Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.2015.v01i01.008
Year: 2015, Volume: 1, Issue: 1, Pages: 30-33
Case Report
Suprita P Nayak1, Balwant D Kowe2, Dinkar T Kumbhalkar3
1Assistant Professor, Department of Pathology, Government Medical College, Nagpur, Maharashtra, India,
2Associate Professor, Department of Pathology, Government Medical College, Nagpur, Maharashtra, India,
3Professor, Department of Pathology, Government Medical College, Nagpur, Maharashtra, India
Address for Correspondence:
Dr. Suprita P Nayak, A/203, Ganesh-Gauri Apartments, Khamla Chowk, Gumasta Layout, Nagpur - 440 015, Maharashtra, India.
Phone: +91-9975453094, E-mail: [email protected]
Primary adenoid cystic carcinoma (ACC) of the cervix is an extremely rare condition. It generally occurs in post-menopausal women with vaginal bleeding being the main presenting symptom. In the present case, a 68-year-old female came with the chief complaints of a gradual distension of abdomen and breathlessness. Clinical examination revealed a mass in the lower abdomen. Ultrasonography abdomen was suggestive of a neoplastic lesion probably arising from the uterus. Hysterectomy specimen revealed an enlarged uterus with dilated endometrial cavity, thinned myometrium, and the wall of the cervix diffusely thickened by a grayish-white infiltrative growth that had almost obliterated the endocervical canal. On histopathological examination, it was found to be a case of ACC of cervix. This case is being reported not only because of the rarity of ACC occurring in the cervix, but also because of its unusual presentation.
KEY WORDS:Adenoid cystic carcinoma, cervix, histopathology
IntroductionPrimary adenoid cystic carcinoma (ACC) of the cervix is extremely rare, accounting for < 1% of all cervical carcinomas and about 3% of all primary cervical adenocarcinomas.[1] It generally occurs in post-menopausal women, with the average age of most of the reported cases being about 20 years older than squamous cell carcinoma (SCC) of the cervix.[2] However, ACC of cervix occurring in younger age is also documented.[3] Clinical and radiological characteristics of primary ACC of the cervix are similar to those of SCC of cervix.[3] In most cases, the main presenting symptom of disease is vaginal bleeding.[3-5] ACC of the cervix tends to be more aggressive, with higher tendency to local and metastatic recurrence even when diagnosed in the early stages.[1] This case is being reported not only because of the rarity of ACC occurring in the cervix, but also because of its unusual presentation. |
||||||
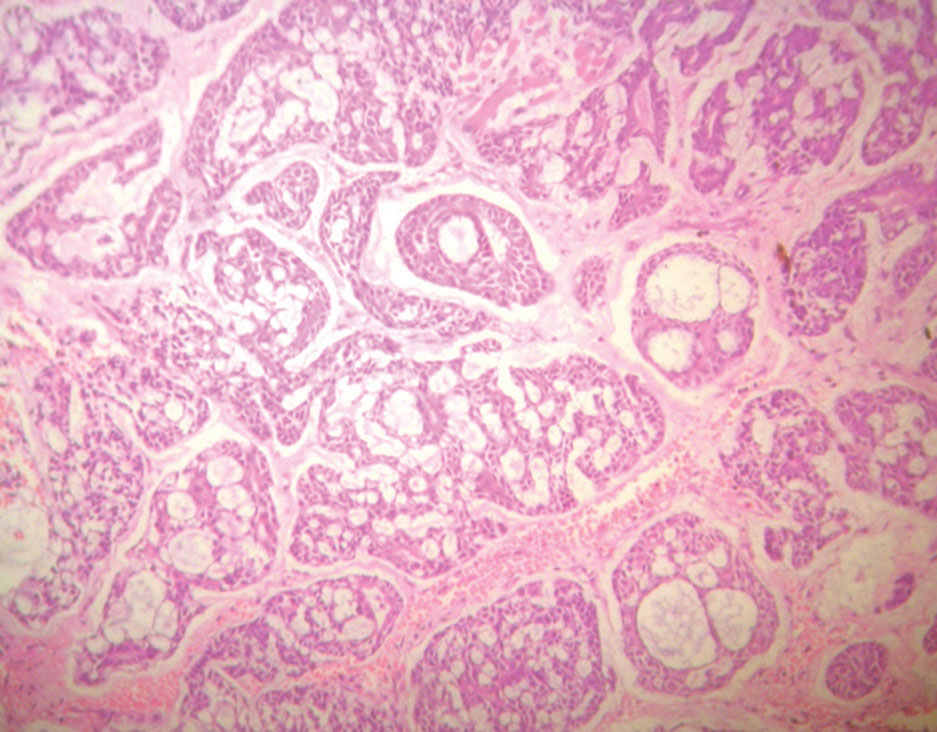
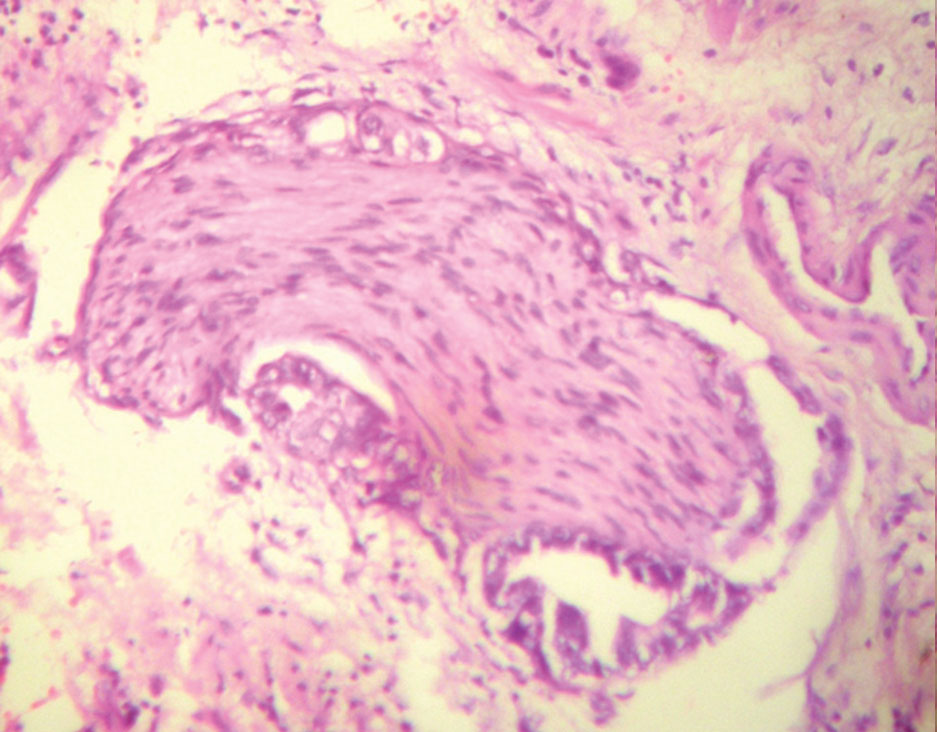
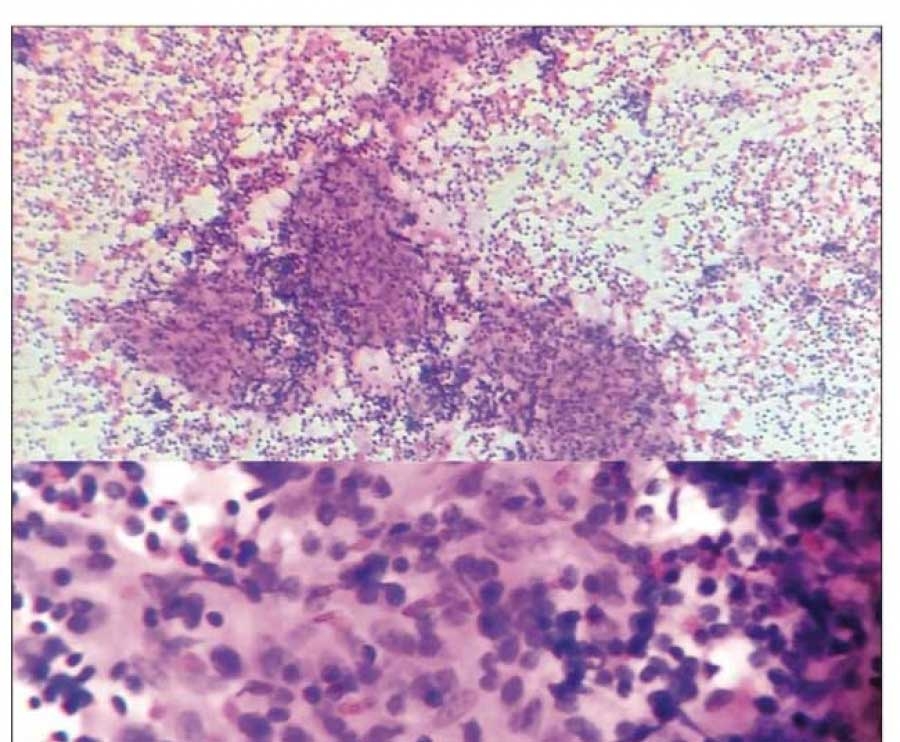
Case ReportA 68-year-old female came with the chief complaints of gradual distension of abdomen and breathlessness since 6 months. The lady had attained menopause 20 years back. Per abdomen examination revealed a large firm mass in the lower abdomen whose lower margin could not be reached. The same mass was also felt per vaginally while on per speculum examination the cervix was flush with vagina, and slight serosanguinous discharge was noted. On enquiry, she gave a history of slight blood- tinged discharge off and on since 4-6 months. Cervical scrape smear was done, but was not satisfactory for evaluation due to paucity of cells. Ultrasonography (USG) revealed 17 cm × 10 cm well-defined hypoechoic pelvi-abdominal lesion with multiple non-echoic areas. Internal echoes did not show any vascularity. The features were suggestive of a neoplastic lesion probably arising from the uterus. A USG- guided fine-needle aspiration was also done that yielded hemorrhagic fluid. A tentative clinical diagnosis of hematometra was offered. However, cytological examination of the fluid revealed clusters of degenerated atypical cells that were suspicious of malignancy. Computed tomography (CT) scan of the thorax revealed metastatic deposits in the left lung. To ascertain the type and nature of malignancy and decide further line of therapy, total abdominal hysterectomy with bilateral salpingo-oophorectomy was done, and the specimen was sent for histopathological examination. The uterus with cervix measured 15 cm × 9 cm × 3 cm. Cut section revealed a grossly dilated endometrial cavity containing dark fluid that spilled out on cutting. The myometrium was thinned, and the endometrial surface showed irregular blackish areas at places. The cervix was 3.5 cm in length, with a grayish-white growth causing diffuse thickening of the entire wall and causing narrowing and near obliteration of the endocervical canal (Figure 1). Bilateral adnexae were unremarkable. Sections from the cervix revealed variably sized smoothly contoured nests of cells that showed cribriform pattern with hyaline material in the punched-out spaces (Figure 2). The predominant population comprised of monotonous small cells with indistinct cell margins, scanty cytoplasm, round-oval nuclei and coarse chromatin. Few solid areas with cellular pleomorphism, occasional mitoses, and patchy necrosis were also noted. Perineural invasion in areas removed from the tumor mass was conspicuously present (Figure 3). The hyaline stroma was periodic acid-Schiff reaction positive suggesting basement membrane material while the cellular component was strongly positive for smooth muscle actin and S100 indicating its myoepithelial differentiation. Based on these findings a diagnosis of ACC of the cervix was offered. The endometrium was mostly sloughed off, but was atrophic wherever preserved. Additional interesting observation was the presence of severe dysplasia in the overlying squamous epithelial lining of the cervix. The patient was started on concurrent chemotherapy and radiotherapy, but after 6 months was lost to follow-up. |
||||||
|
||||||
DiscussionACC is known to occur at almost any site with a secretory gland component. It is usually more common in the salivary glands, with some of the less common sites of occurrence, besides uterine cervix, being breasts, lacrimal gland, prostate, esophagus, and lungs. Despite the architectural similarity, ACC of cervix as compared to its more common salivary gland counterpart sometimes showed more areas of necrosis, greater nuclear pleomorphism and increased mitotic rate.[6] These features were noted in a few areas in the present case too. ACC of cervix is traditionally associated with poor prognosis as it is locally aggressive and capable of metastasis to other organs even in its early stage.[1,3,4] These tumors spread most frequently to the lung, lymph nodes, abdominal cavity, and brain. Treatment is a judicious combination of radical pelvic surgery, radiotherapy, and chemotherapy.[1,3] In the present case too, one of the presenting complaints was breathlessness, with CT scan of the thorax revealing pulmonary metastasis. In the present case, besides the histopathological features of ACC, severe dysplasia was observed in the overlying squamous epithelial lining. This association of ACC of cervix with squamous or focally adenosquamous invasive or noninvasive carcinomas or dysplasia has been documented in most cases.[3,4,7,8] This is probably because ACC of cervix is thought to originate from the cervical subcolumnar multi-potent reserve cells in the transformation zone.[3,7] Studies have also shown two different types of the filaments, actin and keratin. Actin suggests myoepithelial differentiation, and it was presumed that the myoepithelial like traits represent a characteristic acquired secondarily in the process of the malignant transformation.[9] There are various reports that indicate that it is possible to detect ACC of the cervix cytologically at early stages even in the absence of colposcopically visible lesion.[5,8,10] However in the present case, neither were the dysplastic squamous cells nor were the cells or basement membrane material of ACC present in the Pap smear which was unsatisfactory due to paucity of cells. The probable reason for the inadequate representation in the Pap smear can be attributed to the infiltrative, rather than ulcerative or exophytic, growth of the malignancy causing diffuse thickening of the wall of cervix with resultant obliteration of the endocervical canal. In addition, this was also the probable cause of retained secretions that caused dilatation of endometrial cavity leading to the unusual main presenting symptom of distension of abdomen in the present case, and ultrasonography suggesting the dilated uterus to be the basic lesion. Adenoid basal carcinoma (ABC) is the most important differential diagnosis of ACC of cervix. The differentiation between the two is important, as most cases of ABC unlike ACC, have low potential for recurrence and metastasis.[6,11] Even though, both the conditions commonly occur in postmenopausal women, patients with ABC are usually asymptomatic, without any gross abnormality of the cervix. Histologically, ABC shows proliferation of nested uniform, bland basaloid cells with peripheral palisading pattern, but as against ACC there is minimal cellular pleomorphism, rare or absent mitoses and no necrosis. Immunohistochemically too, ABC does not show positive reactivity to actin, collagen IV, and laminin.[11,12] To conclude, this case is unique not only because of the rarity of ACC occurring in the cervix, but what adds to its uniqueness is its unusual clinicoradiologic presentation that was distinctly different and sets it apart from other reported cases of ACC of cervix. |
Subscribe now for latest articles and news.