Journal of Medical Sciences and Health
Year: 2022, Volume: 8, Issue: 3, Pages: 252-257
Original Article
R Yashica Gowda1 , Thejasvi Krishnamurthy1
1Department of Pathology, Kempegowda Institute of Medical Sciences, Bengaluru, Karnataka, India
Address for correspondence:
R Yashica Gowda, Department of Pathology, Kempegowda Institute of Medical Sciences, Bengaluru, Karnataka, India.
E-mail: [email protected]
Received Date:23 February 2022, Accepted Date:19 May 2022, Published Date:03 December 2022
Background: The nail is our most versatile tool and serves a very important function of protecting the distal phalanx. The nail unit shows specific changes that are markers for a wide range of local and systemic conditions. Objectives: The objectives of the study are to identify the spectrum of histomorphological features in various nail lesions and to highlight the role of histopathology in diagnosis of nail diseases. Methods: This is a descriptive study done over a period of 18 months. The nail biopsy specimens were received in 10 % formalin, softened with 10% nitric acid, processed and stained with routine Hematoxylin & Eosin [H&E] stains. Periodic Acid stain[PAS] stain was done wherever necessary. Histopathological examination by light microscopy was done to arrive at a precise diagnosis. Brief patient history and clinical features were also noted. Results: A total of 50 nail punch biopsies were examined. Psoriasis was the most common accounting for 38%. The combined approach of H & E and PAS stain was helpful in diagnosis of onychomycosis in 24%. Pigmentary disorders (14%) , lichen planus (10%) and alopecia areata (6%) were the other conditions observed. In 8% of cases microscopic features were nonspecific. Conclusion: The nail unit has a complex morphology with many peculiarities. Though it is quite accessible, it remains understudied. Histomorphological evaluation of nail punch biopsy is useful in understanding the involvement of nail in various dermatoses and also aids in the accurate diagnosis.
Keywords: Dermatoses, Histopathology, Nail biopsy
Nails are ectodermal appendages composed of compact translucent keratinised calls.1 Nail lesions present either as isolated nail pathology or as a manifestation of underlying systemic condition. Different nail disorders present with more or less similar clinical manifestations making clinical diagnosis difficult.2 In such cases, nail biopsy is warranted. It also aids in understanding the pathogenesis of nail diseases. But only a few studies on nail histopathology with limited number of patients have been carried out , as it is not routinely preferred by dermatologists. 3
In the current study, we aimed at identifying the spectrum of histopathological features in certain inflammatory, infectious and pigmented lesions affecting the nail unit to provide a precise diagnosis to the dermatologist. Understanding the complex histology of the nail is essential to arrive at a histological diagnosis.
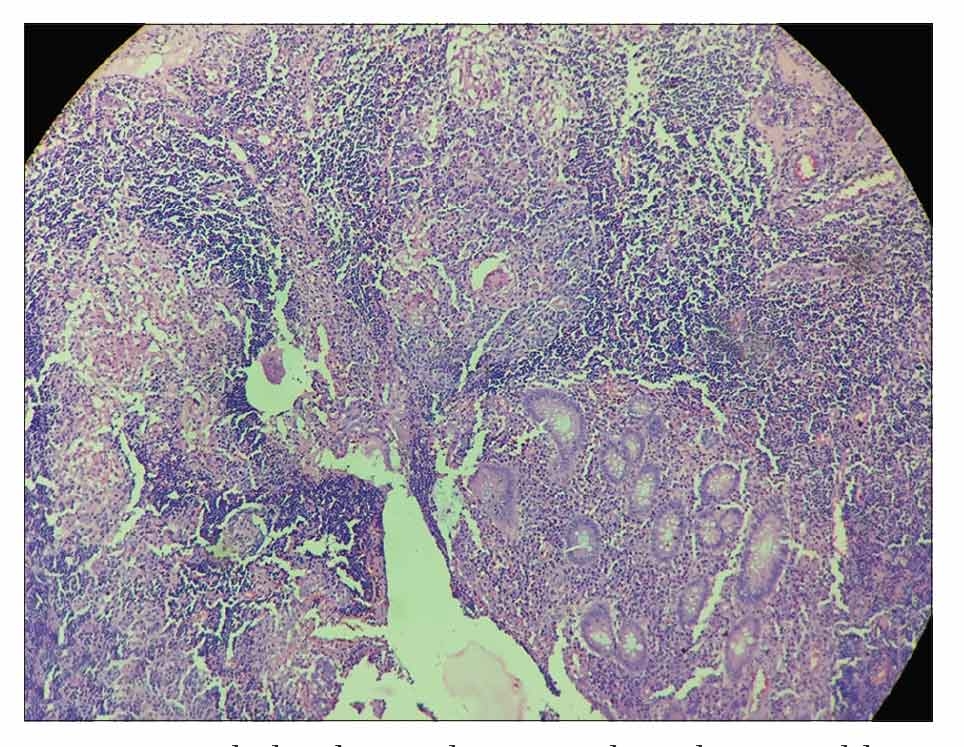
The nail unit comprises nail plate, nail bed and nail matrix. 4 The Nail plate consists of cornified dead cells. [Figure 1a] The Nail bed is situated below the nail plate and consists of thin epithelium with no stratum granulosum. [Figure 1b] Few inactive melanocytes may be present.
The Nail matrix is present below the proximal part of the nail plate. It is made up of papilliform germinative epithelial cells which keratinises to produce the nail plate by a process called onychokeratinisation. The rete ridges of the epithelium run obliquely in a proximal direction. 5 [Figure 1a]

Nail punch biopsies performed at the department of dermatology were received at the pathology department in 10% formaldehyde fixative. Decalcification of the biopsy specimens were done for a short duration (1-2 hours) using 10% nitric acid solution to soften the hard nail plate.
The biopsy samples were then routinely processed in an open type tissue transfer automated processor for a duration of 8 hours which involves processing through formalin, graded alcohols, xylene and molten paraffin wax. After which the processed biopsy sample is embedded in paraffin blocks and sections of 4-5 microns thick were taken using a microtome followed by Haematoxylin and Eosin staining. PAS [Periodic Acid Schiff] stain was done for biopsies where fungal infections were suspected.
A limited number of samples (50) were included in the study due to various factors like fewer indications for nail biopsies, reluctance by the patients, reluctant dermatologists in view of scarring seen in few patients following the procedure and also presence of co-morbidities in patients like diabetes mellitus and immunocompromised states.
We looked for the following specific features on microscopy:
In the nail plate-Hyperkeratosis, parakeratosis, fragmentation, pigment deposits, plasma crusting, fungal organisms.
In the nail base and nail matrix-acanthosis, spongiosis, exocytosis, basal cell vacuolar degeneration, pigment deposits.
In the subungual tissue-oedema, inflammation.
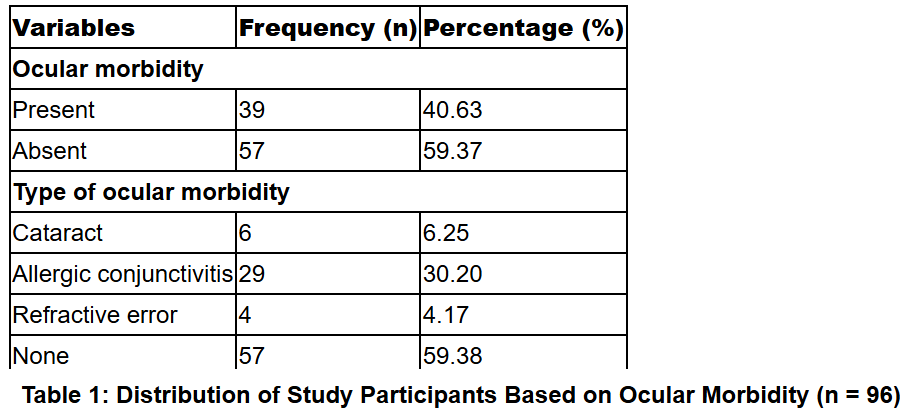
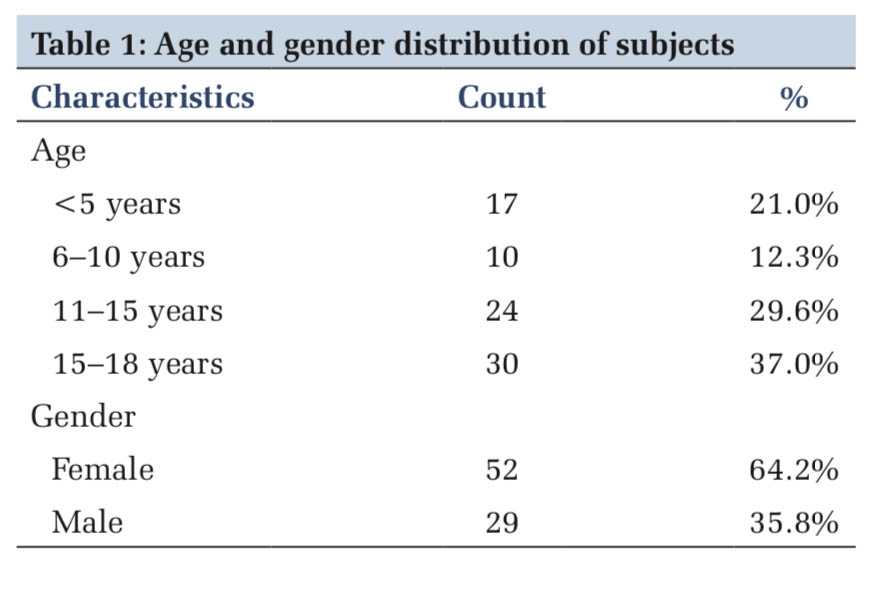
A total of 50 nail punch biopsies were evaluated. The nail histopathology showed diagnostic features in 46 cases. We observed a spectrum of interesting cases which includes inflammatory, infective and pigmentary diseases. The lesions noted were Psoriasis(19), Onychomycosis(12), melanonychia(07), Lichen planus(05) and Alopecia areata(03). Only in 4 cases the microscopic features were inconclusive. [Table 1]
|
Nail lesion |
Total number of cases (n=50) |
Percentage (%) |
|
Psoriasis |
19 |
38 |
|
Onychomycosis |
12 |
24 |
|
Lichen planus |
05 |
10 |
|
Pigmentary disorders |
07 |
14 |
|
Alopecia areata and atopy |
03 |
6 |
|
Inconclusive |
04 |
8 |
The nails are affected in various dermatoses like fungal infections, psoriasis, lichen planus, vesicobullous diseases and collagen vascular diseases. 6, 7 A majority of the nail changes seen in these diseases are caused by damage to nail matrix or nail bed which encourages the use of nail histopathological examination for precise diagnosis. Studies in the past have also highlighted the importance of histopathology of the nail unit as an etiologic and diagnostic tool.
Hanno et al studied predominantly inflammatory nail pathologies and found diagnostic features in 40% of their subjects. 2, 8 In a study by de Berker et al, 93.93 % biopsies
were diagnostic, but they evaluated mainly tumours.2 Grover C et al evaluated 60 nail biopsies and significant diagnostic changes were seen in 64 % of cases. 2 Hanno et al performed a study on patients with acquired nail dystrophies, at Henry Ford hospital and found that histopathology supported clinical diagnosis in 8 of 20 cases. 8
In our study, the nail histopathological examination showed diagnostic features in 92% of cases.
Psoriasis was the predominant disease in our study, as highlighted in Table 1.
Grover C et al studied nail biopsies in 32 patients and diagnosed psoriasis as the commonest lesion. 9
In a study by Nageswaramma S et al, paronychia and onychomycosis were predominant. 6 Hamza et al evaluated 50 patients with nail dystrophy and reported onychomycosis (47%) as the predominant disorder found in almost half of the cases. 10
Psoriasis presents with isolated nail involvement in about 5-10% of patients. 11, 12
The commonest clinical presentation of psoriasis was pitting of the nail plate, followed by subungual hyperkeratosis as seen in Figure 2a.
The most common histological change observed in our study was parakeratosis of the nail plate (n=19), followed by acanthosis of nail base (n=15) and nail matrix (n=5). Hypergranulosis of nail base was noted in 7 cases. [Figure 2a] Spongiosis and neutrophilic infiltration in the nail base epithelium were also seen in 3 cases. [Table 2]

|
Histopathologic features |
Number of cases |
Percentage (%) |
|
Parakeratosis |
19 |
100 |
|
Fragmentation of nail plate |
11 |
58 |
|
Plasma crusting |
3 |
16 |
|
Acanthosis of nail base |
15 |
79 |
|
Hypergranulosis |
7 |
37 |
|
Acanthosis of nail matrix |
5 |
26 |
|
Spongiosis |
3 |
16 |
Most of the microscopic findings in our study were in concordance with the study by Grover C et al and Dogra A. 11
In our study, onychomycosis was the second most common disease comprising 24% of all biopsies. Discoloration of the nail plate was the common clinical finding observed in our patients. [Figure 3a]
PAS staining is reported as the most sensitive method for the detection of hyphae in the nail unit (sensitivity 82%), compared to culture (sensitivity 53 %), direct microscopy with KOH (sensitivity 48%) and fluorescence brightener (sensitivity,53%).2, 5, 13, 14, 15, 16, 17, 18
The most common microscopic finding was fragmentation of the nail plate (n=11). [Figure 3b] Parakeratosis was seen in 5 cases and hyperkeratosis in one case. Acanthosis of the nail base epithelium was seen in 5 cases in our study. 2 cases showed hypergranulosis. There were no significant changes in the nail matrix. While 3 cases showed inflammatory infiltrate in the subungual tissue. [Table 3]

|
Histopathologic features |
Number of cases |
Percentage (%) |
|
Parakeratosis |
5 |
41 |
|
Fragmentation of nail plate |
10 |
91 |
|
Plasma crusting |
2 |
17 |
|
Acanthosis of nail base |
5 |
41 |
|
Hypergranulosis |
2 |
16 |
|
Acanthosis of nail matrix |
1 |
8 |
|
Spongiosis |
2 |
17 |
|
Fungal organisms |
12 |
100 |
In all the cases, PAS staining revealed the invasion of the nail unit by fungal hyphae. [Figure 3c] Overall, the presence of fungal hyphae on histology complemented by PAS staining was helpful in the diagnosis of onychomycosis in our study.
Grover C et al studied histology in onychomycosis in 15 patients using PAS staining and reported presence of fungal hyphae in 14 patients (93.3%). They also observed hyperkeratosis, parakeratosis, hemorrhage and serum crusts in the nail unit.18
Lichen planus limited to the nails is uncommon. It is seen in 1-10% of cases of disseminated lichen planus.2, 19, 6, 13, 14
4 out of 5 patients with lichen planus presented with pterygium of the nails which is the characteristic clinical finding as seen in a study by Tosti et al. 19 [Figure 4a] The characteristic microscopic findings noted in our study were fragmentation of the nail plate (n=3), hypergranulosis (n=3) and acanthosis (n=3) of the nail base combined with inflammatory infiltrate in the subungual tissue. 2 cases also showed civatte bodies in the nail base epithelium and basal cell vacuolar degeneration. [Figure 4b] The nail matrix was unremarkable in 4 out of 5 cases. [Table 4]

|
Histopathological features |
Number of cases (n=5) |
Percentage (%) |
|
Inflammatory infiltrate |
5 |
100 |
|
Fragmentation of nail plate |
3 |
60 |
|
Parakeratosis |
1 |
20 |
|
Acanthosis of nail base |
3 |
60 |
|
Hypergranulosis |
3 |
60 |
|
Civette bodies |
2 |
40 |
|
Basal cell vacuolar change |
2 |
40 |
There are very few studies on histopathology of lichen planus of the nails. Few of which include studies by Flores et al, Martin B and Grover et al. 2, 5, 14, 20 They have quoted that lichen planus of nails show similar features as skin which includes hypergranulosis, acanthosis, presence of civatte bodies and basal cell vacuolar degeneration. However exclusive features limited to the nails are parakeratosis, spongiosis and mild inflammation 2, 5, 14 which were also seen in our study.
The causes of abnormal pigmentation are numerous, including inflammation, physiological longitudinal melanonychia, trauma, drugs and several systemic disorders. 13 Moreover, nail biopsy is of specific use to rule out malignant melanoma of the nails.
All the cases which presented with pigmented bands clinically had melanoma as one of their clinical differentials. Hence, nail biopsy was of value to rule out melanoma in our study.
Either diffuse or focal pigmentation of the nail plate was observed both grossly and microscopically in all the 7 cases. 3 cases in addition had pigment deposits in the nail base. [Figure 5 a, b]

Between 10% - 66% of patients with alopecia areata have nail involvement. The nail changes may precede or follow the onset of alopecia. 21 Pitting of the nail plate was the presenting feature in two out of 3 cases of alopecia areata seen in our study. [Figure 6a]
Nails are targeted by the same type of inflammatory cells that target hair follicles in alopecia areata.
Characteristic microscopic nail changes in alopecia areata include lymphocytic infiltration and spongiotic vesiculation in the nail base epithelium. 22
The prominent microscopic changes observed in all the 3 cases were parakeratosis and plasma crusting of the nail plate with inflammatory infiltrate in the subungual tissue. [Figure 6b]

Histopathological analysis of the nail unit provides a wealth of information for diagnosing various nail disorders and to determine their pathogenesis and prognosis. Histopathological features and diagnostic criteria are available in the literature which needs to be utilised in interpreting the nail lesions. Though nail biopsies are not performed routinely, it gives a definitive rather than a hypothetical approach to treatment, especially in clinically ambiguous conditions.
Subscribe now for latest articles and news.