Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.v11.i2.24.396
Year: 2025, Volume: 11, Issue: 2, Pages: 167-171
Original Article
Akanksha1 , Deepti Pruthvi2 , P Shashikala3
1Postgraduate, S. S. institute of Medical Sciences & Research Centre, Davangere, Karnataka, India,
2Professor, S. S. institute of Medical Sciences & Research Centre, Davangere, Karnataka, India,
3Professor and HOD of Pathology, S. S. institute of Medical Sciences & Research Centre, Davangere, Karnataka, India
Address for correspondence:
Akanksha, Postgraduate, S. S. institute of Medical Sciences & Research Centre, Davangere, Karnataka, India.
E-mail: [email protected]
Received Date:23 November 2024, Accepted Date:23 February 2025, Published Date:16 June 2025
Introduction: Histopathology is the foremost diagnostic method for numerous lesions, utilising biopsies to pinpoint diseases precisely via microscopic scrutiny. It establishes the diagnostic benchmark, influencing prognosis and treatment planning. Initial incomplete sectioning leads to errors; deeper sections enhance minor biopsy diagnosis. Laboratories commonly adopt deeper sectioning to refine results, particularly with limited small biopsy specimens. Objectives: To evaluate the prevalence of deeper sections required for definitive diagnoses in small biopsies and to analyse which anatomical sites are associated with a higher frequency of these requests. Materials and Methods: In a 6-month study at a tertiary care hospital, 106 small biopsy cases were examined to compare initial histopathology with deeper sections, assessing their impact on final diagnoses. Results: Out of 106 cases, 36 biopsies (34%) were analyzed. Deeper sections were frequently requested from samples received from Obstetrics and Gynaecology (33%) and least from Pulmonology (5%). 4 cases (11.2%) needed deeper sections due to inadequate initial samples. In 28 cases (77%), deeper sections were used to confirm or clarify diagnoses; of these, 13 (46.4%) revealed new pathology, 13 (46.4%) upheld initial findings, and 2 cases (7.2%) required diagnosis changes. 4 cases (11.2%) remained inconclusive, and 2 (5.6%) had tissue loss. Conclusions: Deeper sections significantly impact the ultimate diagnosis. Therefore, regardless of the lesion's site, consistently employing deeper sections is universally advised. This practice serves to surmount the constraints posed by the initial histopathological characteristics of small biopsies. Balancing this need with additional time, cost, and patient care effects is crucial.
Keywords: Biopsy, Histopathological examination, Deeper sections, Diagnosis
A biopsy involves retrieving tissue from a living body for microscopic scrutiny by a pathologist. Thorough histopathological analysis of biopsied tissue is the gold standard for diagnosing various conditions, encompassing malignancies, inflammation, and infections.1 Small biopsy samples, typically a few millimetres to centimetres in size, require no dissection and are directly embedded, processed and sectioned.1, 2 The process involves various sectioning techniques—serial sections, step sections, deeper sections, retrospective and prospective step sections—to enhance diagnostic accuracy by accessing tissue at different depths.2 Pathologists may examine these tissues at various levels for comprehensive analysis, even seeking deeper sections to enhance diagnostic precision.1 While standards aren't firmly established, practices typically involve multiple deeper sections at intervals to ensure thorough examination. The balance between diagnostic accuracy and practical considerations, like time and cost, drives the approach toward deeper sectioning. This study aims to evaluate the frequency of deeper section requests contributing to definitive diagnoses in small biopsies and to analyze which anatomical sites commonly required deeper sections for accurate assessment.
This observational study was conducted at the Department of Pathology in a tertiary care hospital. It encompassed all 106 small biopsies reported in six months. Specimens from all organ systems which required deeper sections were included. Slides with deeper levels for improved or specialized staining were excluded. Formalin-fixed small biopsy specimens underwent processing and embedding before being sectioned into 3–5μm sections for Hematoxylin and Eosin staining.1 The histopathologist examined the slides under a light microscope. In our study, a 2-step sectioning method was routinely followed. To minimise bias, we adhered to various operational definitions for deeper sections, as practiced both institutionally and globally. Deeper sections were defined as those exceeding 5µm in thickness and included the following categories 1:
Step Cut (SC): Sections obtained after every alternate section.
2-Step Section (2SC): Sections obtained after every two sections.
3-Step Section (3SC): Sections obtained after every third section.
Slides labelled “deeper sections” and the corresponding “initial sections” were reviewed. The rationales for requesting deeper sections were categorized into non-diagnostic superficial sections, presence for additional information and misleading diagnosis, although the study did not explicitly address the number of required deeper levels for diagnosis.
A total of 106 small biopsy specimens from different clinical sites were included in the study. Deeper sections were performed in 36 cases, accounting for 33.9% of the total. The majority of these cases were from the Obstetrics and Gynaecology (OBG) department, comprising 12 cases (33.3%), which primarily included biopsy samples from the cervix and endometrium. This was followed by the Surgery and ENT departments, each contributing 9 cases (25%) that included a variety of biopsies, such as those from lymph nodes, the prostate, finger, maxillary sinuses, and vocal cords. Dermatology accounted for 4 cases (11.2%) involving biopsies from sites like the nose and forehead. Other departments collectively contributed 2 cases (5.5%).
Thirty-six (33.9%) cases were advised for deeper sections out of 106 cases. Out of the 36 cases, the diagnosis was revised in 4 (11.2%) as the initial sections were superficial & non-diagnostic, representing only a part of the biopsy. Deeper levels in 28 cases (77.7%) were taken to look for additional histological features, even though diagnosis was possible from the initial slides. This was to improve diagnostic sensitivity or confirm the initial diagnosis using the initial slide. Out of these 28 cases, 13 cases (46.4%) disclosed additional pathological findings, i.e, from mild to severe dysplasia in the buccal mucosa, haemorrhage and insignificant findings to polyp in cervical biopsy & granulomas in the tendon sheath of the little finger, from metaplasia to carcinoma. In contrast, the other 13 cases (46.4%) showed the same histological features in deeper sections. Two cases (7.2%) required a revised diagnosis due to misleading initial sections. In 4 cases (11.2%) a definitive diagnosis remained elusive despite deeper sections.
Overall, deeper sections enhanced the diagnosis in 17 cases (47.2%), with 4 cases (11.2%) revealing new features that changed the initial diagnosis. In 13 cases (36.1%), the histological features remained unchanged. Additionally, 2 cases (5.5%) showed tissue loss compared to the original sections (Table 1).
|
Categories |
Frequency |
|
Nondiagnostic superficial sections |
04 (11.2%) |
|
Misleading diagnosis |
02 (5.6%) |
|
Additional features |
13 (36.1%) |
|
Same as initial sections |
13 (36.1%) |
|
No diagnosis possible |
04 (11.2%) |
In one case where the initial slides of buccal mucosa biopsy displayed only signs of squamous metaplasia (Figure 1 A), further examination of deeper sections (Figure 1 B) revealed the presence of infiltrating moderately differentiated squamous cell carcinoma characteristics.

Ulcer biopsy from left little finger. The initial section (Figure 2 A) shows inflammatory infiltration of lymphocytes & plasma cells only. Deeper section (Figure 2 B) shows multiple Langhans giant cells in the upper dermis & granulomas in the deeper dermis (H&E stain 10X).

The punch biopsy from the nose revealed tumor nests of basaloid cells more distinctly in the deeper sections compared to the initial sections (Figure 3 A & B).

Routine small biopsy reports may be ready at the earliest within 2-3 days after the sample is received in the laboratory. False negative diagnosis in pathology is the most common consequence of sampling error caused by incomplete sectioning through the tissue block. No standardized approach for sectioning small biopsy specimens have been discovered so far. There are differences of opinion about the deeper sectioning methods to obtain optimal diagnostic information. As histopathologic assessment is subject to sampling error, many institutions and laboratories 'preorder' deeper sections for selected cases (referred to as prospective deeper sections), while others request additional deeper sections if the pathologist is unable to diagnose from the initial section (referred to as retrospective deeper sections). Though this practice provides enough evidence for better diagnosis of small biopsies, preparing and examining more sections can increase costs and cause delays in the dispatching of reports. Therefore, every pathologist's question is what should be the standard protocol for deeper sections to save time and money with a more appropriate diagnosis?
While reviewing the literature, we have encountered many studies regarding the utility of deeper sections in histopathology. The present study showed that a total of 36 cases (33.9%) needed deeper sections at various levels, compared to studies done by Lama G et al 1 (26.9%), Patil S et al 3 (10%) and Manyam R et al 2 (8%). This indicates that our study had a marginally higher frequency of deeper sections which can be attributed to the less sample size.
Our study showed that in 36% of the cases, the microscopic features were similar to those of the features in deeper sections. Each level was thoroughly examined for any additional features to the initial sections. Significant findings emerged in 11% of cases where the initial slides were non-diagnostic, whereas 36% of cases revealed additional diagnostic findings. In one case where the initial section showed only haemorrhage, the deeper section revealed cervical tissues with features of polyp with chronic cervicitis and mild atypia. This was in coherence with the study conducted by Parameswaran L et al 4. Deeper sections in small biopsies are routinely performed to enhance diagnostic sensitivity and accuracy. Our study revealed additional findings in 13 cases, consistent with other studies, such as 37.5% in Manyam R et al 2, 2.2% in Lama G et al 1, 7.3% in Yadav AB et al 5, and 4% in Patil S et al 3.
Interestingly, in one case of squamous cell carcinoma, the initial sections showed only squamous metaplasia, but in deeper sections, superficial epithelium with dysplastic islands in the stroma with keratin plug was visible. Another case with a clinical diagnosis of granulomatous reaction in the tendon
|
Categories |
Present study |
Lama et al 1 |
Manyam et al 2 |
Yadav et al 5 |
Patil et al 3 |
|
Frequency of Deeper sections |
33.9% |
26.9% |
8% |
9.6% |
10% |
|
Nondiagnostic initial slides |
11% |
28.2% |
47.5% |
20.7% |
44% |
|
Additional findings |
36% |
2.2% |
37.5% |
7.3% |
4% |
|
Similar findings |
36% |
67.4% |
15% |
38% |
- |
|
Misleading diagnosis |
6% |
- |
- |
- |
52% |
|
Tissue segment loss |
5% |
2.2% |
- |
- |
- |
sheath of a little finger showed no granulomas or giant cells in the initial section but the deeper section was consistent with Koch’s with chronic granulomatous inflammatory lesions with Langhans giant cells.
In 2 of the cases (5%), initial sections were as good or even better as there was tissue segment loss in deeper sections which showed coherence with studies of Lama et al 1 (2.2%), Parameswaran L et al 4 (1.3%) and Yadav AB et al 5 (3.6%). This shows that deeper sections are not always a boon. Therefore, care must be taken to get the deeper sections and close-level cutting would solve this issue of tissue segment loss in deeper sections rather than leaping between the microns.
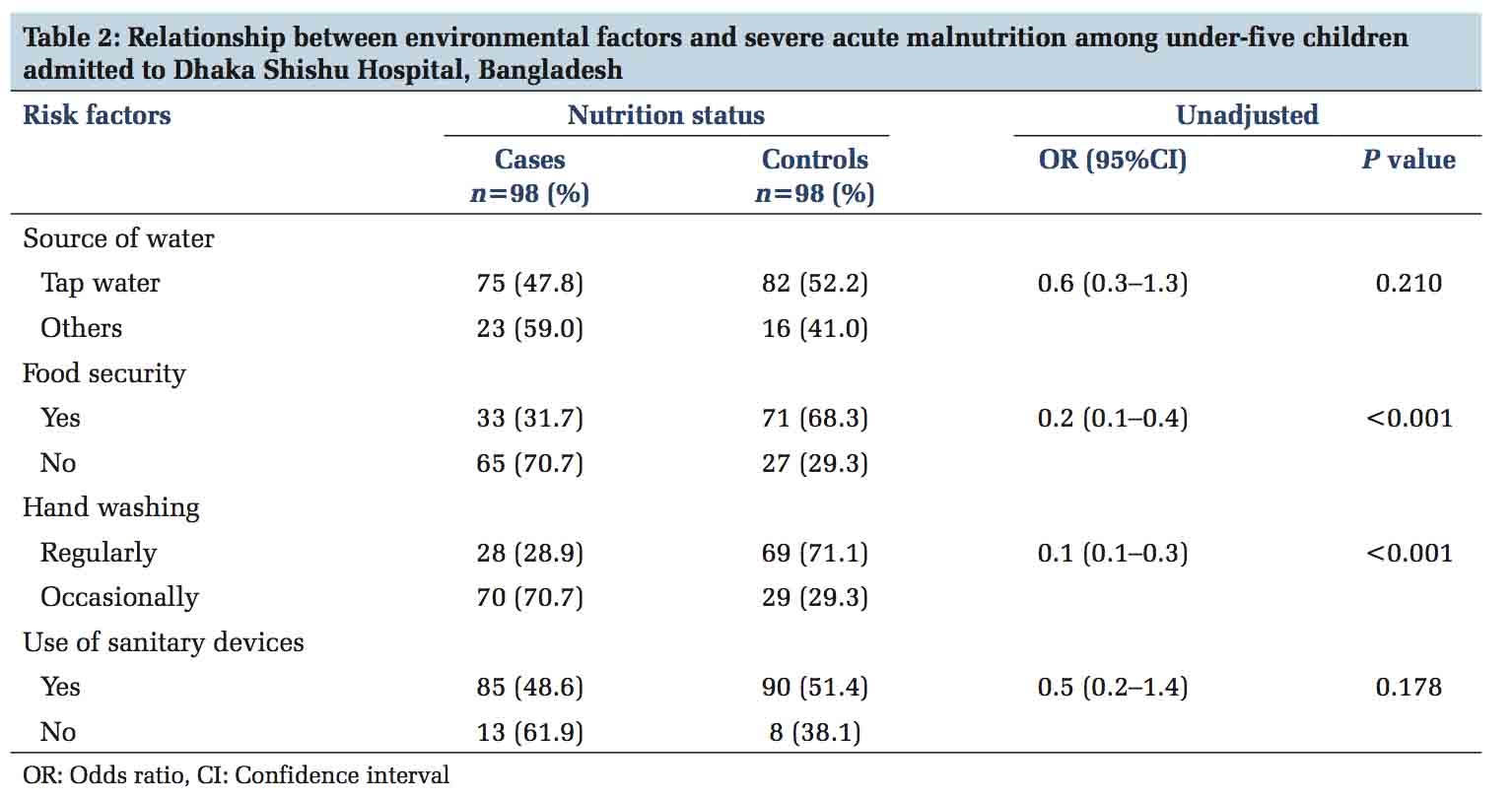
Comparison with other similar studies done in past are compared in the Table 2 using same categories as used in our study.
This study has certain limitations, including a restricted sample size due to the six-month study period, which may influence the broader applicability of the results. Furthermore, the lack of special stained slides might have reduced the ability to identify specific histopathological characteristics, potentially affecting diagnostic precision and thorough pathological evaluation.
This study highlights the critical role of deeper sections in improving diagnoses, particularly in regions with limited access to advanced diagnostic tools. It stresses the need for standardized terminology and varying depths based on tissue availability across organ systems. Deeper sections enhance diagnostic accuracy, guide better therapeutic decisions, and help identify hidden malignancies without affecting cost or case turnover. In low-resource settings, deeper sections are especially vital, given the constraints on advanced techniques like IHC and molecular studies.
Funding: Nil
Conflict of interest: Nil
Subscribe now for latest articles and news.