Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.2018.v04i01.003
Year: 2018, Volume: 4, Issue: 1, Pages: 15-17
Original Article
Archana Bhat1*, Rayna Roy2, T Umashankar1, C S Jayaprakash1
1Department of Pathology, Father Muller Medical College, Kankanady, Mangalore, Karnataka, India,
2Department of Undergraduate Medical Student, Father Muller Medical College, Kankanady, Mangalore, Karnataka, India
Address for correspondence:
Dr. Archana Bhat, Department of Pathology, Father Muller Medical College, Kankanady, Mangalore, Karnataka, India.
Phone: +91-9035572134. E-mail: [email protected]
Background: Cerebrospinal fluid (CSF) analysis is required to make a diagnosis of meningitis to aid in the proper management of patients. In urban areas with good health-care facilities, it is easy to get a CSF analysis done. However, in rural and remote areas with no proper transport facilities, such a simple point of care test will definitely be useful. We conducted a study and compared the results of reagent strip test with the biochemical tests and microscopic examination.
Aims and Objectives: The aim of the study was to determine the utility and efficacy of reagent strip test on CSF.
Materials and Methods: A prospective, time-bound study was carried out on the CSF sample remaining after the biochemical tests and microscopic examination. The values of both the methods were compared. Using Chi-square and Fischer’s exact test, data were analyzed.
Results: Protein reagent strip positivity had a high sensitivity of 100% for detection of CSF proteins >30 mg/dl, in our study.
Conclusion: This test will be useful in remote areas as a point of care test for early patient management.
KEY WORDS: Cerebrospinal fluid, meningitis, reagent strip.
Bacterial meningitis is more common in low- income settings than in well-resourced centers. It is a medical emergency and delay in treatment may lead to neurological damage or death. Cerebrospinal fluid (CSF) analysis is required to make a diagnosis of meningitis to aid in the proper management of patients.[1] In urban areas with good health-care facilities, it is easy to get a CSF analysis done. However, in rural and remote areas with no proper transport facilities, such a simple point of care test will definitely be useful. CSF studies have been determined in the past with the help of reagent strips, but the results are variable, and the method has not gained popularity. If proven useful these strips can be used as an excellent test to help clinicians make a rapid bedside diagnosis of meningitis and initiate treatment.[2] This would greatly benefit health professionals working in areas with limited resources.[3] Besides, these tests do not require any expertise and can be easily performed bedside[4] and interpreted. Despite its usefulness, this study is not gained importance because of lack of interpretation using proper cutoff values.[5] In our study, we have compared the results of reagent strip test with the biochemistry and microscopy to know if this simple test can be used as a point of care test in diagnosing bacterial meningitis.
The aim of the study was to determine the utility and efficacy of reagent strip testing on CSF proteins, glucose, and leukocytes.
Biochemical values (proteins and glucose) and microscopic examination (leukocyte number) were considered gold standard.
This study was conducted in the Department of Pathology at Father Muller Medical College, Kankanady, Mangalore, after obtaining ethical clearance from the Institute Ethics Committee. The study was prospective, conducted for a period of 2 months between July 6, 2017 and September 6, 2017, on CSF samples remaining after biochemical tests and microscopic examination. If the quantity of the CSF sample was insufficient for performing the index test, then those samples were excluded. The values of both the methods were compared. Normal CSF values used were leukocytes: 0–5 cells/micro l (adults) and 0–30 cells/microl (neonates), glucose: 50–80mg/dl, and proteins: 15–45mg/dl. Cutoff values used for diagnosing bacterial meningitis were CSF protein of >30 mg/dl, CSF glucose of < 50 mg/dl, and CSF neutrophils of >10 cells/mm3.
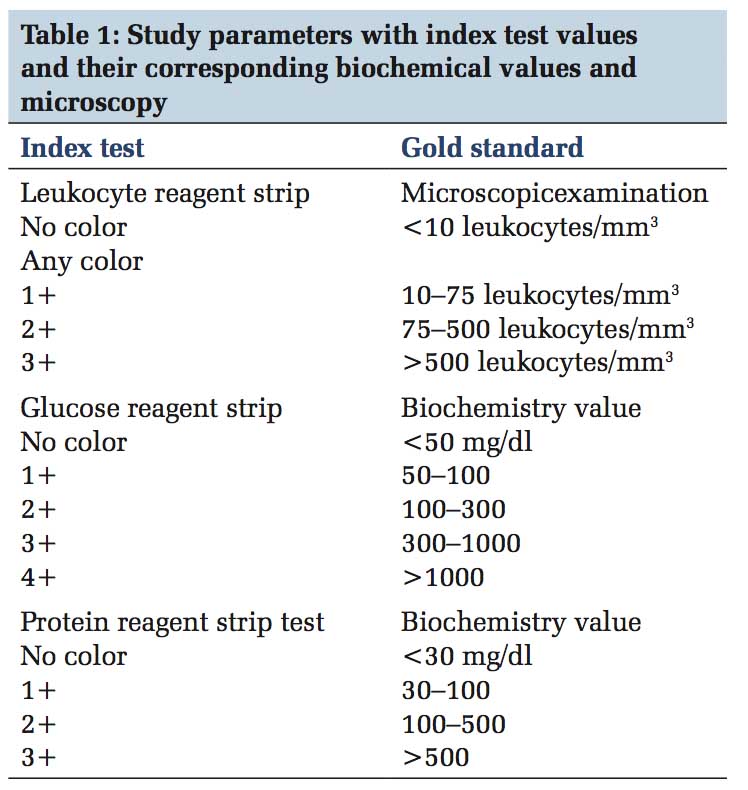
Reagent strip combur 10 test M (Roche, Germany) was used for the study and the parameters were analyzed as in Table 1:
CSF samples of 50 patients were included in the study. 60% of the patients were men (30/50). 26% of the patients were < 1 year of age (13/50). Median age was 17 years (range - 1 day to 76 years).
We estimated the diagnostic accuracy of the key indicator tests with reagent strip testing as the index test and CSF microscopy or biochemical laboratory- based values (CSF proteins and CSF glucose) as reference standards. Leukocyte esterase positivity by test strip had a sensitivity of 36.36% and specificity of 85.71% for detection of CSF granulocytes more than 10 cells/mm3. Protein reagent strip positivity had a high sensitivity of 100% for detection of CSF proteins >30 mg/dl, but the specificity was low, i.e., 28.57%.
Statistics To check the association between the gold standard and index tests the Chi-square test was done using Fisher’s Exact test. The results are as follows in Table 2.
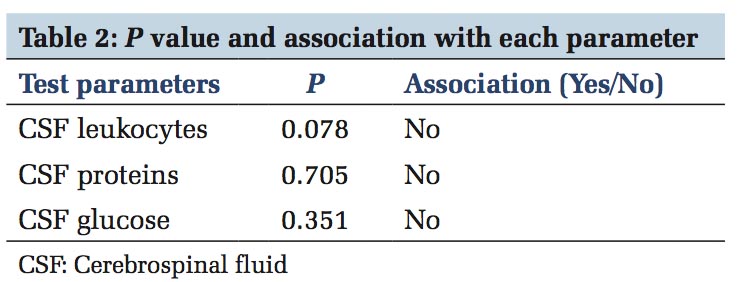
There is a good correlation between the results of reagent strip test and laboratory methods of CSF protein, sugar, and leukocyte estimation.
Parmar et al.[1] reported the sensitivity and specificity of the reagent strips for the diagnosis of meningitis as 97.14% and 96.42%, respectively. They observed sensitivity, specificity for tuberculous meningitis and bacterial meningitis of 100%, and 96.55%, and of 70% and 96.55% for aseptic meningitis. Accuracy observed for the diagnosis of meningitis as a whole, bacterial, tubercular, and aseptic meningitis were 96.78%, 98.2%, 98.27%, and 83.0%, respectively. Romanelli et al.[2] conducted a study on CSF samples of 164 children and obtained a sensitivity, specificity, positive and negative predictive values, and accuracy of 90.7, 98.1, 95.1, 96.4, and 96.1, respectively. They found a good correlation between the reagent strips and cytological and biochemical assays.
Moosa et al.[3] observed a sensitivity of 97% in the diagnosis of meningitis by reagent strip testing of CSF samples of 234 children with clinically suspected meningitis.
In another study involving 75 samples, sensitivity and specificity for testing CSF proteins by reagent strip was 77.8% and 100%, respectively, while that for CSF granulocytes was 92.6% and 100%, respectively.[4]
Study by Joshi et al.[5] involving 75patients found a sensitivity and specificity of 98.1% and 57.1%, respectively, for detection of CSF proteins >30 mg/dl. While the leukocyte esterase positivity had a sensitivity and specificity of 85.2% and 89.6%, respectively.
In our study of the total 50 cases, leukocytes of more than 10 were seen in 21 cases. In these 21 cases, dipstick for leukocyte esterase was positive in 11 cases. Of the 10 cases in which dipstick leukocyte esterase was negative, majority of them was viral meningitis. This is due to the fact that the dipstick detects granulocytes which have not degranulated their contents. In one case, the dipstick was positive though there were no granulocytes in microscopy. This could be due to blood contamination as a result of the traumatic tap.
In a study by Bisharda et al.,[6] 14 of the total 36 cases were confirmed to have meningitis by laboratory criteria. Of these, 12 were picked up by the dipstick test. Five samples tested positive by dipstick although their microscopic results were negative. They found a sensitivity of 85.26% and specificity of 77.27% in detecting pyogenic meningitis by dipstick test.
In a study by Molyneux and Walsh,[7] the sensitivity of the strips was only 33%, and the specificity was 83% on clear CSF samples.
In our study, 36 samples had a protein value of >30mg/dl while the dipstick was positive in 46 cases. There were 10 false positive cases on the dipstick.
In a study by Joshi et al., sensitivity and specificity for CSF protein >30 mg/dl was 95% and 57%, respectively. They were of the opinion that the sensitivity and specificity improved significantly when higher cutoff was used.
The important limitation of our study was the small sample size since this was carried out in a short duration of 2 months only. Furthermore, we have not documented and taken into account the physical appearance of CSF (turbid/clear).
Dipstick testing of CSF for proteins and granulocytes can be carried out as a point of care test in correlation with clinical findings and CSF physical appearance according to various studies. Also using a higher cutoff improves the sensitivity and specificity. However, the small sample size is the major drawback of our study.
Subscribe now for latest articles and news.