Journal of Medical Sciences and Health
Year: 2022, Volume: 8, Issue: 1, Pages: 28-34
Original Article
Steve Paul Manjaly1, Savitha A Sebastian2, Arun Alex3
1Consultant Geriatrician, Apollo Hospitals, Bannerghatta Road, Bangalore, 560078, Karnataka, India,
2Assistant Professor, Department of General Medicine, St. John’s Medical College, Bangalore, 560034, Karnataka, India,
3Consultant Gastroenterologist, St Gregorius Hospital, Parumala, Thiruvalla, 689626, Kerala, India
Address for correspondence: Steve Paul Manjaly, Consultant Geriatrician, Apollo Hospitals, Bannerghatta Road, Bangalore, 560078, Karnataka, India. E-mail: [email protected]
Malnutrition in the elderly has been associated with deleterious effects on health care outcomes such as functional decline, cognitive impairment, depression, increased hospital stays, and increased morbidity and mortality. This cross-sectional study aims to determine the association of malnutrition with functional status and cognition and duration of hospitalization among 200 elderly patients admitted to medical wards of a tertiary care hospital in India. The nutritional screening was done using Mini Nutritional assessment- short form (MNA-SF). The functional activity was assessed using the Barthel’s Index. Cognitive assessment and screening for depression was done using the Mini-cog test and Geriatric Depression score – 4 respectively. Descriptive analyses were used to estimate the prevalence of malnutrition and associations were assessed using the Pearson chi square test. Among the total patients, 136 (68%) were malnourished. Of these, 45 (22.5%) were severely undernourished. The malnourished patients had poorer functional scores (p<0.001), were likely to be cognitively impaired (33%, 45 of 136) (p < 0.001) and stayed longer in the hospital (n= 9.13 days) compared to the normally nourished. The nutritional status of hospitalized elderly may therefore serve as a surrogate marker of disability and poor clinical outcome.
Keywords: Malnutrition, Geriatric, Nutritional assessment, Undernourishment, Functional decline, Elderly
Older adults are at risk of malnutrition. It has been reported that 15% of community-dwelling and homebound elderly individuals, 62% of hospitalized elderly patients, and 85% residents of nursing homes are malnourished.[1–4]
The causes of malnutrition in the elderly are multi-factorial. Apart from physiological changes such as decreased appetite, hospitalization and acute illnesses, psychosocial causes like isolation, depression, cognitive impairment, loneliness and insecurity, and economic factors such as poor purchasing power, medication costs also contribute.[5,6] Moreover, elderly people living alone may be reluctant to prepare food for themselves and may not take a balanced diet.
These subsequently lead to progressive decline in health, reduced physical and cognitive functional status, complicated hospitalization outcomes, morbidity and mortality.[7–9]
Nutritional status is closely linked to functional activity of older hospitalized patients.[10] Functional status is a key indicator of geriatric health and any decline in the functional activity of older hospitalized patients could have widespread ramifications on their health outcomes.[11] Therefore, the need of a thorough nutritional assessment and appropriate interventions to prevent functional decline needs to be emphasized. Hospitalized older patients are at particular risk of malnourishment as their acute illness demands an increased nutritional requirement. This leads to a myriad of biochemical abnormalities such as hypoalbuminemia, hypokalemia and sarcopenia that can result in prolonged hospitalization leading to a bed bound state.[12] This points out the dearth of nutritional assessment and intervention in hospitalized elderly patients.
Though there is no gold standard for estimating malnutrition among the elderly, assessment tools that are sensitive to predict malnutrition in the elderly are available. Mini Nutrition Assessment (MNA) is a simple, low cost and non-invasive tool designed for health professionals, which can be done at the bedside to monitor the health status of patients both in hospital and in nursing homes.[13–16] It has a sensitivity of 96%[17] specificity of 98%, and the prognostic value for malnutrition of 97%.[13] The MNA scale comprises 18 items, corresponding to 4 domains: anthropometric measurements, dietary behavior, global (risks factor for malnutrition) and subjective assessment of self-perceived quality of health and nutrition.
MNA has also been proved valuable for screening in a short form version, Mini Nutritional Assessment short-form (MNA-SF).[13,18–20] MNA – SF has a total score of 14; scores 8-11 are at risk for malnourishment and scores < 8 undernourished. In the present study, we aimed to assess the association between the nutritional status and adverse clinical outcomes such as functional decline, cognitive impairment, prolonged or complicated hospital stay (including Intensive Care) or mortality, in elderly in-patients in a teaching hospital in south India.
The setting for this study was at the Division of Geriatric Medicine, at a teaching hospital in Bangalore, South India. The study populations were included from both the general and the geriatric wards. Two hundred patients who were 60 years or older and admitted in the medical wards between October 2014 to March 2015 were included in the study, after obtaining their consent. The patients selected were grouped into youngold (60-74yrs), old-old (75-84yrs) and the oldest old (>85yrs). Those who had terminal illnesses such as malignancy, advanced dementia, advanced Parkinsonism or Human Immunodeficiency Viruses (HIV) were excluded. Those unable to provide answers to the screening questionnaires due to lack of a caregiver or due to severe cognitive impairment were excluded from the study. The study protocol had been approved by the Institutional ethical committee and review board (No. 144/2014).
Demographic data were recorded which included age, sex, living condition, (living alone/ with spouse/ with children) and residential status.
The nutritional screening was done using MNA-SF. The MNA-SF consists of six questions which include dietary questionnaire, food intake, acute illness, neuropsychological problems and anthropometric measurements.[15,21] The maximum subtotal of the score is 14. A total score of MNA-SF <8, 8–11, and >11 indicates malnutrition, risk of malnutrition, and no malnutrition, respectively. In the present study, patients were grouped into three categories.
a. Normally nourished: MNA-SF score >11
b. At risk of malnourishment: MNA-SF score 8-11
c. Severely malnourished: MNA-SF score< 8
Category b and c was broadly grouped as malnourished.
Height was measured using a stadiometer, and weight, using a digital weighing scale. In patients who were unable to stand, nutritional assessment required the measurement of the calf circumference using a measuring tape as per the MNA- SF.[20] The functional activity was assessed using the Barthel Index for Activities of Daily Living (ADL).[22]
It is a well-established tool comprising of bowels and bladder function, self-care (grooming, dressing, toileting and bathing), feeding and global function (transfers and mobility). Each domain is score in one-point increments ranging from 0-20. Cognitive assessment was done using the Mini-cog test.[23]
It is a short survey to screen for cognitive impairment in older adults, consisting of a threeword recall and a clock drawing test. Patients were given three unrelated words to memorize and asked to recall. Patients were then asked to draw the face of a clock and the hands of the clock to read a specific time. A point is given for each word recall and 2 points for normal clock draw. If the patient scores <3, they are diagnosed as positive for “cognitive impairment”.
Geriatric Depression score – 4 (GDS-4) was used to screen for depression. It consists of four structured questions to detect major depression.[24] Scores less than one- no depression and scores more than onelikely to be depressed. The duration of hospital stay was taken as prolonged if the total duration exceeded 7 days.
Data was assessed using the IBM SPSS v 20. Descriptive analyses were used to estimate the patient characteristics, duration and outcome of hospitalization, prevalence of malnutrition, functional and cognitive status. Numerical variables were expressed as mean ± standard deviation and category variable were expressed in frequency and percentage.
The association of malnourishment with functional and cognitive status and duration of hospitalization was assessed using the Pearson’s chi square test. Normality was assessed using several assumptions of Normal distribution. ADL and duration of hospital stay were not normally distributed. Comparison of functional and cognitive status and hospitalization with nutritional status was calculated using Kruskal walli’s test. Since a significant difference in ADL was noted, Dunn- Bonferroni multiple comparison tests were done.
Two hundred inpatients were assessed. Out of these, 125 (62%) were aged 60-74 years (young old), 65 (33%) were in the age group of 75-84 years (old old), and 10 (5%) were aged above 85 years (oldest old). The mean age of the patients in the study group was 71 years.
Of the 200 patients, 84 (42%) were females and 116 (58%) were males. Seventy six percent of the patients lived with their children, 19% with their spouses, 3% lived alone and 2 % were institutionalized.
The mean duration of hospital stay were 8.48 days with 107 (53%) patients having a prolonged duration of hospital stay.
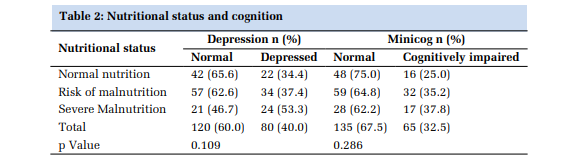
Of the 200 patients, 28 of them required treatment in the intensive care unit during their course of hospital stay. Eighty patients (40%) were depressed, and 65 (32.5%) cognitively impaired.
One hundred and four patients could not have their weights recorded. These patients were too ill to stand up or had diseases that precluded maintaining an erect posture. The average weights of the patients recorded were 56 kg. The lowest weight recorded was 28 kg.
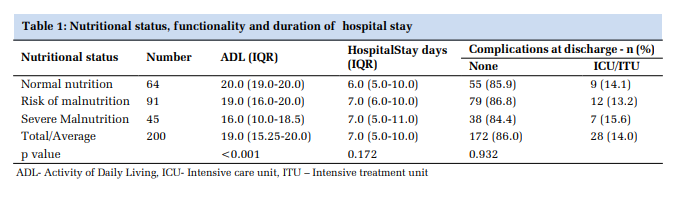
Only sixty-four (32%) of the 200 patients were normally nourished. Forty-five were severely malnourished.
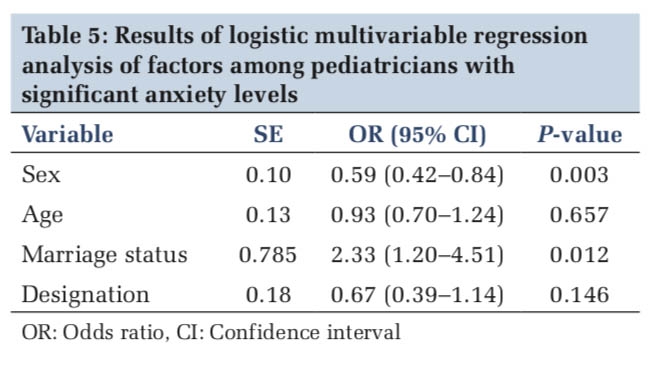
Out of the 200 patients screened, a statistically significant 80% (67 of 84) of the malnourished were women as compared to 59% (69 of 116) of malnourished men (p <0.01).
Significant association was noted between the mean ADL scores and the degree of nutrition, with a higher mean ADL score noted in those with normal nutritional status (p<0.001). In pairwise comparison, each of the subgroups of MNA showed a statistically significant association with decline in ADLs.
Undernourished patients stayed longer in the hospital compared to those with normal nourishment. Although, the duration of the hospital stay appeared to increase proportionally to worsening nutritional status, this was not statistically significant.
Twenty-eight patients had a complicated event during hospitalization necessitating ICU admission. Of these 7 belonged to the severely malnourished group.
Eighty patients were depressed according to the Geriatric Depression Scale (GDS-4) score. Of these, majority (37.4%, n=34) belonged to the ‘at risk’ group, followed by the severely malnourished group (53.3%, n= 24).
Of the 200 patients, sixty-five (32.5%) were cognitively impaired, majority in the ‘at risk’ group (n=32, 35.2%). Cognitive impairment was also significantly higher in malnourished patients (73.0%, 49 of 136) (p<0.001).
Risk of malnutrition increases with age and the present study aimed to assess the association of malnutrition among elderly with functional and cognitive decline, depression, length of, and / or complicated hospital stay. Our study revealed the malnourished patients tended to have cognitive impairment, poor functional status and prolonged hospital stay.
Previous studies have estimated the prevalence of malnourishment to be 69.6% in elderly inpatients.[5] We observed a similar prevalence of malnourishment among our hospitalized elderly, with higher rates in elderly women compared to men, in direct contrast to other studies conducted in South India. The proportion of patients ‘at risk for malnourishment’, and of those with ‘overt malnourishment’, were also similar to studies conducted among community living elderly in other parts of the world.[25–28]
Our study showed that malnourished patients had a worse functional status compared to those normally nourished. Malnutrition leads to the biological plausibility that poor nutrition results in poor muscle strength and balance. This can result in gait abnormalities and increased dependence on caregivers. Malnutrition has previously been shown to be a predictor of poor functional status in various settings including hospitalized patients.[10] Poor muscle strength, decreased bone mass and altered cytokine production are contributors to poor functional status.[29] Conversely, functional status impairment increases vulnerability and can have negative impacts on quantity and quality of food consumption.[10] This in turn, can have deleterious effects on the hospitalized patient and can predispose to falls; fear of fall, gradually leading to a bed bound state.[10] Studies conducted in Brazil and Japan have earlier shown that malnourished older people were more dependent on eating and had poor health outcomes compared to normally nourished individuals.[11,30]
Depression was a harbinger of under nourishment. Loneliness, poor social support are often causes of poor eating habits, poor calorie intake and can lead to undernutrition.[5] Conversely, prolonged hospitalization and other disease states also could lead to depression. Though various studies have emphasized the need to rule out depression as a cause of undernourishment in elderly, this is mostly left unaddressed.[31,32]
Patients with cognitive impairment are more likely to be malnourished.[33] Cognitive impairment may interfere with the ability to appreciate taste and smell sensations, texture of the food, affecting a nutritious meal intake. It is also often associated with motor disability or difficulties in chewing and swallowing that precludes patients from consuming a healthy meal. [34] Our study showed a statistically significant association between cognitive decline and malnourishment, similar to studies done outside India.[33,35]
Our study revealed that malnourishment was associated with longer hospital stay and as in other studies, these patients were prone to developing worse clinical outcomes.[36,37] A previous study in India showed an increased length of hospital stay of eight days among elderly malnourished patients.[38] Our study showed a similar finding with elderly ‘at risk of malnutrition’ and ‘severe malnutrition’ staying eight and nine days respectively. Though this was not statistically significant, it highlights the need for nutrition screening and intensive treatment in this subgroup. The absence of any statistically significant association in our study could be explained from various non-medical factors that may have influenced hospital stay in an urban population at a tertiary hospital, such as this. Our study emphasized the effects of malnutrition among hospitalized elderly patients. Nutritional assessment needs to be recognized as a vital sign in the assessment of older patients on admission as this would help in predicting poor hospital outcomes and cognitive functional decline.
Our study has its limitations. Firstly, the sample selected was relatively small and comprised patients admitted from medical wards. Secondly, nutritional assessment was done using a standardized questionnaire, and not a by a rigorous assessment including the diet composition details, the amount of calorie consumed or by examination of laboratory and biochemical parameters. A comprehensive evaluation would have probably yielded more information.
Nutritional assessment is often overlooked in the management of hospitalized elderly. Hospital policies should incorporate simple nutritional assessment tools in the routine evaluation of older patients in the medical wards. This can serve as an index of adverse hospital outcomes.
We extend our sincere gratitude to Mrs Mridula Vellore, Research Assistant of Jubilee Center Medical Research for editing this article, and Mr. Unnikrishnan, Lecturer, Department of Community Medicine for data analysis.
Subscribe now for latest articles and news.