Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.v9i3.23.124
Year: 2023, Volume: 9, Issue: 3, Pages: 336-339
Case Report
Jawalkar Aishwarya1 , Nagarjuna Chary Rajarikam2
1Post Graduate Resident, Department of Pathology, Nizamabad,
2Professor and Head of the Department, Department of Pathology, Government Medical College, Nizamabad
Address for correspondence:
Jawalkar Aishwarya, Post Graduate Resident, Department of Pathology, Nizamabad.
E-mail: [email protected]
Received Date:17 May 2023, Accepted Date:13 October 2023, Published Date:28 December 2023
Gouty arthritis is an inflammatory condition due to defective uric acid metabolism resulting in deposition of monosodium urate crystals deposited within and around joints. Rheumatoid arthritis (RA) is an autoimmune inflammatory condition mostly involving peripheral joints. In this report, we describe the clinico-pathological features of a polyarticular tophaceous gout in a 68-year-old male with polyarticular arthritis, affecting all the joints of upper limbs and lower limbs associated with subcutaneous nodules and to emphasize the importance of differentiating this disease entity from RA so that early treatment can be started to prevent joint deformity and loss of function.
Keywords: Arthritis, Gout, Polyarticular, Tophi
Gout is a most prevalent form of chronic inflammatory arthritis characterized by urate crystals deposition in the joints or soft tissues, following long standing hyperuricemia. Gout occurs more often in middle aged and elderly men. It presents later in women after menopause and is associated with comorbidities such as hypertension, renal insufficiency, more often use of diuretics.
Gout usually manifests as acute monoarticular arthritis, often affecting the big toe. Polyarticular involvement is less frequent and tends to be linked with more advanced and longstanding gout cases.
Gouty tophi represent a foreign body granulomatous reaction comprising of collections of urate crystals with surrounding inflammatory cells and connective tissue 1, 2.
Tophus is mainly responsible for the functional limitation of joint, chronic pain, joint damage and significant joint deformities.
A 68-year-old male was presented to department of General Surgery at Government General Hospital, Nizamabad, a tertiary care hospital, with long standing history of frequent intermittent episodes of arthritis for approximately 25 years initially involving small joints of feet and ankles and gradually involving small and large joints of both upper limbs and lower limbs. The patient reported with the history of pain and swelling on elbows and small joints of hands and feet for 2 years. Patient developed recurrent attacks of pain after intake of alcohol and non-vegetarian diet. He intermittently used analgesics for pain relief. He is a known case of hypertension for 30 years and on Tab Met-XL 50mg regularly. He is a known case of Coronary artery disease (CAD) for 8 years. He has been on a mixed diet and a chronic alcoholic for 40 years. No similar history in the family.
Physical examination of locomotor system revealed multiple subcutaneous nodules on second metacarpophalangeal joint (MCP), third proximal interphalangeal joint (PIP) joint of Right hand, both elbows, third & fifth PIP joint of left hand and first Figure 1 ), right midfoot and Right tibialis anterior.



Laboratory workup revealed hemoglobin 12.9 g/dL, Total Leukocyte counts of 12,800/µL, platelet counts of 183x103/ µL, erythrocyte sedimentation rate (ESR) of 75/mm I st hour, serum uric acid of 9.5 mg /dL, serum creatinine of 0.9 mg/dL, rheumatoid factor (RF) negative, fasting blood glucose of 110 mg/dL, Glycated hemoglobin HbA1c of 6.5%.
X-ray both hands with wrists shows Left 5th PIP joint rat bite erosions & Left 4th PIP soft tissue shadows noted. X-ray Both feet show Bilateral 1st MTP joint erosions.
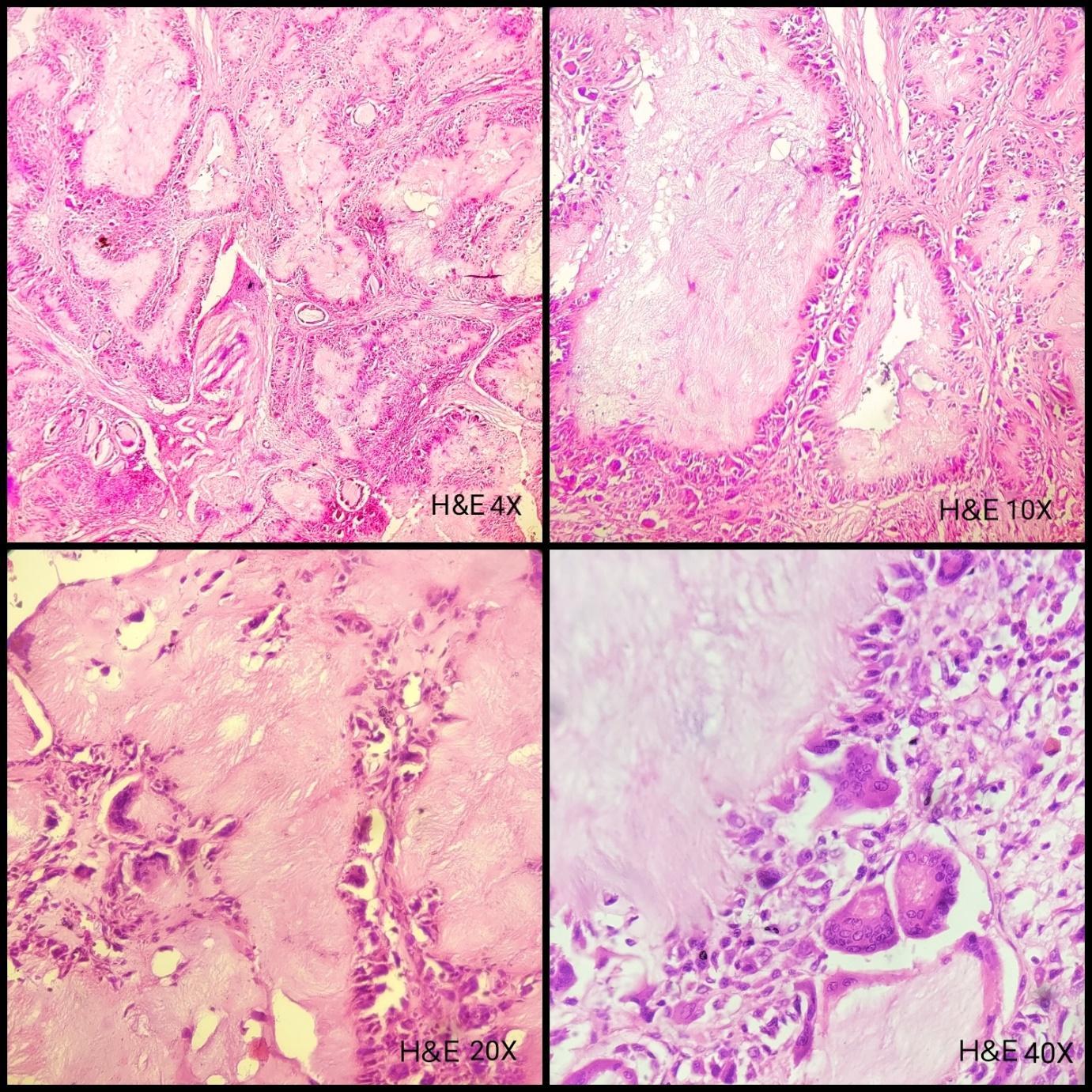
Histopathological examination of nodule removed from left MCP joint (Figure 2, Figure 3) revealed multiple irregular pale amorphous dissolved urate crystal areas rimmed by granulomatous inflammation comprising of histiocytes, multinucleated giant cells and lymphocytes, suggestive of Tophi (Figure 4). A diagnosis of tophaceous gout was made and the patient was treated with colchicine 0.5 mg/day and febuxostat 40 mg/day, naproxen 500mg for symptomatic relief. Patient was advised complete restriction of alcohol and red meat intake and a low sodium diet. Follow-up of the patient revealed serum uric acid levels of 6.1 mg /dL and his symptoms subsided.
The prevalence of gout is increasing across the world and is higher in males and increases with age for both males and females. In India, approximately 0.3% of the population is affected by gout. It usually affects the first MTP joint. Gout in elderly patients shows frequent polyarticular presentation and also involves joints of upper limbs. Gout is rarely seen in women in the premenopausal age group as the estrogen promotes renal clearance of uric acid 3.
Gout is a metabolic disorder characterized by hyperuricemia (serum uric acid> 6.8 mg/dL) which results from decreased renal uric acid excretion, drug induced hyperuricemia (Thiazide diuretics, Pyrazinamide) , dietary factors such as consumption of red meat, alcohol and seafood 4.
Gout is associated with increased frequency of obesity, chronic kidney disease, hypertension, type 2 diabetes mellitus, dyslipidemias, cardiac diseases, stroke and peripheral arterial disease (PVD) 5.
In untreated cases, gout may lead to chronic tophaceous gout and it usually occurs in patients who had gouty arthritis for at least 10 years. Tophi represents subcutaneous, nodular collection of monosodium urate crystals at joints and in soft tissues overlying tendons or cartilage 6, 7, 8.
Gout typically presents as acute monoarticular (affecting one joint) arthritis, most commonly in the big toe. Polyarticular involvement is less common and is often associated with more advanced and long-standing cases of gout. Polyarticular tophaceous gout is a chronic and progressive condition. It may result in severe joint damage, deformities, and significant disability if not managed effectively.
In RA, presence of subcutaneous nodules is a common and significant finding and seen in approximately 30% of patients with RA. These patients are usually tested positive for rheumatoid factor (RF). Although the disease processes for gout and RA are different, both are characterized by pain and swelling in joints which may lead to disability. Thus, gout can be considered in patients with subcutaneous nodules with negative RF and should be investigated.
Early diagnosis and intervention play a pivotal role in preventing joint deformities. Timely identification and treatment of joint conditions can significantly reduce the risk of permanent structural abnormalities. Prompt intervention helps to manage inflammation, control disease progression, and preserve joint function.
Polyarticular tophaceous gout presents unique challenges in the context of a differential diagnosis with several important implications to consider:
Mimicking Other Conditions: Polyarticular tophaceous gout can mimic the symptoms of other rheumatic or inflammatory diseases such as rheumatoid arthritis, osteoarthritis, or pseudogout. This similarity in symptoms makes it crucial for healthcare providers to conduct thorough evaluations and consider gout in the differential diagnosis, especially in cases with joint involvement.
Risk of Misdiagnosis: Due to its rarity and the potential overlap of symptoms with other joint disorders, polyarticular tophaceous gout is at risk of being misdiagnosed. This can lead to delayed treatment and further complications.
Need for Crystal Identification: Definitive diagnosis often requires the identification of uric acid crystals in joint fluid or tophi. This diagnostic step can be crucial in distinguishing gout from other joint conditions and should be pursued when polyarticular tophaceous gout is suspected.
Multifaceted Approach: The diagnosis of polyarticular tophaceous gout often involves a combination of clinical evaluation, imaging studies, laboratory tests (including serum uric acid levels), and joint fluid analysis. The need for a comprehensive approach underscores the importance of considering gout in the differential diagnosis of joint diseases.
Treatment Implications: Accurate diagnosis is essential because the treatment approach for polyarticular tophaceous gout differs significantly from that of other joint disorders.
Medical management aims at pain relief and to prevent further acute attacks. First line options are nonsteroidal anti-inflammatory drugs (NSAIDS), colchicine and glucocorticoids. Uric acid lowering drugs are used to treat chronic gout 9.
Surgical treatment is rarely required and it is indicated in cases of infected tophi with ulceration, joint deformities or in tophi causing nerve compression 10.
Most commonly involved joint in Gout is the Metatarsophalangeal joint. While polyarticular tophaceous gout is relatively rare compared to other forms of gout, it is a serious manifestation of the disease that typically occurs in individuals with long-standing and poorly managed gout. Polyarticular arthritis is seen in many conditions like RA, septic arthritis, Osteoarthritis, Systemic lupus erythematosus. Polyarthritis along with subcutaneous nodules is also seen in RA. However, Polyarticular tophaceous gout should be considered as one of the differential diagnosis in such cases for early management and for prevention of joint deformities. Treating polyarticular tophaceous gout can be more challenging than managing acute gout attacks. It often requires a combination of medications, including urate-lowering drugs and anti-inflammatory agents, along with lifestyle modifications.
Subscribe now for latest articles and news.