Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.v10.i2.24.82
Year: 2024, Volume: 10, Issue: 2, Pages: 154-161
Original Article
Kunal Tewari1 , Akash Ray Mohapatra2 , Deepak Mishra3 , Om Bahadur Thapa2 , Jyotsna2
1Professor, Department of Anaesthesiology and Critical Care, Command Hospital (Southern Command), Pune,
2PG Trainee, Department of Anaesthesiology and Critical Care, Command Hospital (Southern Command), Pune,
3Assistant Professor, Department of Anaesthesiology and Critical Care, Command Hospital (Southern Command), Pune
Address for correspondence:
Kunal Tewari, Professor, Department of Anaesthesiology and Critical Care, Command Hospital (Southern Command), Pune.
Email: [email protected]
Received Date:19 March 2024, Accepted Date:30 May 2024, Published Date:17 June 2024
Background: Blood loss is often a major complication of neurosurgery; and adversely impacts postoperative outcomes. Primary objective of our study was to assess the effect of tranexamic acid (TXA) on total perioperative blood loss and the need for packed red blood cell (PRBC) transfusion in patients. Secondary objective was to assess and compare the effect of TXA on haemoglobin (Hb) , packed cell volume (PCV), coagulation profile, crystalloid and PRBC requirement, neurological outcomes; and the quality of surgical field peri-operatively. Materials and Methods: 60 adult patients, undergoing elective craniotomy for tumor resection were recruited. 30 patients each, received either a bolus of TXA , followed by an infusion (TXA group); or normal saline in the same dose (Placebo group). Crystalloid and PRBC transfusion, blood loss, Hb, PCV, platelet count, fibrinogen levels, international normalized ratio were recorded. Mean intensive care unit (ICU) stay and Glasgow Outcome Extended (GOSE) score were also measured. Results: There was no significant difference in blood loss, PRBC requirement, Hb, PCV, fibrinogen levels , INR, duration of ICU stay or the quality of the operative field; between the TXA and placebo groups. GOSE scores were better and platelet count decrease was significantly higher in the TXA group. Conclusion: Low-dose TXA did not significantly reduce blood loss or improve outcomes in patients undergoing intracranial tumor resection. GOSE score was better; and the platelet decrease post- operatively was significantly higher in the TXA group.
Keywords: Intracranial Tumours, Tranexamic Acid ( TXA), Glasgow Outcome Extended (GOSE) Score
Brain tumours are a diverse category of tumours that originate from cells inside the central nervous system. With an overall survival rate of little more than 35 percent after five-year’s follow-up, malignant primary brain tumours continue to rank among the most challenging tumours to treat 1. The intracranial surgery is a necessary part of the surgical treatment for the brain tumours. Because these tumours induce local tissue plasminogen activator and cause fibrinolysis, the surgical procedure is frequently associated with a significant amount of blood loss 2. Intraoperative blood loss may be significant, which can result in hemodynamic instability and call for the administration of significant blood transfusions. This is often linked with an increase in postoperative morbidity and death. It is well understood that intraoperative haemorrhage in neurosurgery, more especially during the excision of cerebral meningioma, often necessitates the transfusion of a significant amount of blood and blood products 3.
Generally, it is agreed that intraoperative blood loss is one of the most serious problems that may arise during neurosurgical procedures. This is because it has a direct bearing on the postoperative morbidity and mortality of the patients 4. A significant loss of blood may result in hemodynamic instability as well as coagulopathy; as a result, blood conservation/salvage methods should be used whenever it is possible to do so 5. Minimising the amount of blood lost during tumour excision may successfully help ensure that the whole tumour is removed.
The considerable intraoperative bleeding that frequently occurs requires, in addition to the infusion of a large volume of crystalloids, the replacement of the lost blood volume with a large number of blood units and blood products. Allogeneic packed red blood cell (PRBC) transfusion is associated with a number of well-known adverse effects. These effects can range from relatively mild allergic reactions, acidosis, citrate toxicity, and hypocalcemia to severe anaphylactic reactions, transfusion-associated lung injury, infectious disease transmission, circulatory overload, and immunosuppression 6. In addition, it has been shown that giving a significant quantity of replacement fluids in the form of PRBCs or crystalloids may dilute the coagulation factors, which can lead to a malfunction in the coagulation process and further increase the amount of bleeding that occurs during surgical procedures 7.
Therefore, it is very necessary to have a plan that is geared towards minimising the significance of intraoperative blood loss and the need for the transfusion of unstable blood products. In recent years, there has been a resurgence of interest in the use of tranexamic acid (TXA) in a variety of neurosurgical procedures, including those involving trauma, subarachnoid haemorrhage, tumour excision, and spine operations. Recent research conducted on adults demonstrates its efficacy in lowering the amount of blood lost, the need for blood transfusions, and the development of improved haemostasis following brain tumour removal; all with few adverse effects 8.
TXA (an antifibrinolytic drug), also known as trans-4 aminomethyl cyclohexane carboxylic acid; prevents the conversion of inactive plasminogen into the active proteolytic enzyme plasmin by inhibiting the high affinity lysine binding site of plasminogen in a manner that is competitive 9. As a result, plasmin is prevented from attaching to fibrinogen and fibrin structures after the development of a clot. Although studies evaluating the impact of TXA on the intraoperative blood loss during intracranial surgeries of tumours are available from India, they were conducted among different study population and setting.
Our aim was to conduct a prospective randomized control trial to find out the outcome in terms of blood loss in patients receiving tranexamic acid intraoperatively for intracranial neoplasm surgeries. Primary objective of the study was to assess the effect of TXA on total perioperative blood loss and the need for PRBC transfusion in patients undergoing craniotomy for tumor excision. Secondary objective was to assess and compare the effect of TXA on change in haemoglobin (Hb) and packed cell volume (PCV) levels postoperatively, compare coagulation profile in the perioperative period, requirement of crystalloid and PRBC intraoperatively, neurological outcomes; and the quality of surgical field.
This is a double blinded prospective randomized control trial, conducted at our centre, a tertiary care hospital with large neurosciences centre; from Oct 22 to Apr 24. The project was cleared by Institutional Ethics Committee of the institute, IEC/Anaes/01/2022 dated 03 Oct 22. All adult patients, aged 18-65 years who provided consent; who did not have any associated severe co- morbid conditions, and were scheduled to undergo craniotomy for intracranial tumor excision, were included in the study. Patients who denied consent, had past history of venous thromboembolism, were on current treatment with oral anticoagulant or antiplatelet drugs, those with abnormal coagulation profile, liver function tests, renal function tests, were excluded from the study. Pregnant or lactating mothers, patients with history of allergy to TXA; and those who were planned for pre-operative embolization; were also excluded from the study. Based on a previous study by Rebai et al, and assuming alpha as 5% and power of 90%; the minimum required sample size of 20 was calculated 3. We included a minimum of 30 patients in each group.
All the patients listed for elective intracranial neoplasm surgeries were assessed for eligibility and written informed consent was obtained from them. Consent was obtained from next of kin, if the patient was unable to provide the same. Patients were randomized into two groups; group T (TXA group) and group P (Placebo group) using block randomization technique and allocation was concealed. In the operation theatre, standard monitoring mandated as per American society of Anaesthesiologists (ASA) ; electrocardiogram (ECG), non-invasive blood pressure (NIBP), and oxygen saturation (SpO2) was applied. After recording the baseline vital parameters, standard anaesthesia technique was used for induction and maintenance of anaesthesia as mentioned in study proforma for both the study groups. Invasive hemodynamic monitoring with central venous catheter (CVC) and intra-arterial blood pressure (IABP) was established, after induction.
Enrolled patients were administered either TXA or NS in 50 ml syringe, as per protocol of study (Figure 1). Both the syringes were labelled as ‘ Test Drug’, so that the attending anaesthesiologist as well as operating surgeon were not aware of the contents; and were blinded to the intervention. The anaesthesiologist/ trainee who prepared the drugs was not involved in the study at all. Intraoperatively, heart rate (HR), SpO2, end tidal CO2 (EtCO2), NIBP, temperature, IABP, CVP, minimum alveolar concentration (MAC), and fluid intake/ output were continuously monitored. Hb, PCV, platelet count, fibrinogen levels and international normalized ratio (INR) were measured after induction (taken as pre-operative value), and at 90 mins after skin closure (taken as post-operative values). Quality of surgical field was assessed by single experienced neurosurgeon and the same was evaluated using a five point Likert scale 10.
Intravenous fluid administration consisted of isotonic crystalloid solutions. Transfusion of blood and blood products was made at the discretion of the attending anaesthesiologist. The haemostatic therapy was guided by ASA task force on blood transfusion 11. Intraoperatively, fluid and ventilatory management was guided by invasive hemodynamic monitoring, urine output and regular arterial blood gas analysis (ABG). Transfusion trigger for PRBCs transfusion was a Hb concentration ≤8 g/dl. The amount of transfused blood products was recorded.
On completion of skin suturing, administration of tranexamic acid or saline in the respective assigned group was stopped. The decision for endotracheal extubation on completion of surgery in the operation theatre or elective mechanical ventilation in the postoperative period was taken by the attending anaesthesiologist based on amount of blood loss, hemodynamic parameters, intraoperative brain condition, brain handling and preoperative neurological status. Blood loss estimation in all the cases was done by the principal investigator by subtracting the amount of irrigation fluid from suction aspirate and visual assessment of the soaked sponges, cotton pledges, surgical drapes and area at the operating end during the intraoperative period. Postoperative blood loss was measured as blood volume collected by suction drains at 48 hours. Total blood loss was calculated as the sum of intraoperative and postoperative blood loss.
All patients were shifted to neurosurgical intensive care unit (ICU) for postoperative monitoring and care. Computed tomography (CT) scan was done for all patients to assess haematoma formation or any other complication like hydrocephalus. The duration of ICU stay was recorded. Patient’s neurological status at the time of discharge from the hospital was graded as per the Glasgow Outcome Scale Extended (GOSE) score 12. ICU stay and GOSE score were taken as postoperative outcome measures.
All data were entered in an MS Excel sheet. Analysis was undertaken using statistical package for social sciences (SPSS) software, version 26.0. Categorical variables were expressed in the frequencies and percentages. Mean (SD) and Median (IQR) for continuous variables were calculated. Chi-square test was applied to test the significance between categorical variables and the treatment group. Continuous variables were found to be non-normally distributed. Mann-Whitney test was applied to test the significance in difference of continuous variables between the treatment groups. p value less than 0.05 was taken as statistical significance. Statistical analysis was performed by expert bio- statisticians.

|
Variables |
Group T, n (%) |
Group P, n (%) |
p value |
|
Sex |
|
|
1.000 |
|
Male |
16 (53.3%) |
15 (50%) |
|
|
Female |
14 (46.7%) |
15 (50%) |
|
|
ASA Grade |
|
|
0.855 |
|
I |
3 (10% ) |
2 (6.7%) |
|
|
II |
18 (60% ) |
20 (66.7%) |
|
|
III |
9 (30% ) |
8 (26.7%) |
|
|
Tumor location |
|
|
0.426 |
|
Infratentorial |
13 (43.3%) |
10 (33.3%) |
|
|
Supratentorial |
17 (56.7%) |
20 (66.7%) |
|
|
Tumor pathology |
|
|
1.000 |
|
Astrocytoma |
5 (16.7%) |
5 (16.7%) |
|
|
Glioma |
7 (23.3%) |
8 (26.7%) |
|
|
Meningioma |
12 (40%) |
11 (36.7%) |
|
|
Pituitary adenoma |
2 (6.7%) |
1 (3.3%) |
|
|
Schwannoma |
4 (6.7%) |
5 (16.7%) |
Group T: Tranexamic acid Group, Group P: Placebo Group, ASA: American Society of Anaesthesiologists
|
Variables |
Group T |
Group P |
p value |
|
|
Age (yr) |
Mean (SD) |
54.17 (14.37) |
52.13 (12.64) |
0.428 |
|
Median (IQR) |
53.5 (48, 65) |
52 (46.75,62) |
||
|
Body mass index (kg/m 2 ) |
Mean (SD) |
23.83 (3.26) |
23.67 (4.48) |
0.484 |
|
Median (IQR) |
23 (21,26.25) |
23 (21,25) |
||
Group T= Tranexamic acid Group, Group P= Placebo Group, SD: Standard Deviation, IQR: Interquartile Range
|
|
Group T |
Group P |
|
||
|
Variables |
Mean (SD) |
Median (IQR) |
Mean (SD) |
Median (IQR) |
p value |
|
Blood loss (ml) |
433.33 (266.63) |
300.00 (250,725) |
421.67 (265.45) |
350.00 (150,750) |
0.444 |
|
PRBC transfused ( ml) |
97.00 (151.50) |
0.00 (0,286.25) |
106.17 (143.85) |
0.00 (0,265) |
0.853 |
|
Hb decrease post- operatively ( mg/dl) |
0.74 ( 0.24) |
0.70 (0.6,0.925) |
0.66 (0.35) |
0.55 (0.4,0.9) |
0.131 |
|
PCV decrease post- operatively |
2.07 ( 0.24) |
2.00 (1.775,2.2) |
1.96 (1.28) |
1.55 (1,2.525) |
0.086 |
|
Platelet count decrease post- operatively ( x 103/ ml) |
24.03 (19.94) |
18.00(3,42.25) |
9.23 (19.29) |
7 (6,18) |
0.019 |
|
Fibrinogen increase post- operatively ( mg/dl) |
-12.17 (36.16) |
-14.00 (-48,25.25) |
-23.63 (37.70) |
-23.00 (-63,-10) |
0.193 |
|
INR decrease post- operatively |
0.04 (0.09) |
0.04 (0.01,0.1) |
0.10 (0.13) |
0.10 (0.015, 0.1925) |
0.056 |
|
Crystalloids ( ml) |
3226.67 (560.13) |
3000.00 (2800,3450) |
3026.67 (725.37) |
3000.00 (2650,3425) |
0.297 |
|
Urine output ( ml) |
1158.33 (214.19) |
1100.00 (1000,1325) |
1260.00 (335.13) |
1200.00 (937.5,1600) |
0.359 |
|
ICU stay ( days) |
3.77 (2.66) |
3.00 (2,4) |
4.17 (2.02) |
3.00 (2,6.25) |
0.171 |
|
GOSE score ( out of 8) |
5.80 (0.81) |
6.00 (5,6) |
5.10 (1.49) |
5.00 (5,6) |
0.037 |
|
Quality of surgical field (out of 5) |
3.83 ( 0.91) |
3.5 (3,5) |
3.77 ( 0.68) |
4 (3,4) |
0.937 |
Group T= Tranexamic acid Group, Group P= Placebo Group, PRBC: Packed Red Blood Cell, Hb : Hemoglobin, PCV: Packed Cell Volume, INR: International Normalized Ratio, GOSE: Glasgow Outcome Scale Extended, ICU: Intensive Care Unit, SD: Standard Deviation, IQR: Interquartile Range
The demographic variables (sex, ASA grade, tumor location and pathology, age and body mass index) were evenly distributed amongst both the groups (Table 1, Table 2). Majority of the tumors were meningioma in origin and the location was supratentorial. The quantity of crystalloids infused and urine output was comparable in both the groups.
Patients enrolled in both groups were followed up in the post-operative period and were analysed for difference in multiple variables (Table 3). When compared to baseline values, post- operative change in haemoglobin , fibrinogen and INR, did not demonstrate any statistical significance. Mean intra- operative blood loss, pRBC transfused, crystalloids transfused, and urine output did not have any statistically significant difference amongst both the groups. There was statistically significant difference in platelet count reduction postoperatively in Group T, when compared to Group P (mean: 24033.33 ml vs mean: 9233.33 ml, p value: 0.019). Mean GOSE score of the patients in Group T was higher than Group P, and statistically significant (mean: 5.8 vs mean: 5.1, p value: 0.037). Difference in the duration of ICU stay, and mean quality of surgical field for the patients (as assessed by blinded neurosurgeon), in both the was not statistically significant; when compared amongst the groups.
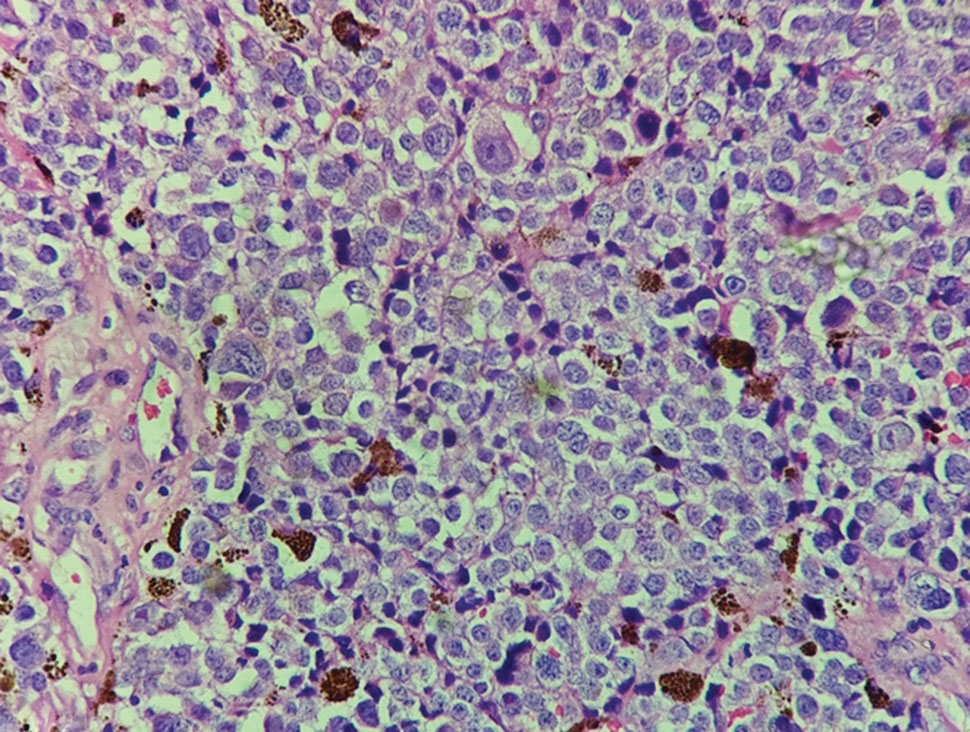
Resection of brain tumors is linked to higher blood loss and a notable rise in intravascular disseminated coagulopathy incidence. Coagulopathy during tumor removal is linked to unfavourable outcomes. Opting for transfusions during neurosurgical procedures can enhance oxygen delivery but also heightens risks like blood infections, hemolysis, lung damage, and weakened immune response 13. Thus, strategies to prevent the blood loss and the transfusion requirement which in turn reduces the adverse outcomes in these surgeries are under study across the globe. The present study assessed the role of low-dose tranexamic acid in reducing intra-op blood loss among 30 intracranial neoplasm patients and compared it with a placebo group of 30 patients at a tertiary care institute of central India.
Although in the current study, both the tranexamic acid and placebo group included meningioma (40% and 36.7%) as the most common intracranial condition, others such as glioma (23.3%-26.7%), astrocytoma (16.7%) and schwannoma (13.3%-16.7%) also had considerable incidence; and no statistically significant difference was observed amongst the pathologies. Batul et al included 60 patients and Vel et al did his research on 100 patients who underwent neurosurgery (craniotomy) for tumor excision; and observed results similar to our study 13, 14. However, most of the similar studies in the past were undertaken exclusively among meningioma patients. Hooda et al undertook a similar study but only among the 60 intracranial meningioma patients 15, Ravi et al included 30 patients with intracranial meningioma 10, and Rebai et al conducted a study among 91 intracranial meningioma patients 3.
The mean age of the patients in the current study among the tranexamic acid and placebo groups was 54.17 years and 52.13 years, respectively. Hooda et al and Vel et al included relatively younger patients in their study, with a mean age of 39.3 years and 40.42 in Tranexamic acid and 41.6 and 39.78 years in placebo group 14, 15.
The majority of the patients in both TXA and placebo groups had supratentorial tumour location (56.7% and 66.7%), respectively, in the present study. Hooda et al and Rebai et al reported a majority of the meningiomas among their patients in the convexity (26.7% to 30% and 43.6% to 48.8%) 3, 15.
In the current study, the mean blood loss of the patients in TXA and placebo group were 433.33 and 421.67 ml, respectively, with no statistically significant difference between the groups. In contrast, Hooda et al reported a significantly higher amount of blood loss in the placebo group (mean: 1124 ml) than the TXA group (mean:830 ml) 15. This might be due to the difference in the study population since their study included only meningioma patients. Rebai et al, Batul et al, Vel et al and Ravi et al also reported a significantly lower volume of blood loss among the TXA group (mean: 283 ml, 332.3 ml, 817 ml and 393.4 ml, respectively) than the placebo group (mean=576 ml, 576.7 ml, 1084 ml and 1150 ml, respectively) 3, 13, 14. Thakkar et al also reported a reduction in blood loss due to TXA in the posterior fossa tumors (PFT) resection in children 8. Two meta-analyses have reported the utility of the TXA in reducing blood loss among meningioma surgery patients 16, 17, while Prastikarunia et al reported the same desirable effect of TXA in all brain tumor surgeries 18.
Conventionally, the removal of intracranial meningiomas is recognized for causing substantial blood loss, necessitating extensive allogeneic transfusions of blood and blood products. This phenomenon is attributed to various factors, including the distinctive blood supply of meningiomas from meningeal vessels, the parasitic nature of pial vasculature, challenges posed by the vascular supply of skull base meningiomas, obscured surgical planes in large tumors with significant peritumoral edema, encasement of major cerebral arteries by the meningioma, involvement of dural venous sinuses by the tumor, and invasion of the scalp and calvaria along with associated feeders 19.
In line with the blood loss, the mean pRBC transfused for the patients in TXA and placebo group were 97 and 106.17 ml, respectively, with no statistically significant difference between the groups in our study. Although Hooda et al also reported a statistically similar pRBC usage among the TXA (mean=554 ml) and placebo group (mean=645 ml), the volume transfused was much higher in comparison to our study in either of the patient groups 15. In the present study, urine output for the TXA and placebo group patients were 1158.33 and 1260.00 ml, respectively, with no statistically significant difference between the groups. This is similar to the findings of Vel et al. 14.
While the preoperative mean Hb was significantly higher among the TXA group (mean:13.67 mg/dl) than the placebo group (mean: 12.58 mg/dl, p value: 0.018) in our study, no such difference was present among the two groups of patients in most of the previous studies 3, 14, 15. No significant difference in the mean change in Hb following surgery was observed in our study, while Batul et al reported a significantly higher drop in Hb among the placebo group than the Tranexamic acid group 13. The mean preoperative fibrinogen levels of the patients in TXA and placebo group were 236.2 mg/dl and 221.27 mg/dl respectively, with significant difference between the groups in our study, which is in line with the findings of Rebai et al. 3 While the post-op mean Hb was significantly higher among the TXA group (mean:12.94 mg/dl) than the placebo group (mean:11.91 mg/dl, p=0.027); no significant difference in the platelet count and fibrinogen in the post-op period was found between the two groups in our study. While Rebai et al. reverberated our findings in the platelet counts, fibrinogen levels were significantly higher among the TXA group than the placebo group. 3 In contrast, Ravi et al reported significantly higher post-op fibrinogen and platelet levels in the Tranexamic acid group than the placebo group 10.
The mean volume of crystalloids given for the patients in TXA and placebo group were demonstrated no statistically significant difference. This is in line with the findings of Ravi et al who also reported similar overall IV fluid administration between the two groups 10. Hooda et al reported a higher level of crystalloids administration in both TXA (mean=4575 ml) and placebo group (mean:4758 ml) 15. The duration of ICU stay for the patients in the TXA group (mean: 3.77 days) and placebo group (mean: 4.17 days) were statistically similar. GOSE score of the patients in TXA (mean: 5.8) was significantly higher than the placebo group (mean: 5.1), while no such difference was reported in the studies by Hooda et al and Rebai et al. 3, 15. The mean quality of the surgical field for the patients in our study among the TXA and placebo group had no statistically significant difference; while Ravi et al reported a significant difference in the quality of surgical field score in the Tranexamic acid group (median: 4) than the placebo group (median:2). 10.
However, our study had certain inherent limitations. As the study was undertaken from a single institute, external validity of the findings are limited. In each case, the histology of the tumor and the extent of tumor resection were not specifically documented. Further, the attending anesthesiologist's subjective assessment of blood loss may have led to an underestimation of the amount of blood lost onto surgical gowns, drapes, and pledgets.
TXA administration did not significantly impact blood loss and blood product transfusion. However, GOSE score was better, and the platelet decrease post- operatively was significantly higher in the TXA group. The present study included patients with major intracranial neoplasms, which increases the applicability of its findings to them. TXA usage may be recommended for the intracranial tumor resection, as per the treating team’s mutual decision, since only a limited utility has been observed in the present settings. Further, multi-centric studies with larger sample size need to be conducted to improve the external validity of our findings.
Subscribe now for latest articles and news.