Journal of Medical Sciences and Health
Year: 2023, Volume: 9, Issue: 2, Pages: 190-196
Original Article
Ashmeet Kaur1 , Anita Harsh2 , Kapil Takhar3 , Kusum Mathur4 , Rateesh Sareen5
1Senior Demonstrator, Department of Pathology, SMS Medical College, Jaipur, 302021, Rajasthan, India,
2Professor, Department of Pathology, SMS Medical College, Jaipur, 302021, Rajasthan, India,
3Resident, Department of Pathology, SMS Medical College, Jaipur, 302021, Rajasthan, India,
4Senior Professor, Department of Pathology, SMS Medical College, Jaipur, 302021, Rajasthan, India,
5Senior Consultant, Department of Pathology, SDMH, Jaipur, Rajasthan, India
Address for correspondence:
Ashmeet Kaur, Senior Demonstrator, Department of Pathology, SMS Medical College, Jaipur, 302021, Rajasthan, India.
E-mail: [email protected]
Received Date:28 February 2023, Accepted Date:03 July 2023, Published Date:20 September 2023
Background: Neuromuscular disorders are rare, inherited progressive disorders leading to major disabilities over the years. As a group, there prevalence is not so uncommon and requires attention in view of their rising cases. Muscle biopsy forms an integral part of the diagnostic workup for patients with neuromuscular disorder but is performed in a very few institutes in Asia. In this study, we learn the spectrum of neuromuscular disorders presenting in a tertiary care centre of a developing country, India and evaluate the importance of open muscle biopsy. Material and Methods: 112 Muscle biopsies were reviewed and analysed for investigation of patients with suspected myopathy. Results: Of the 112 cases, 74% of the cases were adults. Mean age of presentation was 25 years and 57% of the cases were males. Pediatric cases constituted 26% of the total cases and 71% of them were male patients. Definitive diagnosis following muscle biopsy was made in 58% (n=65) of cases. Routine histological evaluation revealed the diagnosis of inflammatory myopathy 41% (n=46), muscular dystrophy in 34.8% (n=39),7.1% (n=8) neurogenic, 1.78%(n=2) mitochondrial and 0.8%(n=1) congenital myopathy of the cases. Conclusion: The burden of neuromuscular disorders has increased over the years. Molecular tests are not always helpful in diagnosing LGMD and not accessible to everyone. The role of muscle biopsy is inevitable in detecting false positive cases in mitochondrial myopathy, and for the management of Inflammatory myopathies. Awareness of the utility of muscle biopsy, expertise in diagnosing, and diagnostic challenges need more attention of the clinicians, pathologists and orientation of postgraduates to ease the journey of the patients and their families.
Keywords: Muscle biopsy, Enzyme histochemistry, Neuromuscular disorders, Mitochondrial myopathy, Inflammatory myopathy, Morphology
Most neuromuscular disorders are diverse subset of disease which are inherited and have a progressive course 1, where most affected individuals develop severe disabilities or even loose ambulation The literature studies mention a conservative estimate of an overall prevalence among both sexes as high as 286 x 106 that is, 1 in 3500 of the population may be expected to have a disabling inherited neuromuscular disease presenting in childhood or in later life. 2, 3 Accurate diagnosis is challenging and requires a multidisciplinary approach with interplay of signs, symptoms, laboratory tests, electrophysiological studies such as EMG, elaborate histopathology, immunohistochemistry and imaging studies. 4 Careful consideration of this information should be given prior to genetic testing, especially due to cost and difficulty in interpretation of the study result. So far, it is reported that the diagnostic yield of genetic tests varies from 18–60% dependingon the disease subtype as per literature.4, 5 Many variants of unknown significance are found, making the road to accurate diagnosis even more complicated.
At the same time, the role of muscle biopsy in diagnosis or supporting a clinical impression is ambiguous. 3 While some neuromuscular disorders require biopsy for definitive diagnosis, in others biopsy supplements the clinical diagnosis, 5 while biopsy is not required in few disorders like SMA, DMD, FSHD. The histopathological diagnosis requires adequate expertise and facility to meet out the diagnostic challenge posed by neuromuscular disorder. However, open muscle biopsy is an invasive procedure, hence should be wisely opted. 6
The present study was done at tertiary care government hospital in Western India which caters population from all over the state. The study gives an overview of demography, clinical profile, ancillary tests and histomorphological spectrum of Neuromuscular disorder over 3 year period 2020 to 2022.
The prospective study was conducted in the Department of Pathology, SMS Medical College, Jaipur. The subjects included are patients with clinical suspicion of Neuromuscular disorder who underwent muscle biopsy over 3-year period in the institute.
All the patients and their relatives included in this study gave informed consent, and the research protocols were approved by the Institutional Review Board or the ethics committee (779/MC/EC/2020) of the SMS medical college and Hospital (Jaipur, Rajasthan).
The clinical details, signs and symptoms, laboratory findings (Serum Creatinine Kinase), and electromyograph findings were recorded. The patient’s muscle biopsy was done after taking their consent for procedure. The diagnosis was done as per the following protocol. (Figure 1)

The biopsies were either formalin fixed or snap freezed. Frozen sections were stained with Hematoxylin and eosin, trichome, enzyme histochemistry5 and immunohistochemical stains. The final diagnosis of all patients were categorised in the following 7 groups:
Inflammatory myopathies
Muscular dystrophies
Congenital myopathies
Mitochondrial myopathies
Metabolic or toxic myopathies
Neurogenic atrophy
Indeterminate or No diagnostic pathology
Descriptive statistics was used using online free statistical calculator (Medcalis). Outcomes were evaluated for change in the initial clinical diagnosis and post biopsy diagnosis. Change in the diagnosis and post biopsy results were analysed using McNemar test. A p value < 0.05 was considered as statistically significant.
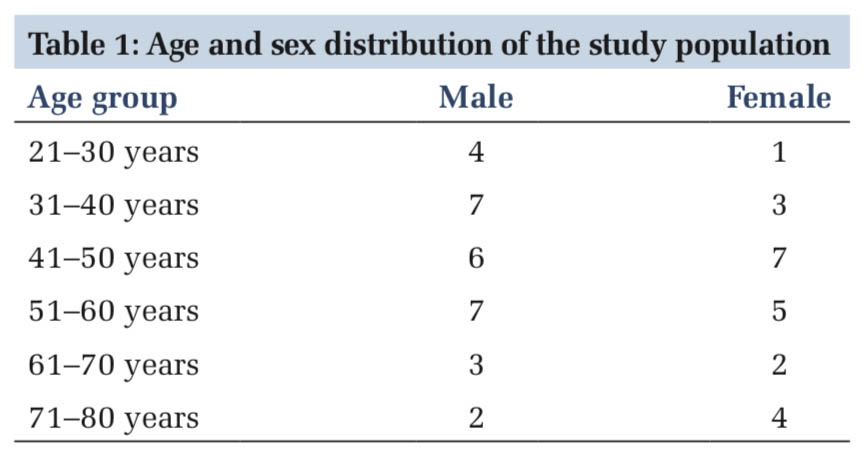
A total of 112 patients were included in the study, among which 62 (57.4%) were males and 46 (42.6%) were females. The majority of patients were in the age group of 11-20 yrs, with the mean age of study population be 25 years. The youngest patient was 7 months old and the oldest patient was 67 years old.
At the time of presentation, proximal weakness was the most common symptom in 43.7% (n=49 cases) where the patients complained of difficultly in standing from sitting or squatting position, climbing stairs, difficulty in raising arms above forehead. 15.1% (n=17 cases) reported distal weakness with slipping of slippers while walking or slipping of objects from hands. Other common symptoms encountered were myalgia 10 (8.9%), fever and dysphagia 8 (7.14%) as shown in Figure 2. A family history of similar affection was found in 12 (10.7%) cases and history of consanguineous marriage was obtained in 8 cases.

Developmental delay was noted in 12 cases (42.8%). Most common complaint in paediatric age group was frequent falls in 18 cases (64.3%). The affected children could not walk as fast as their peers and running was impossible for few (28.5%, n=8).
On physical examination, characteristic signs like scapular winging (n= 6), Gower sign (n= 8), polyhill sign (n= 3) and diamond sign (n= 1), were observed. Lordosis (n=2), Bulbar symptoms (n=8), respiratory problems (n=7) and gait abnormalities (n =6) were also observed. (Table 1)
|
Sl. no |
Examination Finding |
Frequency |
|
|
1 |
Motor weakness in lower limbs |
Proximal |
20 |
|
Distal |
12 |
||
|
2 |
Motor weakness in upper limbs |
Proximal |
29 |
|
Distal |
5 |
||
|
3 |
Facial weakness |
|
4 |
|
4 |
Bulbar symptoms |
|
8 |
|
5 |
Ptosis |
bilateral |
1 |
|
6 |
Bulk |
atrophy |
31 |
|
hypertrophy |
6 |
||
|
pseudohypert-rophy |
9 |
||
|
7 |
Resp weakness |
|
7 |
|
8 |
Characterstic Signs |
Scapular winging |
8 |
|
Gower Sign |
8 |
||
|
Diamond sign |
2 |
||
|
Polyhill sign |
2 |
||
|
Myotonia |
1 |
||
|
9 |
Deformities |
Contractures |
9 |
|
Lordosis |
2 |
||
|
10 |
Gait abnormalities |
|
7 |
|
11 |
Other |
Skin lesions |
6 |
|
Interstitial Lung Disease |
3 |
||
EMG study showed myopathic pattern in 72%, irritable myopathy in 12%, neurogenic in 9.2%, and normal EMG in 6% patients. Creatinine Kinase were normal (up to 200 IU) in 18% (n=20), slightly elevated (200-5000 IU) in 52% (n=56), and elevated (>5000 IU) in 30% (n=33).
On routine histological evaluation, Inflammatory myopathy 41% (n=46), Muscle dystrophy in 34.8% (n=39), neurogenic 7.1% (n=8), mitochondrial 1.78% (n=2) and congenital myopathy 0.8% (n=1) were diagnosed. (Figure 3)

46 (41%) cases of inflammatory myopathy were further sub-classified as polymyositis, dermatomyositis, immune mediated necrotising myopathy, necrotising myopathy, and inclusion body myositis as per the integrated classification.7 However, 18 cases out of 39, of muscular dystrophies could not be sub classified as majority cases (n=13) were received in formalin, while others show either multiple protein defects. Among the paediatric patients, 17 cases were included in this group, where majority were diagnosed DMD (41.2%, n=7) and 1 case of BMD, on the basis of IHC findings, in correlation with clinical findings.

Neurogenic was the third most common group comprising 3 cases of SMA, One of ALS (involving upper motor neuron) and 4 cases had peripheral nerve involvement. Specific diagnosis based on muscle biopsy study is shown in Table 2.
|
Diagnostic categories |
Specific diagnosis |
Total Cases |
|
Inflammatory myopathy (N=46) |
Polymyositis |
24 |
|
Dermatomyositis |
7 |
|
|
IMNM |
8 |
|
|
NM |
4 |
|
|
IBM |
3 |
|
|
Muscular dystrophy |
Dystrophinopathy |
8 (1 - BMD) |
|
Dysferlinopathy |
3 |
|
|
Calpainopathy |
2 |
|
|
Sarcoglycanopathy |
2 |
|
|
Uncertain (FSHD, Multiple protein deficiencies, no IHC) |
24 |
|
|
Congenital myopathy |
Core Disease |
1 |
|
Mitochondrial myopathies |
PEO |
1 |
|
Other |
1 |
|
|
Neurogenic (n=8) |
SMA |
3 |
|
ALS |
1 |
|
|
Peripheral nerve involvement |
4 |
The change in prebiopsy and post biopsy results were analysed for all categories using McNemar test. (p value < 0.05 was considered as statistically significant). The pre and post biopsy diagnosis for inflammatory myopathy, muscular dystrophy, neurogenic atrophy and congenital myopathy were similar without statistically significant difference. (Table 3) However, mitochondrial myopathies were over diagnosed prior to biopsy. Prebiopsy 10 cases (8.9%) had mitochondrial myopathy as diagnosis whereas post biopsy only 2 (1.7%) patients were diagnosed with mitochondrial myopathy (McNemar p=0.0269) (Table 4).
|
Diagnostic groups |
Prebiopsy diagnosis (n=108) |
Post biopsy diagnosis (n=108) |
|
Inflammatory myopathies |
50 |
46 |
|
Muscular dystrophies |
43 |
39 |
|
Neurogenic atrophy |
8 |
8 |
|
Congenital myopathies |
1 |
1 |
|
Mitochondrial myopathies |
10 |
2 |
|
No diagnostic pathology |
|
16 |
|
Total |
112
|
112
|
|
Mitochondrial myopathies |
Post biopsy |
Total |
McNemar p value |
||
|
Diagnosed |
Not diagnosed |
||||
|
Pre biopsy |
Suspected |
1 |
9 |
|
|
|
|
Not suspected |
1 |
86 |
96 |
0.0269 |
Out of the 46 patients with inflammatory myopathies, 22 patients were given combination of steroids and immunosuppressive therapy prior to biopsy, while the remaining 24 patients were managed on prednisone. After biopsy, only 12 continued to receive immunosuppressive therapy, 2 were given rituximab and 1 was given IvIg. Hence, the impact of muscle biopsy was that 13 patients had change in treatment in the form of immunosuppressive agent alone, IvIg or rituximab
Muscle biopsy processing is a new and challenging technique due to technical and analytical expertise needed at the centers. The present study conducted at the medical college of state capital gives an overview of the diagnosis of neuromuscular disorder in the country. 8
In the evolving era of molecular diagnostics, the utility of muscle biopsy cannot be underestimated as it is cost effective and therefore every specialised laboratory at tertiary care hospital should adopt to techniques for diagnosing muscle biopsy.
The mean age of the presentation was 25 years and 57.4% of them were males. Majority patients were in the age group 11-20 yrs. Paediatric population comprise 26% only, although neuromuscular disorders have higher prevalence in paediatric age group. 9 This is because many clinicians and patients opt for non-invasive molecular tests for diagnosis of these disorders as also observed by Manisha et al. 10 in her study.
The integration of prebiopsy workup with clinical features, lab finding adds to diagnostic value in suspected cases of myopathy. 11 Tenny et al. 9 also documented that biopsy provides a sensitivity of 63%. Change in the prebiopsy diagnosis was observed in the study due to false positive (n=31) and false negative (n=16) cases. Sensitivity of post biopsy diagnosis was 68.6% which is significant (p<0.05). The findings of the present study were similar to those by CH Lai 12 , where specific clinical diagnosis on muscle biopsy was made in 43% of cases. Biopsy resulted to a specific clinical diagnosis or changed the diagnosis/treatment in 74% of patients.
The most common etiology of Neuromuscular disorder in the present study was Inflammatory myopathy (predominantly in adults). Majority of these myopathies are autoimmune mediated particularly, cell mediated characterised by CD8+ T cells which secrete cytotoxic granules leading to necrosis of muscle fibrs. Mediators of innate immunity, non-immune mechanisms (NFKB activation, ER stress) and even HLA association is also identified. 13 Most patients of inflammatory neuropathies presented with aching pain, rapidly progressive proximal weakness and skin, lung involvement in few cases. Secondary association with infections, malignancy and systemic illness are also established. Hence, histopathology shows characterstic inflammation, both in endomysium and perimysium, which is variable-histiocytic (CD68+ in IMNM), T cell mediated (predominant CD4+in PM/predominant CD8+ in IBM) or B cell mediated. On the basis of these inflammatory infiltrate, their location and characteristic MHC1 expression on the sarcolemma, various subtypes were differentiated. Perifasicular atrophy and MAC (membrane attack complex) expression on endomysial blood vessels were diagnostic features of Dermatomyositis. Distal weakness, dysphagia and histologically presence of rimmed vacuoles were observed in the cases of Inclusion body myositis.
It was interesting to note that our study did not report the commonly described primary and secondary neuromuscular diseases (Muscular dystrophy/Limb Girdle Muscular Dystrophy) described in literature, but inflammatory myopathy was the largest group, as our study was limited to patients undergoing muscle biopsy, while molecular tests were preferred for children owning to their non-invasive nature. Our findings are similar to Lai CH et al. 12 , where also the predominant group was inflammatory myopathy (40%) and Laguna et al. (50%). 14
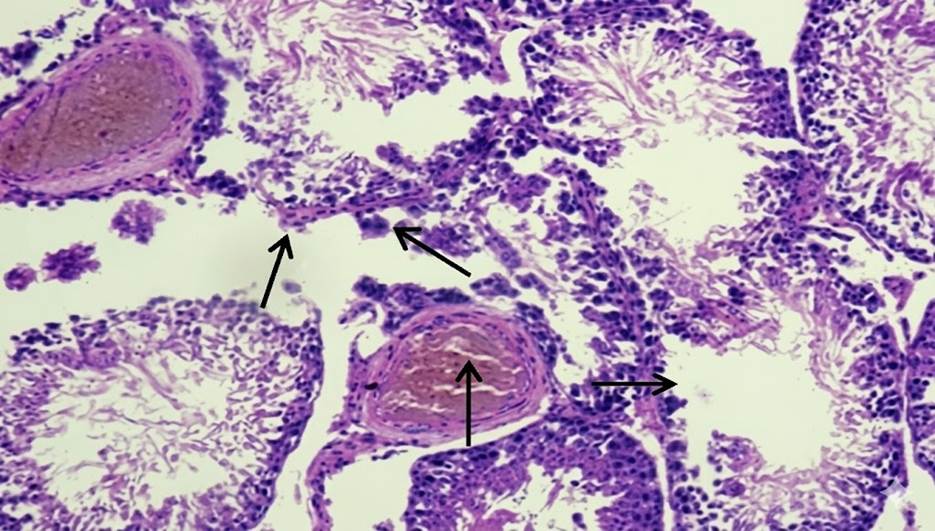
The most common neuromuscular disorder among the children in the present study was Muscular dystrophy. This is a heterogenous group with genetic association. These are clinically classified as congenital and non-congenital (inherited). Congenital muscular dystrophies, namely Merosin/Ulrich and Dystroglycanopathies are presented at birth. 13 We did not encounter any biopsy of a neonate for the same in our study, for genetic tests were preferred by the paediatricians for establishing the same. However, among the non-congenital group, clinically, most of the children presented with development delay in the form of delayed walking and poor physical activity as compared to peers. Histologically, muscle architecture was effaced with varying degree of fat and connective tissue infiltration. Variation in fibre size, atrophic fibres, hypertrophic fibres, splitting of fibres, increased internal nuclei were the predominant findings. Immunostains, namely, Dystrophin, Dysferlin, Sarcoglycans (alpha, beta, gamma, delta), Calpain, Caveolin and Desmin were applied to further categorise Limb Girdle Muscular Dystrophy. However, while considering the group of patients in muscular dystrophies, myopathy of unspecified cause is of special interest. Indeed, 43 patients (38.3% of cases) presented with a myopathy mimicking limb-girdle muscle dystrophy, i.e., with progressive weakness in proximal or distal muscles, and dystrophic or myopathic muscle pathology was seen in 39 (34.8%) cases on muscle biopsy. However, we failed to identify significant IHC findings in three patients. This observation was also noticed by Eachaniz Laguna et al. 14 Similarly, multiple protein deficiency (patchy alpha sarcoglycan and dysferlin, patchy beta sarcoglycan and dysferlin) were observed in 5 cases. This cohort of patients may therefore provide a valuable resource for identification of novel mutations. 14, 15
Neurogenic muscular dystrophies are inherited and acquired clinical disorders characterised by defect in upper/lower motor neurons or peripheral nerve. 13 Histological changes in muscle biopsy usually occur as a result of denervating process. Atrophic fibres, angulated fibres and grouping of fibres/clustering of the two population of fibres were seen in the biopsies. Enzyme histochemistry showed characteristic loss of checkerboard pattern with grouping of one type of fibres (ATPase) and target fibres (Oxidative stains). Our findings are similar to Lai CH et al., 12 where neurogenic changes were observed in 12% of the cases.
Muscle biopsy plays an important role in establishing an etiologic diagnosis and is required for prognostic, predictive and therapeutic planning. Molecular tests, although non-invasive and easy to perform has its own limitations. Multi gene neuromuscular disease panels are unproven, costly and not medically required, if muscle biopsy is available, due to insufficient evidence of efficacy. The need of expertise and diagnostic challenges of Neuromuscular disorders requires greater exposure of post graduate students to timely diagnose these cases, provide optimum rehabilitation to improve the quality of life of the affected and genetic counselling to the family.
Subscribe now for latest articles and news.