Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.2016.v02i02.006
Year: 2016, Volume: 2, Issue: 2, Pages: 29-36
Original Article
K Humsene1, N Krishnaveni2, B Sarada3
1Assistant Professor, Department of Radiology, MNR Medical College & Hospital, Sangareddy, Medak, Telangana, India,
2Professor, Department of Radiology, Government Medical College, Ananthapuramu, Andhra Pradesh, India,
3Assistant Professor, Department of Radiology, Government Medical College, Ananthapuramu, Andhra Pradesh, India
Address for correspondence: Dr. N Krishnaveni, Department of Radiology, Government General Hospital/Government Medical College, Ananthapuramu, Andhra Pradesh, India. Phone: +91-9440337737. E-mail: [email protected]
Background: The presence of open fontanelle in infants plays a major role in the ability to image the brain with ultrasound. The premature infants are more prone for hypoxic-ischemic insults and complications, which on early diagnosis helps the neonatal brain to protect from further insults.
Aims and Objectives: Evaluation of intracranial pathologies by transcranial neurosonography in neonates and infants, by dividing into three groups: Preterms before 34 weeks, after 34 weeks, and unrelated to gestational age. All preterms and neonates are scanned early to diagnose intracerebral hemorrhages, hypoxic-ischemic encephalopathy (HIE), infections, and congenital problems and later follow-up scans to identify its complications for the timely management of neonate.
Materials and Methods: A total of 165 infants with clinical suspicion evaluated on neurosonogram for 2 years. The study was conducted in the Department of Radiology using multi-frequency convex probe, sector probe and small linear probe, and Doppler flow studies. The babies were screened in coronal, sagittal, parasagittal planes using anterior fontanelle, transtemporal as an acoustic windows, and additional views whenever necessary.
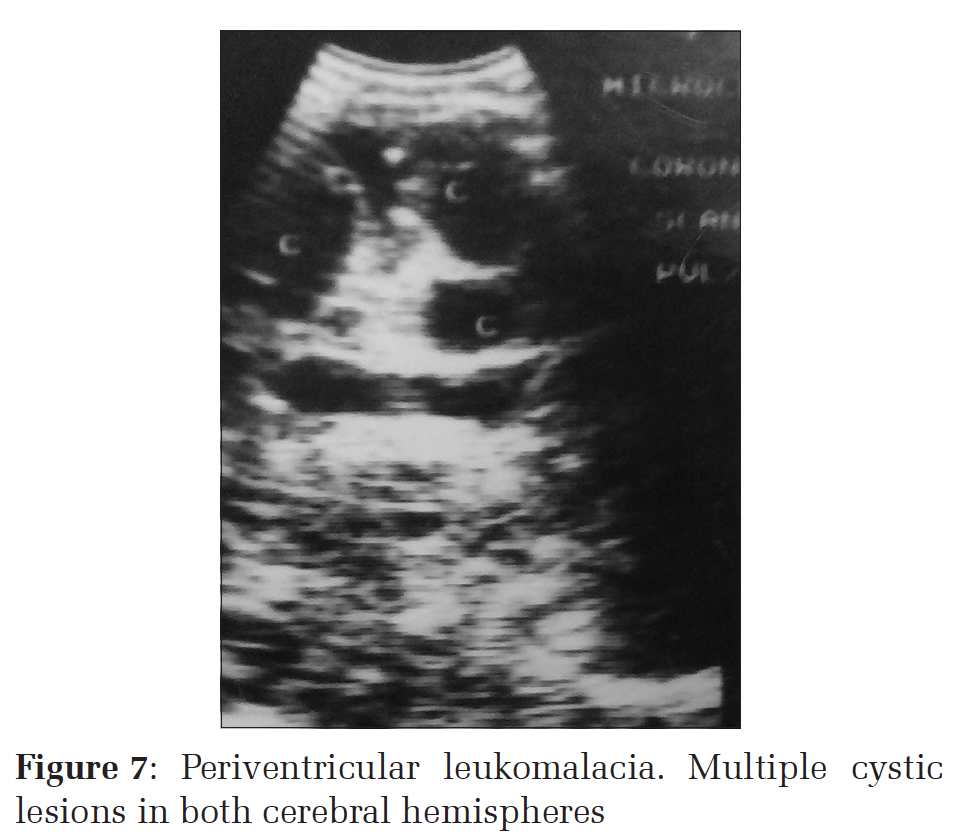
Results: Positive sonographic findings identified in 120 patients. Some patients showed more than one sonographic findings. 75% of preterm babies presented with intraventricular hemorrhage and on follow-up scans showed communicating hydrocephalus in 75% and 16% porencephalic cysts. In HIE, 74% had cerebral edema followed by periventricular echo densities. 10 cases of periventricular leukomalacia with 2-3 mm cystic lesions resulting in cerebral palsy. All infections presented with echogenic sulci or meningeal thickening in 38%. Hydrocephalus being the common sequelae in 48%. In congenital anomalies, hydrocephalus predominates the study in 54% with other associated anomalies such as Dandy–Walker malformation.
Conclusion: Neurosonography is a non-invasive, safe, cost effective and allows for the prediction of neurological development. It provides a clue to a wide range of pathology and spectrum of pathological imaging appearances encountered in neonates. It is an accurate and sensitive modality for early diagnosis and timely management.
KEY WORDS:Hypoxic-ischemic encephalopathy, hydrocephalus, intraventricular hemorrhage, meningitis, neurosonography, preterm, periventricular leukomalacia.
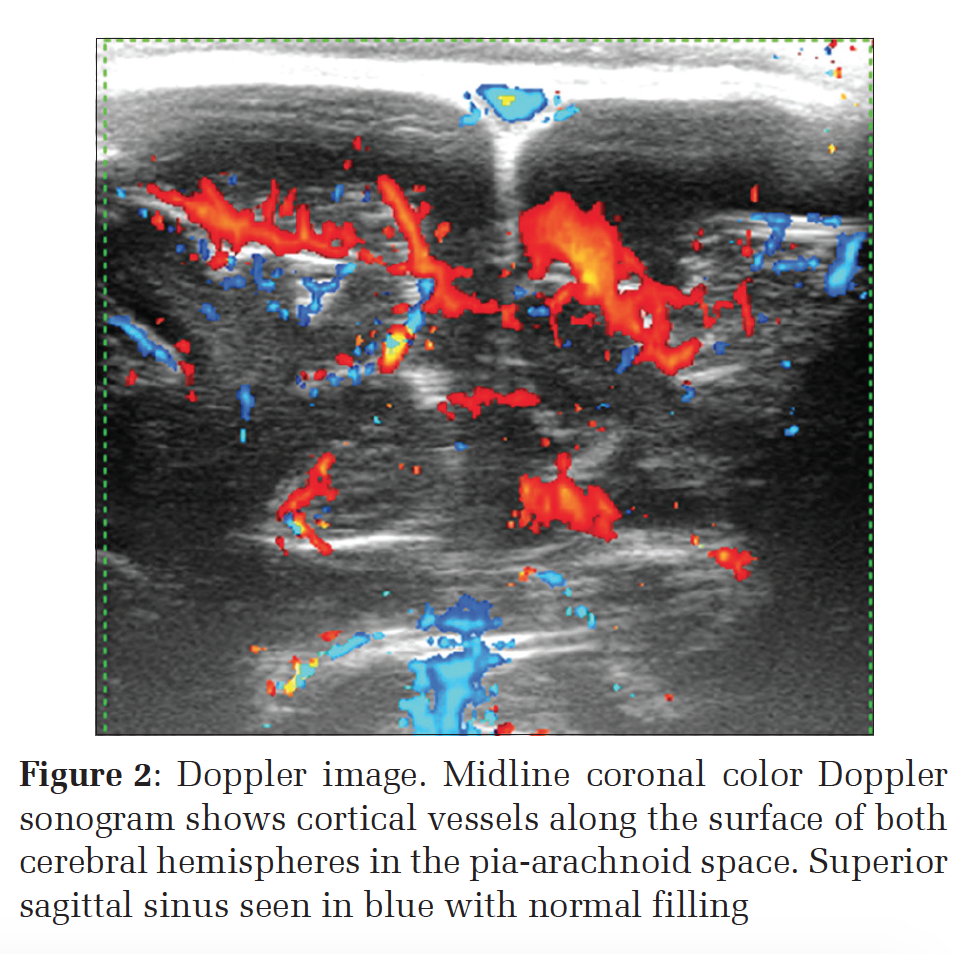
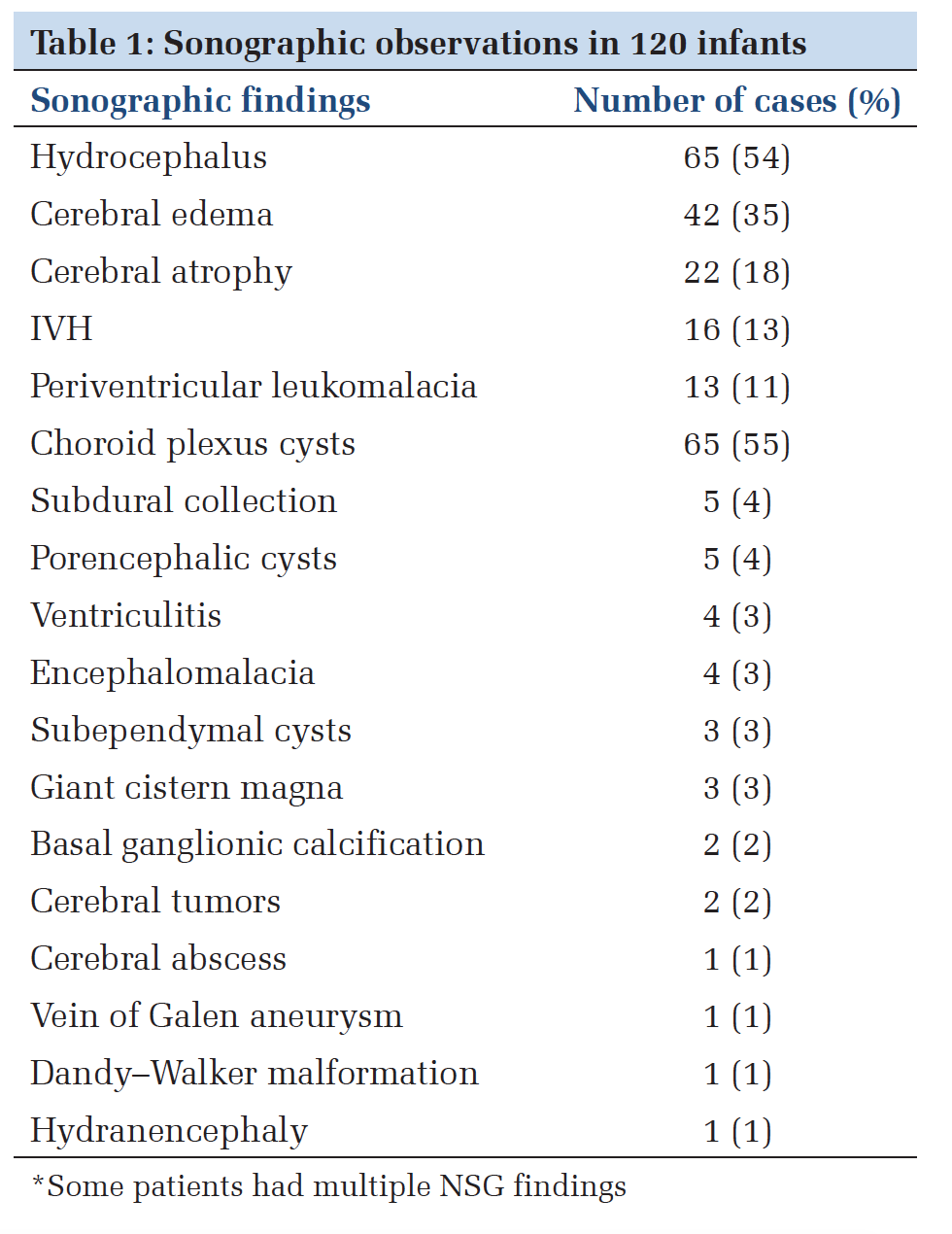
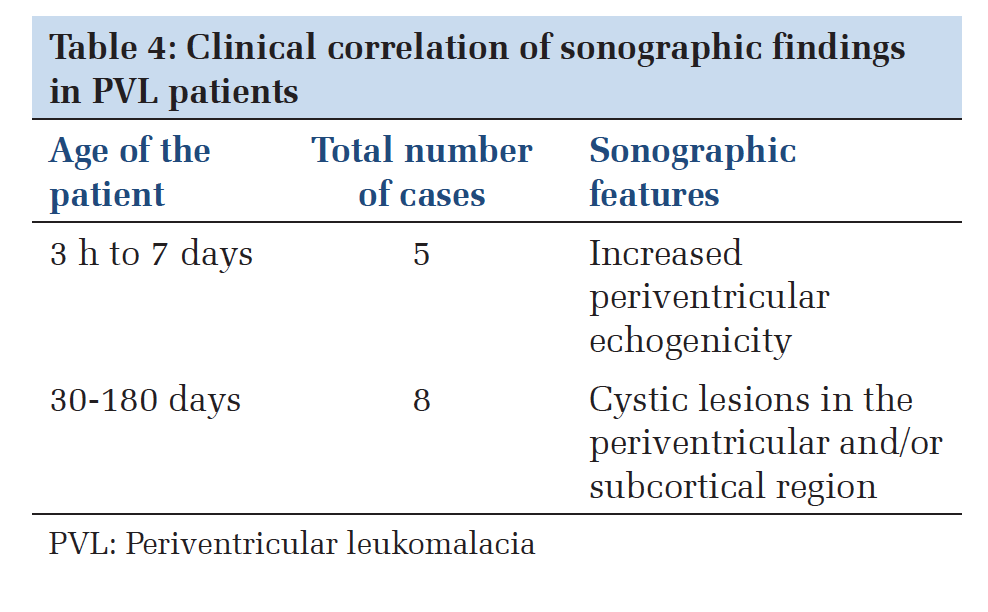
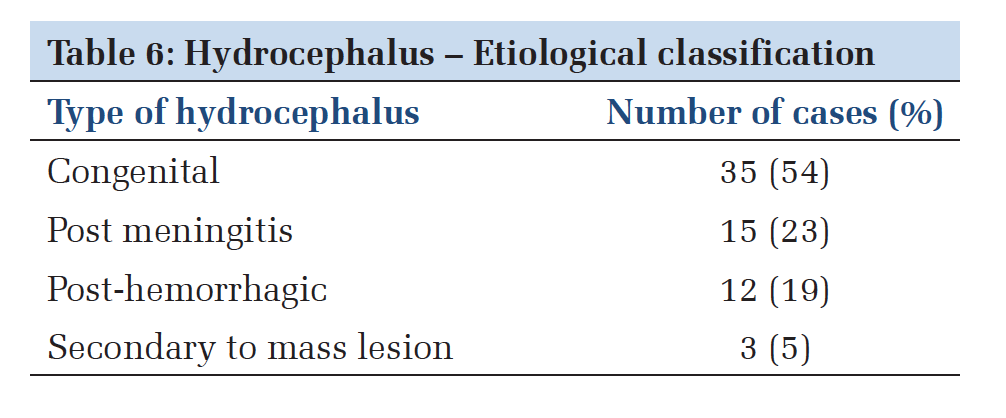
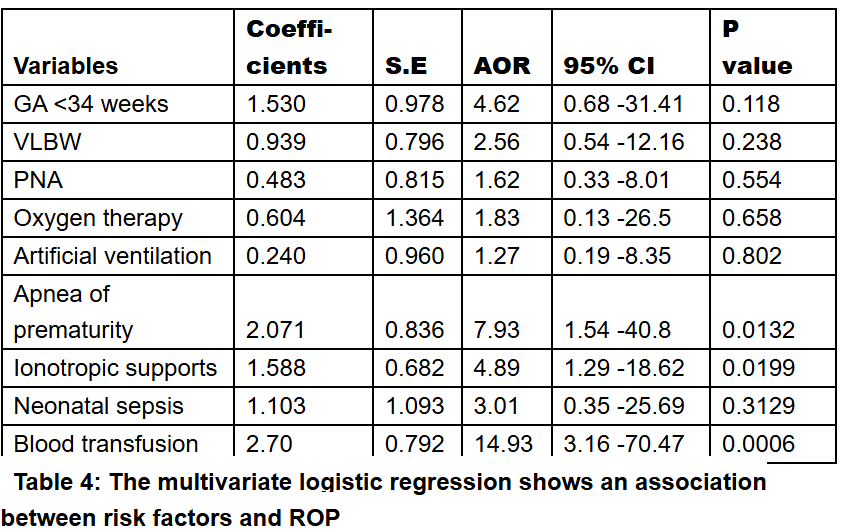
IntroductionNeurosonogram (NSG) is the only method able to image the neonatal brain at the bedside, which can be vital in the case of the critically ill infant. This investigation does not require sedation or specific monitoring easily reproducible and no ionizing radiation. Understanding echo texture of brain parenchyma and its content is essential to differentiate normal and abnormal areas. With modern high-end machines, there is improved resolution and it is more important than ever to be aware of the normal echogenicity of various anatomic structures in the brain.[1] Before 34 weeks of gestation Post-hemorrhagic hydrocephalus can be directly attributed to IVH; future handicap is best related with the extent of parenchymal damage. PVL is a form of ischemic white matter damage.[3] In preterm, the more common pattern is focal noncystic white matter injury or diffuse white matter gliosis. The infants < 30 weeks of gestation to undergo screening on ultrasound (US) at 7-14 days and a repeat US at 30-40 weeks. Beyond 34 weeks of gestation The US changes in hypoxic-ischemic encephalopathy (HIE) can be classified as peripheral and central.[4] An increased echogenicity of brain parenchyma, i.e. bright brain is fully developed by the 2nd-3rd day of life. The moderate to severe increase of parenchymal echogenicity has a high sensitivity (88%) for death or severe disability and can be an early predictor of permanent brain damage in asphyxiated infants.[5] By the 2nd-3rd day of life, the predictive value of the “bright brain“ phenomenon can be as high as 90-100%.[6] Long-lasting increase in parenchymal echogenicity (5-7 days and more) is a predictor of poor outcome [Figure 1].[6-8] Pathology unrelated to gestational age Infections Neoplasms Materials and MethodsIt is a retrospective study of 165 cases underwent transcranial sonography to evaluate intracranial pathology. US machines with color Doppler and with appropriate probes for neonatal head examination (5-15 MHz frequency) were used. Examination was performed according to a standardized protocol starting with gray-scale imaging via the anterior fontanels in the coronal and sagittal planes.[4,14,15] The presence of open fontanelle in the infant place major role in the ability to image the brain with US to obtain high-resolution real time images. Six to eight coronal images are obtained, beginning at the anterior frontal lobes and extending to the occipital lobes posterior to the lateral ventricle, i.e., trigone area.[16,17] The transducer is then rotated 90° and five sagittal images are obtained. Axial sections – with babies head in lateral position the probe is placed along the tempero parietal region to demonstrate lateral ventricular area. It gives a better view of the cerebellum and also useful for lateral ventricular size. Color Doppler images for arterial and venous structures were obtained for the screening of vascular structures. It is performed through the following four cranial windows (in addition to patent fontanelle or Burr holes) – transtemporal, transorbital, transforaminal, and submandibular. The most commonly used alternative windows include the posterior and mastoid fontanel to visualize occipital horns and infratentorial structures such as the cerebellum and surrounding anatomy.[18] Linear high-frequency transducers with Doppler were applied to obtain a coronal magnification view of the extra-axial fluid space and to differentiate collection versus atrophy [Figure 2]. As our study is largely dependent on gestational age, it is considered on three subdivisions: (1) Before 34 weeks (preterm), (2) after 34 weeks of gestation, and (3) pathology unrelated to gestation. US findings correlated with clinical situation and follow-up studies done after 2-12 weeks for complications and sequelae. Data underwent a statistical analysis and results were compared to available data in the literature. Data are presented as number and percent in tabular form. ResultsAmong 165 patients examined, 120 patients showed sonographic findings depending on their clinical situation which are listed in Table 1. 45 patients have normal sonograms. We had 12 cases as preterm in whom IVH was present in 75% of cases, and on follow-up, they developed communicating hydrocephalus in 75% of cases as frequent sequelae, followed by porencephalic cysts [Table 2]. A wide spectrum of sonographic abnormalities [Table 3] was observed in 31 cases of suspected central nervous system infections either in the form of pyogenic meningitis or tuberculous meningitis. Out of them, 5 had normal sonogram despite clinical and biochemical profile of pyogenic meningitis. In this study, it was observed that 35.48% of infant’s earliest sign is echogenic sulci and followed by other signs as per [Table 3]. The common sequelae after infection noted are hydrocephalus (48.38%). Out of 13 cases of PVL 13 patients of our study, 10 are full term and 3 were preterm. All cases had birth asphyxia. Sonographic features are shown in Table 4. In our study, among 50 patients of HIE, 80% showed changes of HIE, and among them, 74% had cerebral edema in both stages of in Edema in both HIE1 and HIE2 followed by other signs [Table 5]. Among congenital anomalies, the most common etiology is congenital hydrocephalus is most common congenital anomaly followed by postinfective etiology [Table 6].
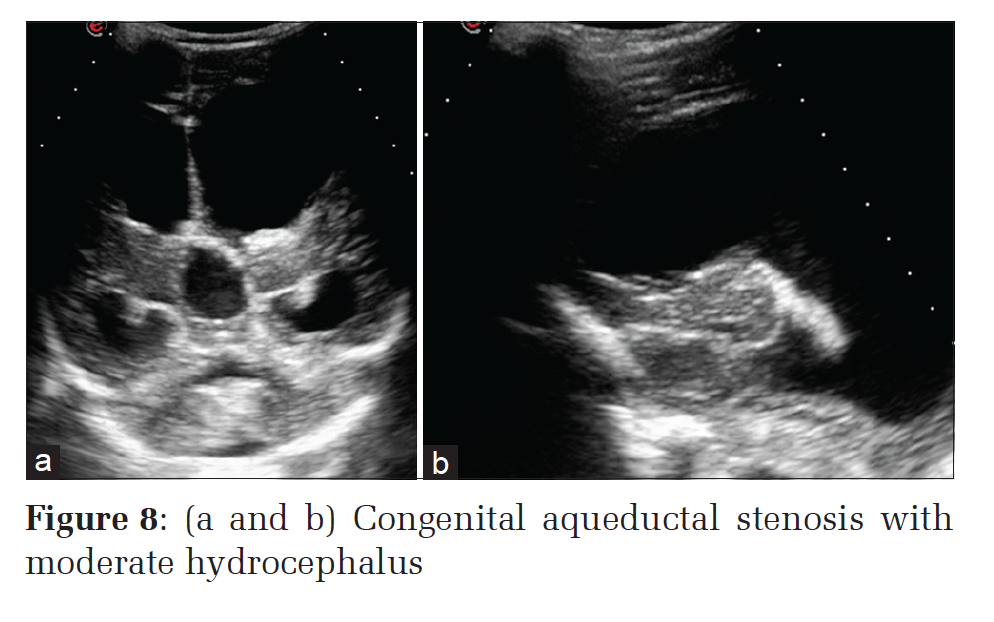
DiscussionOur study aims particularly in the view of efficacy of NSG, as it is increasingly considered as a basic first line technique in many neurological conditions in neonates and infants that significantly influence morbidity and mortality. The premature infants are now able to survive beyond perinatal period due to advanced life support system in neonatal intensive care units. It can be used as a simple screening tool in the exclusion of gross intracranial pathology. Before 34 weeks most frequently, ICH occurs in the 1st week of life, and 97% of the cases are detected by the transcranial US.[19] GM-IVH [Figures 3 and 4] is the most frequent neonatal ICH and the risk for GM-IVH decreases significantly after 32 weeks of gestation. On US intraparenchymal hemorrhage appears as unilateral well defined brightly echogenic area, dorsal, and lateral to the external angle of lateral ventricle. In our study, 4 patients had minor IVH. SAH appear as a focal area of increased echogenicity in two patients overlying both caudate nuclei and lateral walls of lateral ventricles in coronal plane. In the sagittal plane, it was seen lying in the caudothalamic groove [Figure 3]. The finding in other 2 patients with minor IVH. Hemorrhage is seen as low-level echoes within the occipital horns of lateral ventricles. Among 5 patients of with Grade 3, IVH presented as large echogenic material within dilated lateral ventricles, and ventricular cast formation noticed in 3 of them. In our series, intraparenchymal hemorrhage was unilateral in all 7 neonates with Grade 4 IVH. It was brightly echogenic and relatively well defined, the degree of brightness was comparable with that of choroid plexus. The intraparenchymal bleed was differentiated from focal edema by the degree of brightness and differentiation from hemorrhagic PVL was done by considering their topographic location and bilateral symmetric nature of PVL. Literature reviews and published studies correlated the degree of prematurity and the increased ICH risk.[20-22] It is generally accepted that the incidence and severity of the ICH are related to both gestational age and birth weight, occurring in 25-30% of patients born at < 32 weeks gestation, with < 1500 g. In previous studies, the intracranial hemorrhage prevalence in all gestational age preterms is reported much more higher between 40% and 45%.[23] Our study shows 75% which is much higher which is attributed for improved resolution with high-frequency probes. Among infections, pyogenic meningitis is more common pathology with sonographic signs of echogenic sulci [Figure 5] or meningeal thickening as earliest signs, due to intense inflammatory exudates which accumulate in the depth of fissures, sulci, particularly around pia and subarachnoid vessels seen in 26-83% of affected patients.[11,24] We detected gyral lesions in three infants with history of meningitis, one patient with features of ventriculitis and cerebral edema initially, followed by rounded well-defined sonolucent lesion with echogenic walls in fronto-parietal region after 4 weeks. The sonological diagnosis of the cerebral abscess was confirmed by CT scan, revealed streptococcus pneumonia on culture [Figure 6]. We had 15 cases of hydrocephalus with history of meningitis; out of them 6 patients had tuberculous meningitis, the other 9 had non-tuberculosis bacterial meningitis. The diagnosis of post-meningitis hydrocephalus was based on clinical data, cerebrospinal fluid analysis, and NSG. One of the serious complications of bacterial meningitis is abscess formation reported with a frequency of between 1% and 18% in newborns with meningitis.[25] Mortality rates are significant, and many of survivors develop neurological sequelae. It is 3% in our study. In our study, of 50 patients of HIE showed sonographic changes in 80%. Among them, 74% presented with cerebral edema which predominates the picture followed by other findings such as periventricular echo densities in 10%, focal parenchymal densities in 10%, followed by the sequelae porencephaly in 2%, and cystic encephalomalacia in 6%. The gray-scale scan missed disease in 2 cases and the application of Doppler is able to show diminished blood flow pattern with subtle disease in those cases indicating the application of Doppler is mandatory in clinically suspected cases with normal grayscale scans. Widening of interhemispheric fissure is another important finding we observed in 6 patients with, multifocal or diffuse damage to the brain, who developed cerebral atrophy on follow-up scans after 4-8 weeks. It is important to identify and note the severity, extent, site of brain damage and which requires MRI for further evaluation early clinical suspicion is crucial to prevent irreversible damage. Most of our cases on follow-up showed either cerebral atrophy or PVL. PVL In 13 patients of PVL of our study 10 are full term and 3 were preterm babies, all are born with birth asphyxia. On US 2-3 mm cystic lesions could be detected with high-frequency probes. They are present in both periventricular and sub cortical areas in full term babies and in periventricular area in preterm babies. In addition, 4 patients had widening of interhemispheric and ventriculomegaly suggestive of cerebral atrophy, which correlated with Grant and Schellinger[27] indicating that HIE affects entire brain parenchyma apart from localized infections. Cystic PVL is a predictor of cerebral palsy (CP). Pidcock et al. study show 26 patients with periventricular cysts developed with CP, out of 127 studied indicates periventricular echo densities without cysts have negative predictive value for CP.[28] A direct relationship between the presence of PVL and the severity of neurological sequels is described. We had only 2 cases with CP whose earlier scans showed cysts in the periventricular region more than 3 mm in diameter. At present, most of the congenital anomalies are detected in utero due to extensive antenatal US applications. MRI plays major part than NSG in infants to depict normal and abnormal variations. Congenital hydrocephalus predominates the picture in our study along with associated anomalies such as myelomeningocele, Chiari malformations, and Dandy–Walker variations. In general, hydrocephalus contributes to a large number of cases and needs follow-up by NSG. The extent of hydrocephalus, level of obstruction, and thickness of the cerebral mantle should be noted for subsequent follow-up. Biventricular and the bifrontal ratio are measured at the level of the foramen of Monroe for quantitative follow-up of hydrocephalus. In our study of 35 patients with congenital hydrocephalus, 19 had non-communicating type and aqueductal stenosis found in 13 patients with grossly dilated ventricular cavities [Figure 8a and b]. Aqueductal obstruction can be evaluated through the mastoid fontanels. Detection of aqueductal obstruction is 69% in our study. Distinguishing between obstructive versus non-obstructive hydrocephalus is important for neurosurgical consultation for prompt management. Serial follow-up of ventricular size by sonography helps in analyzing obstructive, progressive hydrocephalus, and also status postventriculoperitoneal (VP) shunts. Our study had 8 patients with post-VP shunt who presented with clinical deterioration and increasing head circumference. Displacement of shunt tube demonstrated in 5 patients. The other 3 patients had moderate to severe hydrocephalus with shunt tube in situ. We had 1 case of Dandy– Walker malformation in our study. The US findings are of large cystic lesion posterior to cerebellum with enlarged posterior fossa, dilated ventricular system with absent vermis, hypoplastic cerebellum, and diagnosis confirmed on CT scan. Tumors and vascular malformations may be identified by their classical appearance as in the cases of choroid plexus papilloma and vein of Galen aneurysm. Vein of Galen malformation in our study was confirmed by color Doppler and CT scan. |
ConclusionUltrasonography is operator dependent, and the quality of the study is intimately related to the skill and experience of the sonologist as well as their knowledge of the anatomy and pathology of the neonatal brain. Clinical application of this imaging method is extremely useful for premature neonates, particularly when NSG performed early will contribute with valuable data for a better therapeutic approach and neurological development of pediatric patients. Despite the advances in multislice computed tomography and MRI, NSG is the most commonly used first baseline modality for examining the newborn brain, considering growing economic pressure, and the low invasiveness as well as the easy availability of US that can easily be repeated at any time. Neonatal NSG still remains a mainstay of imaging in the neonatal brain. |
Subscribe now for latest articles and news.