Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.v11.i1.24.231
Year: 2024, Volume: 11, Issue: 1, Pages: 74-78
Original Article
Shaifalika Thakur1 , Manish Kumar2 , Sunil Kishore2 , Jayant Prakash3
1Post Graduate Resident, Pediatric Medicine, Indira Gandhi Institute of Medical Sciences, Patna, Bihar, India,
2Associate Professor, Pediatric Medicine, Indira Gandhi Institute of Medical Sciences, Patna, Bihar, India,
3Head of Department, Pediatric Medicine, Indira Gandhi Institute of Medical Sciences, Patna, Bihar, India
Address for correspondence:
Manish Kumar, Associate Professor, Pediatric Medicine, Indira Gandhi Institute of Medical Sciences, Patna, Bihar, India.
E-mail: [email protected]
Received Date:21 July 2024, Accepted Date:06 August 2024, Published Date:24 February 2024
Background: Nephrotic syndrome (NS) in children often leads to alterations in serum biochemical parameters, including vitamin D and albumin levels. This study investigates the serum vitamin D levels during active nephrosis in children with NS and its correlation with serum albumin levels. Methods: This two-year observational cross-sectional study analyzed children diagnosed with nephrotic syndrome, focusing on their serum vitamin D and albumin levels. The study period spanned from start year to end year. We collected data on mean, standard deviation (SD), median, interquartile range (IQR), and range for both parameters. Given the non-normal distribution of vitamin D levels across the different NS patterns, we used the non-parametric Kruskal-Wallis test for group comparisons. Results: The mean (SD) serum albumin level was 1.28 (0.29) g/dL, with a median (IQR) of 1.20 (1.1-1.4) g/dL, ranging from 0.8 to 4.1 g/dL. The median vitamin D was (IQR) of 4.85 (3.02-6.47) ng/dL, ranging from 0.1 to 25 ng/dL. There were no significant differences in vitamin D levels between these groups (χ2 = 0.406, p = 0.939). Conclusion: Serum vitamin D levels do not significantly differ across various patterns of nephrotic syndrome in children. Additionally, there is no statistically significant correlation between serum vitamin D and albumin levels (rho = 0.01, p = 0.891). These findings suggest that vitamin D deficiency in children with nephrotic syndrome is independent of their serum albumin status and the pattern of the disease.
Keywords: Nephrotic syndrome, Children, Serum vitamin D, Serum albumin, Biochemical parameters
Nephrotic syndrome (NS) is a common disorder in children, characterized by significant proteinuria, hypoalbuminemia, hyperlipidaemia, and oedema.1 The condition results from increased glomerular permeability, allowing proteins, particularly albumin, to leak into the urine.2 This massive proteinuria leads to a marked reduction in serum albumin levels, a hallmark of nephrotic syndrome.
The hypoalbuminemia observed in nephrotic syndrome is primarily due to the loss of albumin through the urine, which exceeds the liver's capacity to synthesize this protein. Albumin is essential for maintaining oncotic pressure and transporting various substances in the blood, including hormones, drugs, and vitamins. In children with nephrotic syndrome, the depletion of serum albumin disrupts these functions and contributes to various complications.
One critical complication arising from low serum albumin levels is vitamin D deficiency. Vitamin D, a fat-soluble vitamin, binds to vitamin D-binding protein (DBP) in the blood for transport. In nephrotic syndrome, the loss of albumin and DBP through urine significantly reduces the levels of circulating vitamin D. Additionally, the proteinuria-induced hypoalbuminemia may impair the renal conversion of vitamin D to its active form, further exacerbating the deficiency. 3
Vitamin D plays a crucial role in calcium and phosphate metabolism, bone health, and immune function. Deficiency in vitamin D can lead to rickets in children, characterized by bone deformities and growth retardation, and can also impact overall health and well-being. Understanding the relationship between serum vitamin D and albumin levels in children with nephrotic syndrome is essential for developing effective management strategies to mitigate these complications.
This study aims to investigate serum vitamin D levels during active nephrosis in children with nephrotic syndrome and to explore its correlation with serum albumin levels. By elucidating these relationships, we hope to enhance our understanding of the biochemical disturbances in nephrotic syndrome and possibly improve patient outcomes.
This observational, individual-based, analytical cross-sectional study was conducted in the Department of Paediatrics at the Indira Gandhi Institute of Medical Sciences (IGIMS), Sheikhpura, Patna, Bihar, India over two years (July 2022 - July 2024). The study recruited children aged 1-14 years with nephrotic syndrome from the IPD and OPD. The sample size, calculated based on a 60% prevalence of metabolic bone disease in nephrotic syndrome, required a minimum of 369 participants, which was achieved using Epi Info Software (CDC). 4
Data collection included patient demographics, detailed history, and clinical examination. Key variables recorded were age of onset, disease pattern (remission or active, including first episode, first relapse, infrequently relapsing, or frequently relapsing), steroid responsiveness, and drug treatment history. Blood and urine investigations confirmed disease status and assessed biochemical profiles relevant to our study, mainly, Serum Vitamin D levels and Serum Albumin levels.
Patients who met the inclusion criteria (children with normal creatinine levels) and did not meet the exclusion criteria (congenital or secondary nephrotic syndrome, osteogenesis imperfecta, juvenile osteoporosis) were included. Written informed consent was obtained from guardians and assent from the children where applicable. Ethical clearance was obtained before the study. The Kruskal-Wallis test was used for group comparisons of vitamin D levels, and Spearman's rank correlation coefficient assessed the correlation between serum albumin and vitamin D levels.
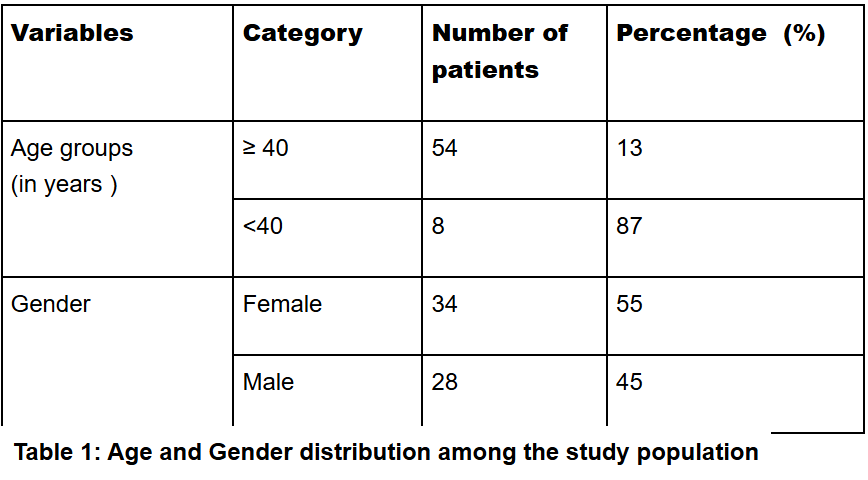
A total of 370 children aged 1-14 years with nephrotic syndrome participated in the study. The mean age of the participants was 6.02 ± 3.33 years. Age distribution showed that 184 (49.7%) participants were in the 1 to 5 years age group, 137 (37.0%) in the 6 to 10 years age group, and 49 (13.2%) in the 11 to 14 years age group. Gender distribution indicated that 263 (71.1%) participants were male, and 107 (28.9%) were female.
Regarding the pattern of nephrotic syndrome, 144 (39.2%) had their first episode, 67 (18.3%) experienced their first relapse, 56 (15.3%) had infrequent relapses (IFRNS), and 100 (27.2%) had frequent relapses (FRNS). In terms of steroid responsiveness, 358 (96.8%) were steroid-sensitive, while 12 (3.2%) were steroid-resistant. Three participants could not be classified according to pattern of the disease due to unreliable clinical history.
|
Clinical Details |
Mean ± SD || Median (IQR) || Min-Max or N (%) |
|---|---|
|
Age (Years) |
6.02 ± 3.33 || 6.00 (3.00-8.00) || 1.00 - 14.00 |
|
Age Group |
|
|
1 to 5 Years |
184 (49.7%) |
|
6 to 10 Years |
137 (37.0%) |
|
11 to 14 Years |
49 (13.2%) |
|
Gender |
|
|
Male |
263 (71.1%) |
|
Female |
107 (28.9%) |
|
Weight (Kg) |
21.24 ± 8.26 || 20.00 (15.00-27.00) || 7.00 - 47.00 |
|
Height (cm) |
1.40 ± 5.05 || 1.12 (1.00-1.25) || 0.68 - 98.00 |
|
Age o f Onset o f NS (Years) |
4.63 ± 2.90 || 4.00 (2.00-6.00) || 1.00 - 13.00 |
|
Duration of Illness (Years) |
1.66 ± 1.78 || 1.00 (0.50-2.00) || 0.50 - 14.00 |
|
Pattern |
|
|
First Episode |
144 (39.2%) |
|
First Relapse |
67 (18.3%) |
|
IFRNS |
56 (15.3%) |
|
FRNS |
100 (27.2%) |

The mean serum albumin level was 1.28 ± 0.29. The median vitamin D level was (IQR) of 4.85 (3.02-6.47) ng/mL, and a range from 0.1 to 25 ng/mL. Vitamin D levels were not normally distributed across the four subgroups of nephrotic syndrome patterns, leading to the use of the Kruskal-Wallis test for group comparisons.
The median (IQR) vitamin D levels in different patterns of the disease were as follows: first episode 4.95 (3-6) ng/mL, first relapse 4.8 (3.05-6.75) ng/mL, IFRNS 4.5 (3.5-6.35) ng/mL, and FRNS 5 (3-6.05) ng/mL. The range of vitamin D levels for the first episode was 0.8 to 15.5 ng/mL, for the first relapse 1 to 17 ng/mL, for IFRNS 0.1 to 25 ng/mL, and for FRNS 0.3 to 13 ng/mL.
|
Pattern |
Vitamin D |
Fisher's Exact Test |
||||
|---|---|---|---|---|---|---|
|
<10 ng/mL |
10-20 ng/mL |
>20 ng/mL |
Total |
χ2 |
P Value |
|
|
First Epis- ode |
135 (39.9%) |
9 (32.1%) |
0 (0.0%) |
144 (39.2%) |
6.308 |
0.560 |
|
First Rela- pse |
61 (18.0%) |
6 (21.4%) |
0 (0.0%) |
67 (18.3%) |
||
|
IFRNS |
50 (14.8%) |
5 (17.9%) |
1 (100.0%) |
56 (15.3%) |
||
|
FRNS |
92 (27.2%) |
8 (28.6%) |
0 (0.0%) |
100 (27.2%) |
||
|
Total |
338 (100.0%) |
28 (100.0%) |
1 (100.0%) |
367 (100.0%) |
||

Out of 370 participants in the study, Vitamin D status of 367 was evaluated. There was no significant difference in vitamin D levels among the groups (χ2 = 0.406, p = 0.939), as seen in Figure 2. Additionally, there was no statistically significant correlation between serum albumin and vitamin D levels (rho = 0.01, p = 0.891), seen in Figure 3.

Fisher's exact test was used to analyze the association between vitamin D levels and steroid responsiveness due to a low expected count in more than 20% of cells. There was no significant difference between the groups in terms of steroid responsiveness (χ2 = 0.043, p = 1.000). The strength of association was minimal, with Cramer's V at 0.01 and Bias Corrected Cramer's V at 0. Among participants with vitamin D <10 ng/mL, 96.8% were steroid-sensitive and 3.2% were steroid-resistant. For those with vitamin D 10-20 ng/mL, 96.4% were steroid-sensitive and 3.6% were steroid-resistant. All participants with vitamin D >20 ng/mL were steroid-sensitive.
This study aimed to evaluate the relationship between vitamin D levels and various clinical parameters in children with nephrotic syndrome (NS) at a tertiary care center. Our findings indicate that the majority of children with NS had low vitamin D levels, with a mean of 5.18 ± 2.99 ng/mL. The distribution of vitamin D levels did not significantly differ across different patterns of NS, nor did it correlate significantly with steroid responsiveness.
In contrast, Yousefichaijan et al.'s prospective study of 218 children aged 1-13 reported that vitamin D deficiency (<10 ng/mL) was significantly more prevalent in steroid-resistant (79%) and steroid-dependent (83%) nephrotic syndrome compared to steroid-sensitive (17%) cases (P < 0.0001). Their study also showed a higher proportion of sufficient vitamin D levels (30-150 ng/mL) in steroid-sensitive cases (91%) compared to steroid-dependent (17%) and steroid-resistant (7%) cases (P = 0.002). These contrasting results highlight a stronger correlation between vitamin D levels and steroid responsiveness in Yousefichaijan et al.'s study, suggesting further research is needed to explore these associations. 5
Our study examined 370 children with nephrotic syndrome (NS) and found a mean age of 6.02 ± 3.33 years, which is comparable to the mean age of 6.75 ± 3.6 years reported by Manideepa et al. In both studies, the majority of participants were experiencing their first episode of NS, with 39.2% in our study and 50% in theirs. The distribution of vitamin D levels in our study was also not normally distributed, consistent with the findings of Manideepa et al. However, our study found a much lower median vitamin D level of 5.18 ng/mL compared to 13.10 ng/mL reported by Manideepa et al. 6
The range of vitamin D levels in our study was from 0.1 to 25 ng/mL, indicating a more severe deficiency compared to the range of 2.4 to 50.3 ng/mL in their study. This stark difference highlights the variability in vitamin D status among different cohorts of children with NS and underscores the need for region-specific strategies to address this deficiency. 6
Our study included 370 children with nephrotic syndrome (NS), while Badyal et al. focused on 50 cases of NS in remission.7 The mean age of onset in our study was 6.02 ± 3.33 years, which is slightly higher compared to 4.9 years in the Badyal et al. study. Both studies reported a male predominance, with our study having 71.1% males and Badyal et al. reporting a male to female ratio of 1.38:1.
In terms of NS patterns, our study observed 39.2% first episode cases, whereas Badyal et al. found 28% first episode cases. Additionally, our study reported 96.8% steroid-sensitive cases compared to a mix of 20 frequent relapsers (FR), 6 infrequent relapsers (IR), 8 steroid-dependent (SDNS), and 2 steroid-resistant (SRNS) cases in Badyal et al.
Regarding vitamin D levels, our study found a mean level of 5.18 ng/mL with severe deficiencies, while Badyal et al. reported that 46% of patients had vitamin D deficiency, 28% had insufficiency, and 26% had normal levels. This discrepancy highlights the variability in vitamin D status among different cohorts.
Badyal et al. also found significant differences in vitamin D levels between frequent and infrequent relapsers, with a strong positive correlation between calcium and vitamin D levels (r=0.720, p<0.001). Our study did not find a significant correlation between serum albumin and vitamin D levels (rho = 0.01, p = 0.891). Overall, both studies emphasize the prevalence of vitamin D deficiency in children with NS.
Our study highlights the significant prevalence of vitamin D deficiency among children with nephrotic syndrome (NS). Despite varying patterns of NS, there was no significant difference in vitamin D levels across different subgroups. No association was established between Serum vitamin D levels and serum albumin levels. The findings underscore the importance of monitoring and managing vitamin D levels in pediatric NS patients to potentially improve outcomes.
This study has several limitations. First, it was conducted at a single center, which may limit the generalizability of the results. Second, the cross-sectional design precludes the assessment of causality between vitamin D levels and NS outcomes. Additionally, seasonal variations in vitamin D levels were not accounted for, and other factors influencing vitamin D status, such as dietary intake and sun exposure, were not controlled.
Future research should focus on multi-center studies to validate these findings across diverse populations. Longitudinal studies are needed to explore the causal relationship between vitamin D deficiency and NS progression or relapse rates. It is also recommended to assess the impact of vitamin D supplementation on NS outcomes and to consider routine screening and management of vitamin D levels as part of standard care for children with NS.
The author declares no conflict of interest.
This research was conducted without any financial support from external sources or funding agencies. All expenses incurred during this study were covered by the author.
Subscribe now for latest articles and news.