Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.2015.v01i03.002
Year: 2015, Volume: 1, Issue: 3, Pages: 5-9
Original Article
A N Roopa1, K S Somashekara Reddy2, P Chandrashekara2, K R Umabai3, H S Madhuvan4
1Professor, Department of Pathology, MVJ Medical College & Research Hospital, Dandupalya, Kolathur, Hoskote, Bengaluru, Karnataka, India,
2Professor, Department of General Medicine, MVJ Medical College & Research Hospital, Dandupalya, Kolathur, Hoskote, Bengaluru, Karnataka, India,
3Associate Professor, Department of Pathology, MVJ Medical College & Research Hospital, Dandupalya, Kolathur, Hoskote, Bengaluru, Karnataka, India, 4Assistant Professor, Department of General Medicine, MVJ Medical College & Research Hospital, Dandupalya, Kolathur, Hoskote, Bengaluru, Karnataka, India
Address for correspondence:
Dr. A N Roopa, Department of Pathology, MVJ Medical College & Research Hospital, Dandupalya, Kolathur (P), Hoskote, Bengaluru - 562 114, Karnataka, India. E-mail: [email protected]
Aims: To study the prevalence of microalbuminuria, insulin resistance (IR), and metabolic syndrome in patients with essential hypertension (HTN). Materials and Methods: It’s a prospective study done on 50 consecutive hypertensive patients admitted in MVJ Medical College and Research Hospital and compared with controls. Detailed history, clinical examination and anthropometric measurements are taken. Estimation of oral glucose tolerance test, fasting insulin, urine microalbuminuria, fasting lipid profile, serum creatinine, and blood urea are done in all subjects. Standard 12 lead electrocardiogram taken to look for evidence of left ventricular hypertrophy and chest radiograph for cardiomegaly. Fundoscopy was done to look for hypertensive changes.
Results: Among the 50 patients studied, microalbiminuria was found in 70% patients. IR (homeostatic model assessment-IR >3.5 μU/ml) was noted in 20% of patients; all these patients had blood pressure (BP) of >190/100 mmHg. Of the total patients, 42.3% were freshly detected and none of them had IR. Dyslipidemia was observed in 61% and obesity in 42% of the patients. About 38.5% patients fulfilled the National Cholesterol Education Program Adult Treatment Panel 3 criteria for metabolic syndrome.
Conclusions: In our study 70% of hypertensives had microalbuminuria and correlated directly with degree and duration of HTN, but it was not statistically significant. Patients with dyslipidemia also had (70%) microalbuminuria. Microalbuminuric patients had a higher degree of end organ involvement as compared to normoalbuminuric patients. IR is seen in patients with very high BP and metabolic syndrome.
KEY WORDS:Insulin resistance, metabolic syndrome, microalbuminuria.
IntroductionHypertension (HTN) is a major public health problem. The incidence of HTN in India is 5-15% in adults against 10-12% in the West.[1] Microalbuminuria in patients with essential HTN is a marker of incipient glomerular dysfunction and clusters with lipid and hemodynamic abnormalities.[2] The National Kidney Foundation of the United States defines microalbuminuria as urine albumin excretion of approximately 30-300 mg/day in at least two out of three consecutive samples of non-ketotic sterile urine. The association of microalbuminuria with HTN is known from a long time ago. Microalbuminuria indicates an increase in renal endothelial permeability and it is an early marker of diffuse endothelial dysfunction.[2] Microalbuminuria is prevalent in 37.5% of patients with essential HTN and has positive correlation with the severity of HTN and thus may be an early marker for end-organ damage susceptibility.[1] Many patients with essential HTN, at the time of initial presentation may have symptoms related to target organ damage (TOD) involving the heart, kidneys, central nervous system, or retina. The blood pressure (BP) reduction using drug therapy is of greater advantage in reducing the target organ abnormalities and/or co-morbidities. For this purpose, assessment of sub-clinical TOD has become the key element in evaluating hypertensive patients. Microalbuminuria is one of the earliest indications of kidney injury in patients with diabetes mellitus and HTN and is associated with high incidence of cardiovascular morbidity.[2] Patients with essential HTN, both treated and untreated, appear to be insulin resistant in about 50% of cases, and cardiovascular risk factors are greatly accentuated in this subset of patients.[3] Microalbuminuria in essential HTN signals the presence of a selective impairment in peripheral insulin-mediated glucose uptake and enhanced insulin secretary response to glucose. Insulin levels rather than insulin sensitivity appears to be related to urinary albumin excretion.[4] Early detection of microalbuminuria, insulin resistance (IR) establishing metabolic syndrome will be helpful for early detection and prevention of occurrence of the cardiovascular and cerebrovascular disease and early treatment. This study was conducted to screen the patients with essential HTN for microalbuminuria and initiating aggressive management of detected cases might reduce the burden of chronic kidney diseases (CKD) and other end organ damage diseases in the community. Although the prevalence of essential HTN is high in India, but the relationship between microalbuminuria and TOD in HTN is not well studied. In this context, this study was conducted at the MVJ Medical College and Research Hospital, Hoskote. MATERIALS AND METHODSThis prospective study was done over a period of 2 years (2011-2013) and 50 patients with essential HTN were attended the medical outpatient clinic and/or admitted to the medical wards at the MVJ Medical College and Research Hospital, Hoskote were screened and compared with controls during this period. Proven cases of secondary HTN, pregnant women and those with diabetes mellitus (fasting plasma glucose values >110mg/dl and postprandial >140mg/dl), established renal disease including urinary tract infection were excluded from the study. Informed consent was obtained from each participant, and the study was approved by the institutional review board. Each participant was interviewed and examined in detail. Both patients undergoing treatment for HTN, as well as newly detected hypertensives of age group 40 years and above were included in the study (Table 1). The BP of each participant was measured, using the auscultatory method with a standardized calibrated mercury column-type sphygmomanometer with an appropriate-sized cuff encircling at least 80% of the arm in the seated posture, with feet on the floor and arm supported at heart level (except when the patient had stroke and had been unable to sit, in which case, BP had been measured in the lying pasture). Two separate measurements were recorded at 5 min intervals, and the average of the two values was taken as the BP at that moment. Similar BP measurements were done on three occasions, a week apart, and a BP above 140/90 mm Hg was regarded as HTN (using diagnostic criteria of JNC7). After excluding urine albumin by using urine strip positive patients, albumin negative urine samples centrifuged at 2000 rpm for 10 min, were used for quantitative estimation of albumin. The corresponding urine sample is also collected in sterile urine containers and was sent for culture to rule out any urinary tract infection. The blood samples of the selected Albustix negative cases were analyzed in Erba XL 300 biochemistry analyzer for fasting glucose, fasting lipid profile, blood urea, and serum creatinine levels by using photometry method. Oral glucose tolerance test also was performed to exclude pre-diabetics. Patients with diabetes (fasting plasma glucose values >110 mg/dl and postprandial >140 mg/dl), pre-existing renal insufficiency
Table 1: Criteria to select cases for studyCriteria to select casesHypertensive (newly detected and on treatment) Fasting blood glucose < 110 mg/dl and post-prandial blood glucose < 140 mg/dl Absence of macroalbuminuria (albustix negative) Urine culture – no growth Female in reproductive age – urine pregnancy test negative including urinary tract infection and pregnant women were excluded from the study (Table 1).
Fasting insulin (electrochemiluminescence immunoassay using cobase 601 immunoassay analyzers), urine microalbuminuria (immunoturbidimetric method by using Erba XL 300 biochemistry analyzer), standard 12 lead electrocardiogram taken to look for evidence of left ventricular hypertrophy (LVH). Chest radiograph was done to rule out cardiomegaly. Fundoscopy was performed to look for hypertensive changes. Computed tomography of the brain was done where ever necessary. People with normal body mass index without any systemic illness were included in the control group. In controls, fasting insulin and urine microalbuminuria were estimated. The relationship of microalbuminuria with the duration and severity of HTN, age, metabolic abnormalities and TOD such as hypertensive retinopathy, LVH, cerebrovascular accidents, and ischemic heart disease (IHD) was assessed by univariate analysis and using Chi-square test. |
||
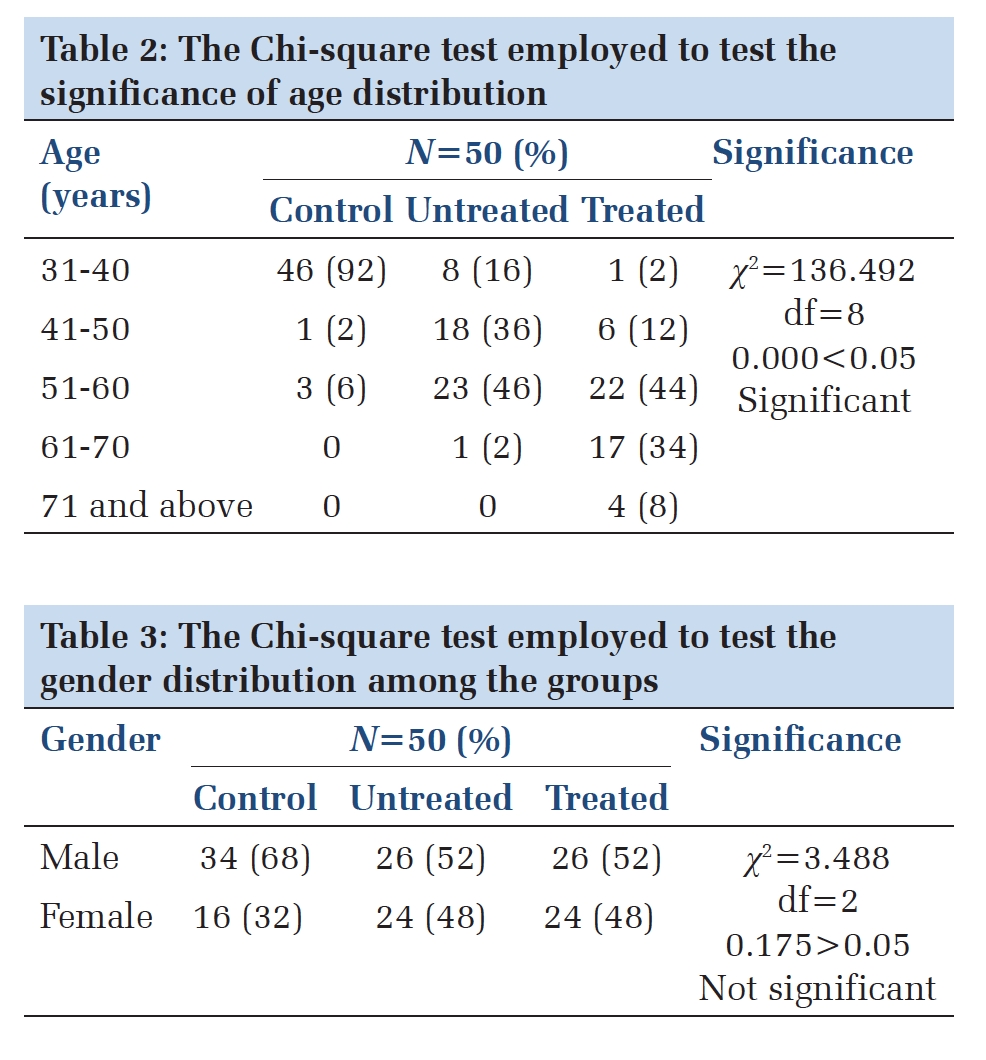
RESULTSThe data from 50 patients who satisfied the inclusion criteria during the study period were analyzed and compared with control group. Among them, 13patients were freshly detected hypertensives. Follow-up was done for 1-year period for TOD. Male and female ratio was 1:1 and mean age of patients were 59.53years. The prevalence of microalbuminuria among hypertensive patients increased steadily with their advancing age (Table 2). Microalbuminuria was noted in 35 patients and had a positive correlation with degree of BP (Table 3). None of the cases in the control group were positive for microalbuminuria. 37 patients with microalbuminuria had end-organ involvement, of which retinopathy in 16 (34%), LVH in 13 (28%), cardiovascular accidents in 5 (11%) and 3 (6.5%) patients had IHD (Figure 1). Among the 50patients studied, 45.7% patients had glucose abnormalities in the form of impaired glucose tolerance (19.3%), impaired fasting glucose (15.4%), and frank diabetes (11%). IR (homeostatic model assessment-IR >3.5 μU/ml) was noted in 20% of patients. All these patients had BP of >190/100mmHg. Of the total patients, 42.3% were freshly detected and none of them had IR. Dyslipidemia was observed in 21 patients, among them 11 had microalbuminuria. 16 patients fulfilled the National Cholesterol Education Program Adult Treatment Panel 3 criteria for metabolic syndrome, microalbiminuria was found in 11 patients (Table 5). Among the control group two cases showed IR (Table 6).
|
||
DISCUSSIONReported data from the United States shows that an overall prevalence of CKD has increased from 10% to 13% recently, and the majority of these have early CKD in the form of persistent microalbuminuria.[5] In India, till date no studies have done to investigate the prevalence of microalbuminuria among patients with essential HTN. The literature shows HTN is more prevalent in the age group above 40 years, hence the age group included in the study was 40 years and above.[6] The prevalence of microalbuminuria in our study was 70% that is higher than the prevalence of microalbuminuria observed (23%) in the LIFE study.[7] The prevalence of chronic renal failure (elevation of serum creatinine more than 1.8 mg/dl) was reported to be only 0.785% in a North Indian study,[8] this study did not consider the prevalence of early/ sub-clinical CKD in the form of microalbuminuria. Hence, our observation shows high prevalence of microalbuminuria in patients with essential HTN and must alert the clinicians regarding the high prevalence of subclinical CKD in this part of the world. Mani from South India[9] has studied on the preventive aspects for the reduction of the burden of CKD by early detection and treatment of HTN. The prevalence of microalbuminuria vary from 15% to 100%.[10] This variation is due to difference in the age, race, and severity of HTN (Table 4). Prevalence of an elevated urine albumin excretion increases with age, severity and duration of HTN, which is supported by our study. Even in treated patients prevalence can be as high as 25%.[1,10] Hypertensive TOD is more common in microalbuminuric patients as noted in our study. Estimation of urinary albumin excretion is a simple and a cost effective test to identify non-diabetic essential hypertensives at high risk and can thus can initiate aggressive treatment to get down to target BP.[11] Patients with elevated urine albumin excretion have higher left ventricular mass, a higher prevalence of hypertensive retinopathy.[12] Patients with severe HTN and microalbuminuria were found to have dyslipidemia and glucose abnormalities which are risk factors for CVD, early recognition and treatment of which will reduce the morbidity and mortality. In this study, none of the controls had microalbuminuria. Literature survey depicts the higher prevalence of microalbuminuria even in healthy people in some of the regions. This was associated with obesity, family history of HTN and diabetes mellitus.[13] Patients with severe HTN and microalbuminuria were found to have dyslipidemia and glucose abnormalities which are risk factors for CVD, early recognition and treatment of which will reduce the morbidity and mortality. Table 7 shows comparison of our study with Jalal et al.[1] and Toft et al.[14] studies. Our study shows higher incidence of microalbuminuria. Hyperinsulinaemia and peripheral resistance to insulin action seem to be features of microalbuminuric patients. It has been suggested that insulin promotes albumin transcapillary excretion, thus determining albuminuria. Microalbuminuria could be also as a result of insulin action at the renal level. When salt sensitive patients are given a high-sodium diet they show an increase in filtration fraction, glomerular pressure, and albumin excretion rate than salt-resistant patients. It has therefore been hypothesized that IR and salt sensitivity may interactively lead to changes in glucose metabolism and hemodynamics, both favoring albuminuria.[15] In this study, IR is seen in patients with very high BP and metabolic syndrome. Therefore, all hypertensives should be screened for diabetes and other categories of glucose intolerance as the increased insulin increases their risk of developing Type 2 diabetes mellitus. Two cases in the control group also were positive for IR.[16]
|
||
ConclusionIn our study, 70% of hypertensives had microalbuminuria and correlated directly with degree and duration of HTN, but it was not statistically significant. Patients with dyslipidemia had more chances of microalbuminuria. Microalbuminuric patients had higher degree of end organ involvement as compared to normoalbuminuric patients. Present study correlates with other studies in establishing microalbuminuria as a marker to predict end organ involvement in hypertensives. IR is seen in patients with very high BP and metabolic syndrome. All hypertensives with obesity should be screened for glucose abnormalities. ACKNOWLEDGEMENTSWe would like to thank Dr. M G Shivaramu, Principal Adichunchanagiri Institute of Medical sciences, Balagangadharanatha Nagara, Nagamangala Taluk, Mandya District & Executive editor in chief, JMSH for encouraging us to write this manuscript. We thank Dr. Shameem Sharieff Professor and HOD, Department of Pathology, MVJMC & RH, Hosakote, Bangalore for providing valuable comments and suggestions that greatly improved the manuscript. |
Subscribe now for latest articles and news.