Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.2016.v02i02.007
Year: 2016, Volume: 2, Issue: 2, Pages: 37-40
Case Report
Riti T K Sinha1, Aniruna Dey2
1Visiting consultant, Department of Pathology, Mahatma Gandhi Institute of Medical Sciences, Sevagram, Wardha, Maharashtra, India,
2Assistant Professor, Department of Pathology, ESI Post Graduate Institute of Medical Sciences and Research, ESIC Medical College and ESIC Hospital & ODC (EZ), Joka, Kolkata, West Bengal, India
Address for correspondence: Aniruna Dey, Department of Pathology, ESI Post Graduate Institute of Medical Sciences and Research, ESIC Medical College and ESIC Hospital & ODC (EZ), Joka, West Bengal, India. Phone: +91-8902424614. E-mail: [email protected]
Isolated tuberculosis (TB) of the appendix is a rare occurrence. Its reported incidence is only 0.1-0.6%. The diagnosis is usually made only after histopathological examination of the resected specimen. The present case is of a 14-year-old male child who presented with signs and symptoms of acute appendicitis and was operated on. He was diagnosed with TB of the appendix on histopathological examination with no detectable focus elsewhere in the body. We report this case because of its rarity. The current article also emphasizes the importance of histopathological examination of all appendicectomy specimens.
KEY WORDS:Appendicectomy, appendicitis, appendix, granulomatous inflammation, tuberculosis
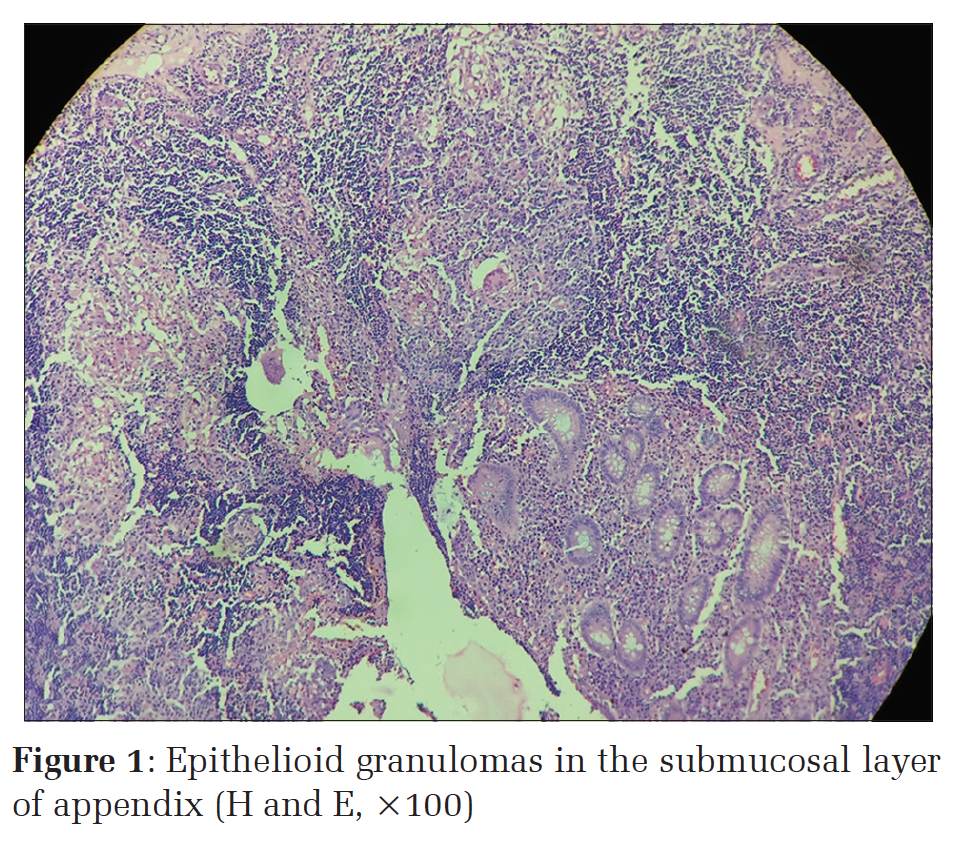
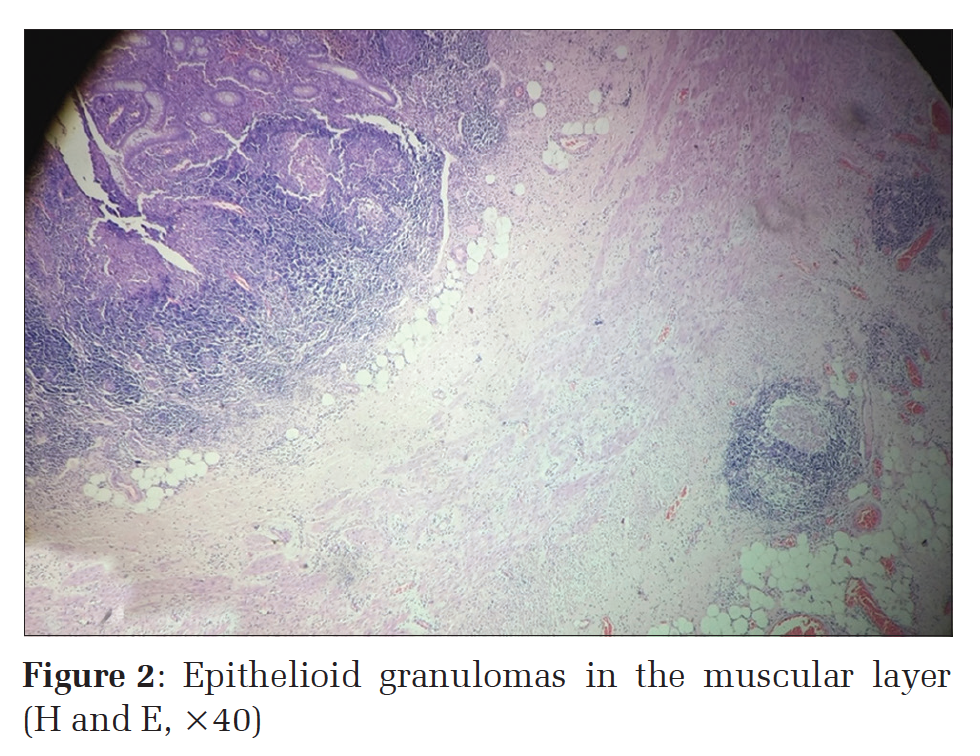
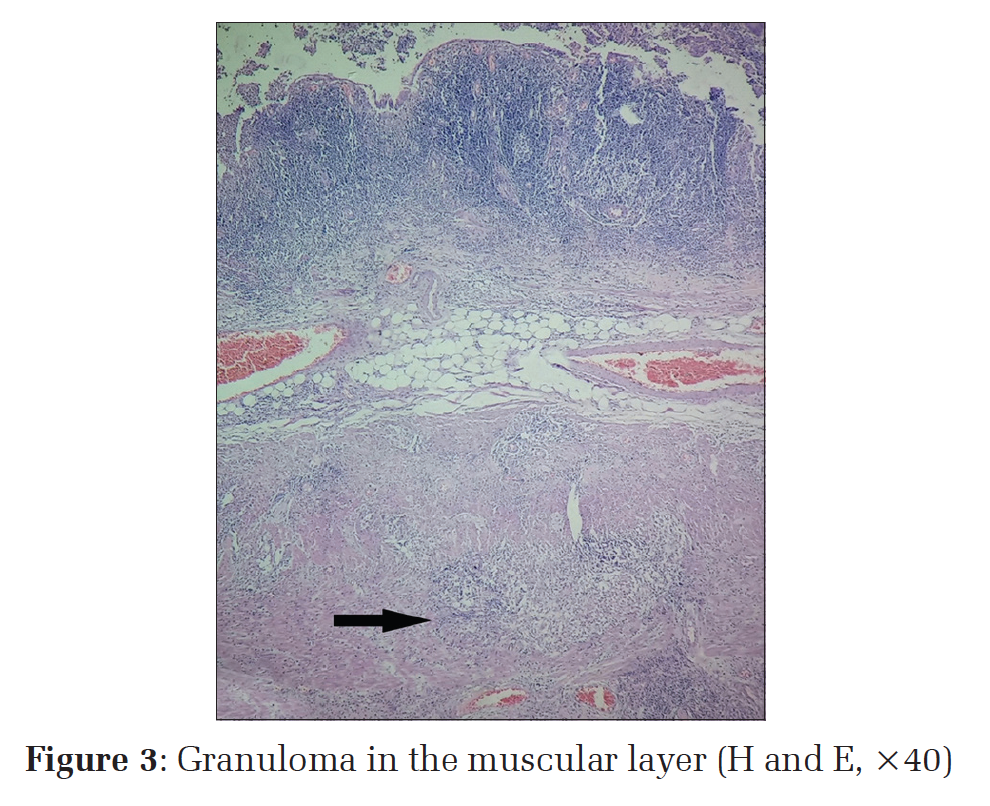
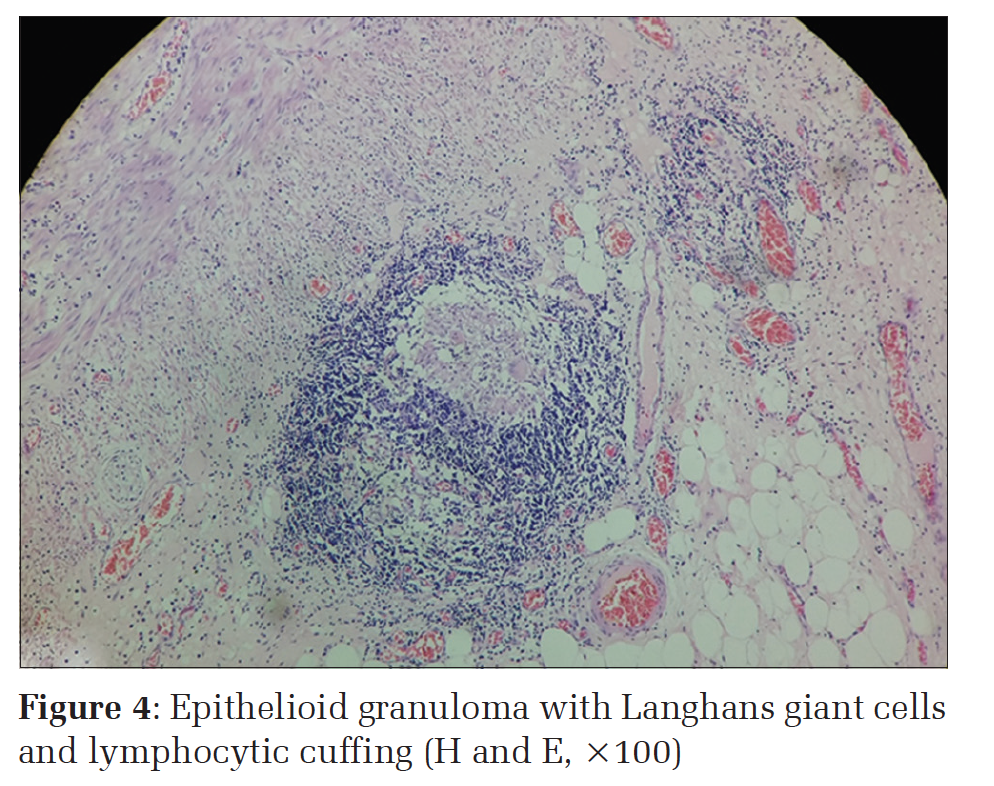
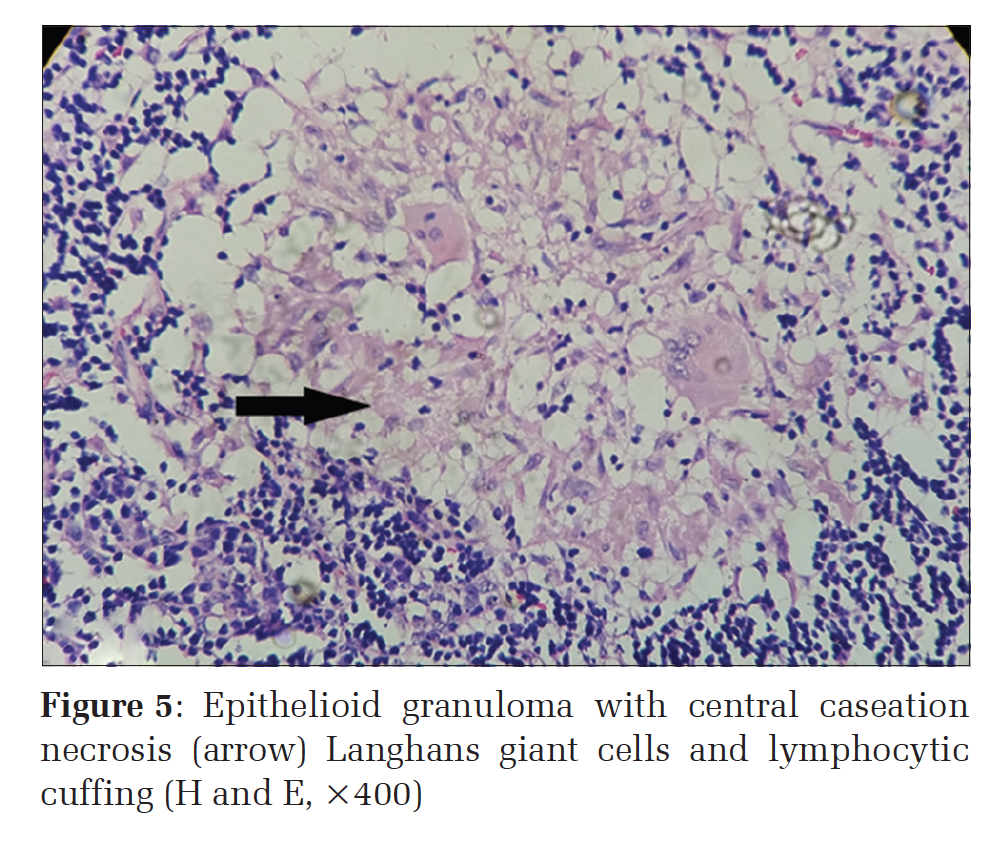
IntroductionTuberculosis (TB) is a major global health problem. The current global scenario of TB shows an estimated nine million cases of TB with more than one million people who died of the disease in 2013. India and China alone account for 24% and 11% of the total cases, respectively.[1] Terminal ileum, ileocecal junction, and peritoneum are the most common sites of TB in the abdomen. Although appendix is situated very close to the ileocecal region, primary appendicular involvement is very rare. Isolated TB of the appendix is rare with a prevalence of 0.1-0.6%.[2] Granulomatous inflammation of the appendix is rare. The reported incidence in western countries ranges from 0.14-0.3% and 1.3-2.3% in underdeveloped countries. The higher incidence in underdeveloped countries is believed to be due to increased incidence of TB and schistosomiasis and in developed countries due to Crohn’s disease.[3] We report a case of primary isolated TB of the appendix with no detectable tubercular focus elsewhere in the body. Case ReportA 14-year-old male child presented with complaints of acute onset severe colicky abdominal pain in the right iliac fossa of 1-week duration. On examination, he was average built with normal vitals. Local examination of the abdomen revealed a mass and tenderness in right iliac fossa. Examination of the other systems was normal. Routine blood count showed leukocytosis. Ultrasound of the abdomen showed thickened appendix, suggestive of acute appendicitis. Laparoscopic appendicectomy was done, and the specimen was sent to the histopathology section, Department of Pathology, ESIC, ESI Post Graduate Institute of Medical Sciences and Research, Joka, Kolkata, West Bengal, India. On laparoscopy, hyperemic edematous bowel loops with small areas of serosal neovasculature were seen. There was no evidence of ascites or fibrous bands. Grossly, the appendix measured approximately 8 cm in length with a thickened wall. The external surface showed congestion and periappendicular fibrofatty tissue. Sections were taken for histopathological examination and stained with hematoxylin and eosin. Microscopic examination revealed normal mucosa with areas of ulcerations and neutrophilic microabscesses at places. The submucosa and the outer muscle layer revealed the presence of wellformed epithelioid granulomas (Figures 1-3). On high power examination, the granulomas consisted of central areas of amorphous, granular, eosinophilic, caseous necrosis, epithelioid cells, giant cells of the Langhans’ type surrounded by a cuffing of lymphoplasmacytic infiltrate and fibrosis (Figures 4 and 5). Based on these histopathological features, a diagnosis of tubercular appendicitis was rendered. However, tubercle bacilli were not detected by Ziehl–Neelsen stain. Retrospectively, other relevant hematological and radiological investigations were done. Hematological investigations did not reveal any other abnormality except raised erythrocyte sedimentation rate of 60 mm 1st h. Mantoux test reading with purified protein derivative 10 TU was 8 mm. Sputum examination for acid-fast bacillus by smear and culture was negative. His chest radiograph was within normal limits. Computed tomography (CT) scan of the abdomen was normal. He was seronegative for HIV. He thus had no detectable tubercular focus elsewhere in the body. He was diagnosed as a case of appendicular TB and treated with the short course antitubercular regimen. The chest X-ray and the CT abdomen of the patient were within normal limits. Thus, the absence of tubercular focus elsewhere in the body confirms our case to be isolated primary TB of the appendix. DiscussionTB of the appendix was described by Corbin as early as 1873.[4] Its occurrence can either be primary or secondary, the former being very rare with a reported incidence of 0.1-0.6%.[2] TB is one of the most fatal and widespread illness in both the developed and developing countries, especially with the rising incidence of HIV. Most of the organs and tissues of the body can be affected by TB. The most common forms of non-pulmonary TB are TB of bones and joints (30%), urinary system (24%), lymph nodes (13%), sexual organs (8%), cerebrospinal meninges (4%), and gastrointestinal tract (3%). However, the involvement of the appendix, lying so close to the ileocecal region is rare. Due to the rarity and absence of any specific clinical and radiological finding, diagnosis of tubercular involvement of the appendix is made only after histopathological examination of the appendectomy specimen.[5] TB of the appendix may spread from neighboring organs, from distant focus by hematogenous route, lymphatic route, or from intestinal contents when contaminated sputum is swallowed.[4] There also can be an extension of the disease from neighboring ileocecal or genital TB.[6] The rarity of primary TB of the appendix may be because there is a minimal contact of appendicular mucosa with intestinal contents.[7] TB of the appendix is the only tubercular lesion that may manifest as three clinical forms.[6] The first type presents as an acute form that is indistinguishable from pyogenic appendicitis. The second clinical type presents with vague pain, occasional history of vomiting, diarrhea, and mass in the right iliac fossa. These cases are often indistinguishable from ileocecal TB. The third type is the latent one and found accidentally on histopathological examination of the appendix. Our case belongs to the second type though our case had colicky pain. Clinical symptoms can vary in patients. Rai et al. also reported a case of a 20-year-old male with acute onset colicky pain and mass in right iliac fossa, belonging to the second clinical type. It was diagnosed as TB of the appendix on histopathological examination.[2] Tauro et al. too reported similar two such cases of tubercular appendicitis.[8] Histologically, the caseating granulomas are seen involving the mucosa and submucosa, but when the route of infection is hematogenous or from the neighboring viscera, the granulomas are seen predominantly in the muscle and the serosal layers of the appendix as was seen in our case.[3] Granulomatous inflammation in the appendicular wall can also be seen due to foreign bodies, sarcoidosis, obstruction secondary to fecolith, mucocele, tumor, diverticulitis, Yersinia infestation, and systemic disease like Crohn’s disease. The presence of granulomas in an appendix specimen should prompt the search for Crohn’s disease elsewhere in the bowel, which was not present in our case. Crohn’s and Ginzberg, in 1932, in their initial description on regional ileitis, stated that the process never transcends the limits of the Bauhin’s valve and that the appendix is always spared.[9] Differentiating between Crohn’s disease and TB is very important because of the different approach to the management of these two diseases. The histological diagnosis of Crohn’s disease is characterized by transmural inflammation of appendicular wall with lymphoid aggregates and epithelioid granulomas.[10]
|
ConclusionTB is an endemic disease in our country. Hence, it is advisable to send every specimen of the appendix for histopathological examination. The rarity of the present case lies in the fact that appendicular TB was the initial presentation with no other detectable foci elsewhere. Timely diagnosis and management of the patient with anti-tubercular regime prevents complication such as sinus or fistula formation and spread to other organs. This ensures prevention of complications and complete cure. |
Subscribe now for latest articles and news.