Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.2021.v07i02.006
Year: 2021, Volume: 7, Issue: 2, Pages: 34-38
Original Article
Saba Ekta1 , Bhatnagar Shrish2 , Shamsi Sumaiya3 , Mohd Shahid4
1 Senior Resident, Department of Pediatrics, Hamdard Institute of Medical Sciences and Research Centre, Gaya, Bihar, India
2 Professor and Head, Department of Pediatrics, Eras Lucknow Medical College and Hospital, Lucknow, Uttar Pradesh, India
3 Assistant Professor, Department of Pediatrics, Eras Lucknow Medical College and Hospital, Lucknow, Uttar Pradesh, India
4 Senior Resident, Department of Pediatrics, Eras Lucknow Medical College and Hospital, Lucknow, Uttar Pradesh, India
Address for correspondence: Dr. Shrish Bhatnagar, Professor and Head, Department of Pediatrics, Eras Lucknow Medical College and Hospital, Lucknow, Uttar Pradesh - 226 017, India. Ph: 9918208555. E-mail: [email protected]
Introduction: Rome 4 criteria have classified pediatric functional abdominal pain (FAP) disorders into four variants, that is, functional dyspepsia (FD), FAP not otherwise specified (FAP-NOS), irritable bowel syndrome (IBS), and abdominal migraine (AM). However, there is lack of information on Endoscopy and Histo-pathological findings in this subset of children.
Objective: The objective of the study was to evaluate the endoscopic and histopathological findings in children with FAP disorders especially FD and FAP NOS.
Materials and Methods: This was a prospective observational study. 110 children (aged 4–17 years) with diagnosis of FAP according to Rome 4 criteria were enrolled from pediatric outpatient department, after written consent underwent gastrointestinal endoscopy and biopsy
Results: Majority of children were girls (n = 62, 56.4%). Most of them belonged to age group of 6–12 years (52.7%). Fifty-eight (52.7%) children were suffering from FD, 42 (38.2%) children suffering from FAP NOS, nine (8.2%) had IBS, and one child had AM. Endoscopic assessment showed 28 (42.3%) children with FD had either gastritis, duodenitis, or esophagitis while it was seen only in two (4.8%) children with FAP NOS (P < 0.001) and none in IBS or AM. Rapid Urease Test for Helicobacter pylori was positive in 30 (51.7%) of children with FD, while only 1 in FAP NOS (P < 0.001). Histopathological assessment collaborated with endoscopic assessment in both the categories. Thirty-five children of FD had evidence of gastritis, duodenitis, esophagitis, or mixed while only four children of FAP NOS and one child of IBS had abnormal histology (P < 0.001). On follow-up 96.6% children with FD improved when given treatment with PPI and H. pylori (in positive cases).
Conclusion: : Children with FD have significant high incidence of organic causes including H. pylori infection. Hence, we recommend that children with FD should be subjected to both upper Gastrointestinal endoscopy and H. pylori evaluation while FAP-NOS usually do not require the same.
KEY WORDS: : Functional abdominal pain, functional dyspepsia, Helicobacter pylori
Abdominal pain is a common recurrent pain complaint of childhood. Approximately 15% of schoolchildren experience weekly episodes of abdominal pain and 8% consult a doctor.[1] Rome 4 criteria have classified pediatric functional abdominal pain (FAP) disorders into four variants, that is, functional dyspepsia (FD), FAP not otherwise specified (FAP-NOS), irritable bowel syndrome (IBS), and abdominal migraine (AM).[2] Recent evidence has shown that FD, one of the four main diagnostic entities of FAP, can show some organic changes on endoscopic evaluation.[3] Moreover, Helicobacter pylori, one of the most common etiological factors behind FD remains undetected using conservative diagnostic methods.[4] Recently, Rome IV guidelines have also recommended assessment of role of gastrointestinal (GI) endoscopy in FAP, especially FD.[2] However, there is lack of information on endoscopy and histopathological findings in this subset of Indian children and thus this study was planned to evaluate the endoscopic and histopathological findings in children with FAP.
It was prospective cross-sectional study. The target sample size was calculated on the basis of positive diagnosis by biopsy among all positive cases diagnosed by gastrointestinal endoscopy which was 63.8%.[5] 110 children (aged 4–17 years) with diagnosis of FAP according to Rome 4 criteria were enrolled from pediatric gastroenterology outpatient department of tertiary care teaching hospital. Diagnostic criteria for FD are (Must include one or more of the following bothersome symptoms at least 4 days/month): 1. Postprandial fullness 2. Early satiation 3. Epigastric pain or burning not associated with defecation 4. After appropriate evaluation, the symptoms cannot be fully explained by another medical condition.
Diagnostic criteria for IBS (Must include all of the following): 1. Abdominal pain at least 4 days/month associated with one or more of the following: (a) Related to defecation, (b) a change in frequency of stool, and (c) A change in form (appearance) of stool 2. In children with constipation, the pain does not resolve with resolution of the constipation (children in whom the pain resolves have functional constipation, not IBS) 3. After appropriate evaluation, the symptoms cannot be fully explained by another medical condition.
Diagnostic criteria for AM (Must include all of the following occurring at least twice): (1) Paroxysmal episodes of intense, acute periumbilical, midline or diffuse abdominal pain lasting 1 h or more (should be the most severe and distressing symptom). (2) Episodes are separated by weeks to months. (3) The pain is incapacitating and interferes with normal activities. (4) Stereotypical pattern and symptoms in the individual patient. (5) The pain is associated with two or more of the following: (a) Anorexia, (b) Nausea, (c) Vomiting, (d) Headache, (e) Photophobia, (f) and Pallor. (6) After appropriate evaluation, the symptoms cannot be fully explained by another medical condition.
Diagnostic criteria for FAP NOS must be fulfilled at least 4 times/month and include all of the following: (1) Episodic or continuous abdominal pain that does not occur solely during physiologic events (e.g., eating and menses). (2) Insufficient criteria for IBS, FD, or AM. (3) After appropriate evaluation, the abdominal pain cannot be fully explained by another medical condition.
A detailed relevant history, clinical features along with thorough clinical examination were performed on the pro forma designed for the study.
All children after written consent from parents and assent underwent upper gastrointestinal endoscopy and biopsy (esophagus, stomach [Rapid Urease Test (RUT) for H. pylori] and Duodenum). The presence of Erythema, Erosions, Ulcerations, Mucosal breaks, and Nodularity was considered as significant findings on endoscopy.
GI Endoscopy was performed using Olympus GIF 150 series endoscope in all the children with functional pain disorder. At least two biopsies, 1–2 mm in size were obtained from the esophagus, stomach (Antrum) along with RUT for H. pylori done) and the second part of the duodenum. Biopsy was sent for histopathological evaluation. Children having predominant large bowel symptoms were also subjected to colonoscopy and relevant biopsy to complete the bowel evaluation. All biopsy specimens were evaluated by a single pathologist. Children were treated as the standard protocol of management of the conditions. Clinical follow-up of patients was done for 3 months.
SPSS (Statistical Package for the Social Sciences) software version 21.0 Chi-square test was used.
Out of the 110 children majority were girls (n = 62, 56.4%). Most of the children belonged to age group of 6–12 years (52.7%) (Table 1).
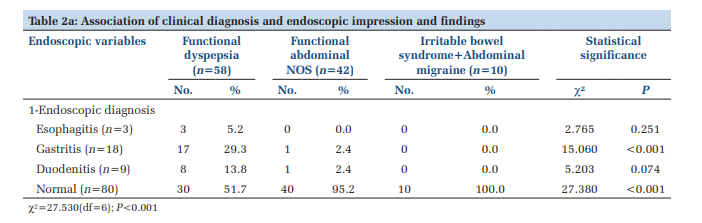
According to Rome IV criteria, 58 (52.7%) children were suffering from FD, 42 (38.2%) children suffering from FAP NOS, nine (8.2%) had IBS, and one child had AM. Endoscopic assessment showed 28 (42.3%) children with FD had significant lesion while it was seen only in 2 (4.8%) children with FAP NOS. Significant lesion on endoscopy in form of erythema, erosions in stomach was seen more in children with FD (P < 0.001) and none in IBS or AM (Table 2a and Figure 1).
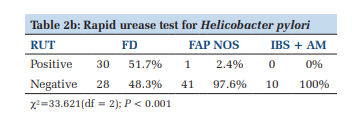
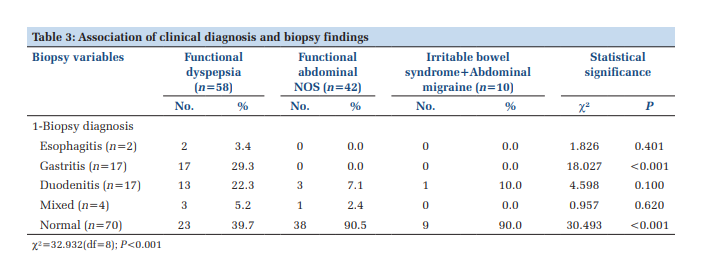
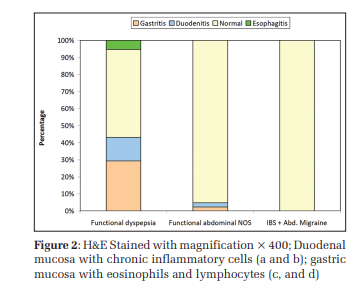
RUT for H. pylori was positive in 30 (51.7%) of children with FD, while only one in FAP NOS (P < 0.001) (Table 2b). Histological assessment of all biopsies was done (Figure 2). Inflammatory changes suggestive of gastritis, duodenitis, esophagitis or mixed involvement was seen in 35 children of FD while it was seen in only four children of FAP NOS and one child of IBS. Chronic Inflammatory changes in stomach suggestive of chronic gastritis were significant more in children with FD (P < 0.001), (Table 3 and Figure 3).
On clinical follow-up of 3 months 96.6% children with FD improved when given treatment with PPI and H. pylori (in positive cases) while 88% children of FAP NOS improved with treatment.
As per ROME 4 guidelines FAP disorders in children mainly incorporate four major diagnostic entities, namely, IBS, FD, AM, and FAP – NOS. Our study has tried to address the gap in knowledge regarding the role of GI endoscopy, RUT, and histopathology which by evidence is gold standard, in children in different variants of FAP disorders. Our study is probably the first study, evaluating the role of GI endoscopy and histopathology in children with FAP Disorders as described by ROME 4 criteria.
A total of 110 children aged 4–17 years (mean age 10.85 ± 3.68 years) were enrolled in the study. Majority of children were aged 6–12 years (52.7%), had a dominance of females (56.4%), and urban children (52.7%). The age and gender profile of children with abdominal pain syndromes varies significantly in different studies from across different parts of the world Puzanovova et al. in their study from USA, reported the mean age of children as 12.1 years and a dominance of females (62%).[6] Barupal et al. in their study from India found 75% children in 4–10 years range and reported a male dominance (53.9%).[7] In a recent study from Nepal, Upadhyay and Sharma (2017) reported the mean age of children as 10.2 years and a dominance of girls (59%).[8] Thus, age and gender profile in general seem to vary with respect to inclusion criteria and chance circumstances our findings suggest that upper GI endoscopy served as a helpful tool for the evaluation of children with FAP Disorders with a diagnostic yield of 37.5%. H. pylori gastritis was the most common finding (28.2%), followed by duodenitis (8.2%) as depicted by mucosal breaks in duodenum and reflux esophagitis (2.7%). In a study by Ukarapol et al., where 38 children having ≥3 episodes of severe upper abdominal pain, subjected to the upper GI endoscopy with biopsy. Majority of the children were female (n = 21; 58.3%) having mean age of 10.5 years. Organic causes were identified in 44.7% cases, with H. pylori gastritis being the most common diagnosis (28.9%). Improvement after institution of specific therapy was observed in all the patients.[9] Similarly in study by Sýkora et al., 56 children with FAP syndrome as per ROME 3 were evaluated, with mean age 12 years ± 2 years; H. pylori was seen in 27 out of 56 cases (30.4%) all having diagnosis of FD as per ROME 3 criteria.[4] Our study showed that in children with FD 51.7% were positive for H. pylori and most of them improved with the treatment for H. pylori. However, in another study by Thaakar et al. which included 290 children (4–18 years old; mean age, 11.9 ± 3.5 years; 93 girls) who underwent GI endoscopy for the primary indication of chronic abdominal pain. Esophagitis was seen in 21.0%; however, H. pylori infection was seen in only 2.0%, and medical therapy was effective in approximately 67% of these children.[3] This difference in H. Pylroi prevalence could be attributed to difference in the diagnostic modalities for H. pylori and variants of FAP included.
Most of the children recruited were from only two groups – FD and FAP NOS; hence, the two other categories of IBS and AM are not representative of general population. H. pylori was established on basis of RUT and not on actual demonstration of H. pylori due to lack of specialized staining facility at our institute. The follow-up time due to convenience was kept as 3 months. Hence, for future studies, we advocate a larger sample size including all age groups, longer follow-up and robust evaluation of histopathology samples to have a complete picture of FAP.



This is perhaps the first study on evaluating the role of endoscopy and histopathology in children with FGID based on the Rome 4 criteria. We found FD and FAP NOS were the two most common diagnosed variant among FAP disorders. Endoscopy, RUT for H. pylori and HPE in children with FD showed significant findings while endoscopy and further evaluation was of no added benefit in children with FAP NOS variant.
Hence, we recommend that categorization of type FAP on basis of ROME IV criteria by systematic history and detailed clinical examination is of prime importance. This will help in rational use of endoscopy and histopathology in further evaluation and treatment of these children.
Subscribe now for latest articles and news.