseating epithelioid granuloma, foreign body and langhans type giant cells, lymphocytes and plasma cells and these findings were consistent with diagnosis of CG. It should be differentiated from other causes of swelling of lip like that induced because of trauma, infection, systemic disease like Crohn’s disease, sarcoidosis and angioedema. Topical and intralesional steroid injections are the mainstay of treatment. The dose depends on the severity of swelling and usually patients are treated every week for 2–3 weeks. Systemic therapy in recalcitrant or severe disease includes the use of prednisone (1 mg/kg), thalidomide, minocycline, and more recently, monoclonal antibodies against TNF-α.
CG is a rare entity and treatment is difficult. The present case report reveals the importance of food allergy test and the role of food allergen in the etiopathogenesis of the disease.
Subscribe now for latest articles and news.