Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.v10.i1.23.317
Year: 2024, Volume: 10, Issue: 1, Pages: 16-25
Original Article
N Manjula1 , C Jayanthi2 , S Srivani3 , Damodara Kumaran4
1Senior Resident, Dhanalakshmi Srinivasan Institute of Medical Sciences and Hospital, Thuraiyur Road, Perambalur, 621 212, Tamil Nadu, India,
2Associate Professor, Department of Pathology, Sri Manakula Vinayagar Medical College and Hospital, Kalvi Vallal N. Kesavan Salai, Kalitheerthalkuppam, Madagadipet, Puducherry, 605 107, India ,
3Professor, Department of Pathology, Sri Manakula Vinayagar Medical College and Hospital, Kalvi Vallal N. Kesavan Salai, Kalitheerthalkuppam, Madagadipet, Puducherry, 605 107, India,
4Assistant Professor, Department of Clinical Oncology, Sri Manakula Vinayagar Medical College and Hospital, Kalvi Vallal N. Kesavan Salai, Kalitheerthalkuppam, Madagadipet, Puducherry , 605 107, India
Address for correspondence:
C Jayanthi, Associate Professor, Department of Pathology, Sri Manakula Vinayagar Medical College and Hospital, Kalvi Vallal N. Kesavan Salai, Kalitheerthalkuppam, Madagadipet, Puducherry, 605 107, India .
E-mail:
[email protected]
Received Date:29 October 2023, Accepted Date:10 January 2024, Published Date:30 March 2024
Background: Breast cancer is a diverse disease with varying characteristics in morphology, presentation, treatment, and prognosis. It constitutes 25% of cancers in Indian women. This study delves into rare special variants and differentiated ductal carcinomas, focusing on their unique histological features and molecular profiles. Aim: To scrutinize the spectrum of special forms of breast carcinoma and their immunohistochemistry (IHC) profile. Material and methods: A retrospective analysis of all the breast carcinomas over a period of 11 months was carried out. The clinical, gross, microscopic and immunohistochemistry findings of 15 special variants and differentiated ductal carcinomas were noted down. Results: In a retrospective analysis of 50 cases of breast carcinoma, 15 were diagnosed as special variants of breast malignancy which accounted to be 30%. Out of the 21 rare histologic subtypes of breast carcinoma 10 variants were encountered by us that included mucinous carcinoma, lobular carcinoma, papillary carcinoma, invasive breast carcinoma with medullary pattern, invasive breast carcinoma with oncocytic pattern, metaplastic carcinoma, cribriform carcinoma, malignant adenomyoepithelioma, secretory carcinoma, and invasive breast carcinoma with neuroendocrine differentiation. Conclusion: This study provides a comprehensive overview of the gross and microscopic features, as well as the immunohistochemistry profiles of these special variants and differentiated ductal carcinomas of the breast. We anticipate that this research will enhance our understanding of these uncommon breast cancer variants, with a particular emphasis on their molecular characteristics, contributing to improved management strategies in the future.
Keywords: Breast Cancer, Immunohistochemistry, Molecular Classification
Invasive breast cancer is a heterogeneous disease in its presentation, clinical course and classification which includes both pathological and molecular. According to latest reports from National Cancer Registry Program (NCRP) breast cancer is one of the most common cancers among Indian females 1. Invasive breast cancer arises from the lining epithelium of the ducts (85%) or lobules (15%) primarily from terminal duct lobular unit 2. Based on the cell morphology and architecture the recent World health organisation (WHO) has classified invasive breast carcinomas into 21 histologic subtypes. Most of breast carcinomas previously termed as “ductal” carcinomas are now categorized as “Invasive ductal carcinoma- no special type,” (IDC-NOS) accounting to about 75% to 80%. Following it, the second most common type of breast carcinoma is the Invasive lobular carcinoma, representing about 5% to 15% 3.
In addition to histopathological examination (HPE), immunohistochemistry (IHC) and molecular pathology plays a major role in predicting the clinical course and outcome of breast cancers. Histopathological examination plays a pivotal role in affirming the special variants of breast carcinoma. Since the prevalence of such breast cancer is low, no much of study are available on the clinical and molecular characteristics of special variants of breast cancer. Routine chemotherapy (Paclitaxel) used in IDC- NOS have showed to have a decreased response in special types of breast cancer 4. Hence identification of special types of breast cancer is essential for initiating appropriate treatment for these patients.
The aim of our study is to determine the clinical, morphological, histopathological and molecular classification of the special and differentiated variants of breast carcinoma. This may also stand as a clinical framework for a future understanding of these rare breast cancers.
It is a retrospective study carried out for a period of 11 months in the Department of Pathology at Sri Manakula Vinayagar Medical College & Hospital after getting approval from the institutional ethics committee (EC/45/2022 dated on 10/2/2022) which included patients diagnosed with special and differentiated variants of breast carcinoma from mastectomy and wide local excision specimens. This study excluded the patients who have received neoadjuvant therapy and patients diagnosed with invasive breast carcinoma of no special type from tissue biopsy and resection specimen obtained from breast.
Totally around 100 breast specimens including the biopsy and resection were received in our department during the study period. Of which 50 were benign and 50 were malignant. Among the 50 malignant cases 15 were of special type.
All the specimens were fixed in 10 % formalin and were grossed as per protocol. The sections were stained using hematoxylin and eosin (H&E) stain and were examined under light microscope. Histopathological reporting was done as per College of American Pathologists (CAP) protocol. IHC using estrogen receptor (ER), progesterone receptor (PR), HER2neu and other relevant markers were used when necessary.
The cases were studied for the histological type, grade, ER, PR, HER2neu status and molecular classification was done.
IHC was performed using polymer kit as per standard protocol. IHC was done on 4μm thick formalin fixed paraffin embedded tissue sections using lysinated slides. Antigen retrieval was done by using pressure cooker method. TrisEDTA buffer was used. Antibodies used for ER, PR and HER 2 were monoclonal antibodies against estrogen receptor (Clone SP1), progesterone receptor (Clone 16) and Her2 receptor (Clone SP3) respectively. The slides were incubated with DAB chromogen and counter stained with Harris Hematoxylin. Then percentage of cells staining positive was recorded.
According to ASCO and CAP guidelines cutoff of 1% of tumor cells positive for nuclear stain of ER/PR was considered to be positive and the tumors staining < 1% of any intensity was considered negative.
For HER 2, a semiquantitative scoring system called Allred scoring system was used which is based on percentage of positively stained cells and intensity of nuclear stain of the cells. A cutoff of > 10% of tumor cells positive for membraneous staining of HER 2 was considered positive and the tumors staining < 10% was considered negative. HER 2 was scored from 0 to 3 (Table 1).
|
Staining Pattern |
Score |
Her2neu Interpretation |
|
No stain or incomplete, faint in <10% tumor cells. |
0 |
Negative |
|
Faint, incomplete staining in <10% tumor cells. |
1+ |
Negative |
|
Complete, weak to moderate staining in >10% of tumor cells. |
2+ |
Equivocal |
|
Complete circumferential membrane staining in >10% of tumor cells. |
3+ |
Positive |
The tumors were classified into three groups (luminal A, luminal B and basal / triple negative) according to ER/PR and HER 2 status (Table 2).
|
Molecular Subtype |
ER status |
PR status |
HER2neu status |
|
Luminal A |
Positive |
Positive |
Negative |
|
Luminal B |
Positive |
Positive |
Positive |
|
Basal/Triple negative |
Negative |
Negative |
Negative |
This study is a retrospective study that included 50 cases of breast carcinoma out of which 15 were diagnosed as special and differentiated variants of breast malignancy which accounts for 30%. These special variants includes 3 (20%) cases of mucinous carcinoma, 2 (13.33%) cases of lobular carcinoma, 2 (13.33%) cases of papillary carcinoma, 2 (13.33%) cases of invasive breast carcinoma with medullary pattern, 1 (6.66%) case of invasive breast carcinoma with oncocytic pattern, 1 (6.66%) case of metaplastic carcinoma, 1 (6.66%) case of cribriform carcinoma, 1 (6.66%) case of malignant adenomyoepithelioma, 1 (6.66%) case of invasive breast carcinoma with neuroendocrine differentiation and 1 (6.66%) case of secretory carcinoma.
The patient’s age ranged from 34 to 65 years with mean age of 51.66 years. Most common age of presentation was in 6th decade. Only one patient (6.66%) turned out to be of male gender. There were 14 (93.33%) modified radical mastectomy (MRM) specimens and 1 (6.66%) wide local excision specimen. Pre operative cytological diagnosis of invasive breast carcinoma was made on fine needle aspiration cytology (FNAC) for all the cases. Mention on the special variant type was not given in cytological reports except for one of the mucinous carcinomas. Out of 15 cases 10 (66.66%) were right sided and 5 (33.33%) were left sided. Of the total, 5 (33.33%) cases were in lower outer quadrant and 2 (13.33%) in central quadrant and 2 (13.33%) had multifocal tumor. Of these cases most commonly reported stage was pT2 and the highest stage reported was pT4b, most common grade reported was grade 3 with score 9.
The details of these special variants of breast carcinoma including gross findings, microscopic diagnosis, IHC findings and molecular subtyping are highlighted in Table 3.
|
S. NO |
Age |
Gross |
Histopathological Diagnosis |
IHC |
Molecular Subtype |
||
|
ER |
PR |
HER2neu |
|||||
|
1 |
63 |
Solid – cystic |
Encapsulated papillary carcinoma with invasion |
-VE |
-VE |
-VE |
BASAL |
|
2 |
52 |
Multifocal with mucoid areas |
Mixed Mucinous carcinoma |
+VE |
+VE |
-VE |
LUMINAL – A |
|
3 |
62 |
Solid |
Extensive LCIS with foci of invasive component |
+VE |
+VE |
EQUIVOCAL
(+/- 2) |
LUMINAL – B |
|
4 |
64 |
Ulceroproliferative growth with friable, hemorrhagic and necrotic area |
Metaplastic carcinoma. |
-VE |
-VE |
-VE |
BASAL |
|
5 |
51 |
Poorly circumscribed solid lesion |
Malignant adenomyoepithelioma |
-VE |
-VE |
-VE |
BASAL |
|
6 |
65 |
Solid lesion with infiltrating borders |
Solid papillary carcinoma with invasion |
+VE |
+VE |
-VE |
LUMINAL – A |
|
7 |
41 |
Solid with mucoid area |
Pure Mucinous carcinoma |
+VE |
+VE |
-VE |
LUMINAL – A |
|
8 |
53 |
Solid |
Invasive lobular carcinoma |
+VE |
+VE |
-VE |
LUMINAL – A |
|
9 |
36 |
Multifocal with mucoid areas |
Invasive breast carcinoma with mucinous differentiation |
+VE |
FOCALLY +VE |
-VE |
LUMINAL – A |
|
10 |
34 |
Solid |
Cribriform carcinoma |
-VE |
-VE |
-VE |
BASAL |
|
11 |
65 |
Solid |
Invasive breast carcinoma with oncocytic pattern |
+VE |
+VE |
-VE |
LUMINAL – A |
|
12 |
45 |
Solid |
Invasive breast carcinoma with medullary pattern |
-VE |
-VE |
-VE |
BASAL |
|
13 |
40 |
Solid |
Invasive breast carcinoma with medullary pattern |
-VE |
-VE |
-VE |
BASAL |
|
14 |
54 |
Solid |
Invasive breast carcinoma with neuroendocrine differentiation |
+VE |
+VE |
-VE |
LUMINAL – A |
|
15 |
50 |
Solid with few cystic spaces |
Secretory carcinoma |
-VE |
-VE |
-VE |
BASAL |
36/F presented with right breast lump for 4 months. Right Modified Radical Mastectomy with multifocal (3) tumor, largest measuring 5 X 5 X 3.5 cms - firm to hard in consistency with glistening areas was seen Figure 1. Microscopy showed foci of invasive ductal carcinoma admixed with mucinous carcinoma characterized by tumor cells floating in lakes of mucin. The presence of mucin was highlighted by special stain Periodic acid-schiff (PAS) and percentage of mucin was found to be between < 50 %, hence was diagnosed as Invasive ductal carcinoma with mucinous differentiation Figure 1. The cells were ER positive, PR focally positive and Her2neu negative. Finally diagnosed as mpT2N1a Invasive ductal carcinoma with mucinous differentiation.
41/ F presented with right breast lump for 1 month. Right Modified Radical Mastectomy revealed a tumor measuring 1.9 X 1.4 X 1 cms. Microscopy showed clusters of neoplastic cells suspended in abundant extracellular mucin, mucin accounted for > 90% Figure 1 . The cells were ER positive, PR positive and Her2neu negative. Finally diagnosed as pT1cN0 Pure Mucinous Carcinoma.
52/ F presented with right breast lump for 2 years. Right Modified Radical Mastectomy showed multifocal (2) tumor, largest measuring 2.2 X 2 X 2 cms, grey white with foci of mucoid areas. Microscopy showed clusters of neoplastic cells suspended in abundant extracellular mucin separated by delicate fibrous septa. The amount of mucin was found to be between 50 and 90%. The tumor cells were ER positive, PR positive and Her2neu negative. Finally diagnosed as mpT2N0 Mixed Mucinous carcinoma.
63/F presented with left breast lump, underwent Left Modified Radical Mastectomy. Cut surface revealed uniloculated cyst measuring 9 X 6 cm with a mural nodule measuring 5 X 5 X 2 cm which was grey white and firm in consistency. Inner surface of cyst was soft and regular. Microscopy showed papillary mass with in a cystic space with a foci of invasion by highly pleomorphic round to spindle shaped cells. The spindle shape cells in the invasive component were positive for Vimentin Figure 1 and negative for ER, PR, Her2neu. Finally diagnosed as pT3N0 Encapsulated papillary carcinoma with invasion.

65/F presented with left breast lump and bloody nipple discharge. Left Modified Radical Mastectomy specimen revealed solid grey white hard tumor measuring 3.7 X 3.1 X 3 cm. Microscopy showed expansile nodules in solid growth pattern with conspicuous delicate fibro vascular core Figure 1. The cells were ER positive, PR positive and Her2neu negative. A diagnosis of pT2N0 Solid papillary carcinoma with invasion was given.
53/ F presented with right breast lump for 1 year. Wide Local Excision revealed a grey white tumor measuring 4 X 3 X 1 cm. Microscopy showed discohesive proliferation of tumor cells arranged in Indian File Pattern. The cells were ER positive, PR positive and Her2neu negative. Diagnosed as pT2N0Invasive lobular carcinoma.
Right Modified Radical Mastectomy specimen from 62 yrs female revealed a grey white firm tumor measuring 2.7 X 2.1 X 1.5 cm. Microscopy showed discohesive proliferation of tumor cells with a foci of invasion. The cells were ER positive, PR positive and Her2neu equivocal (+/-2). Finally diagnosed as pT2N0 Invasive lobular carcinoma / Extensive LCIS with foci of invasion.
45/ F presented with right breast lump for 1 year. Right Modified Radical Mastectomyrevealed a well circumscribed grey white firm tumor measuring 2.6 X 1.5 X 1.2 cm. Microscopy showed high grade tumor with syncytial arrangement of tumor cells with large areas of necrosis Figure 1. The tumor cells were ER negative, PR negative and Her2neu negative. A diagnosis of triple negative pT2N1a Invasive breast carcinoma with medullary features was given.
Left Modified Radical Mastectomy from 40 years female revealed well circumscribed tumor measuring 3 X 2 X 2 cm. Microscopy showed high grade tumor with syncytial arrangement of tumor cells with large areas of necrosis, surrounded by dense inflammatory infiltrates. The tumor cells were negative for ER, PR and Her2neu. Finally diagnosed as pT2N1a Invasive breast carcinoma with medullary features.
Right Modified Radical Mastectomy from 65/F showed a 2 X 2 X 1.5 cm tumor. Microscopy showed sheets of tumor cells with eosinophilic granular cytoplasm, well defined border and centrally placed nucleus Figure 2. The cells were ER positive, PR positive and Her2neu negative. Finally diagnosed as pT1cN0 Invasive breast carcinoma with oncocytic features.

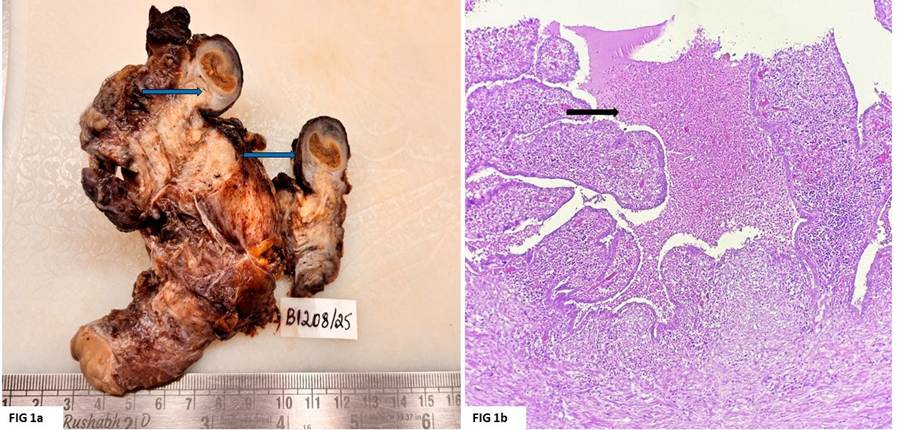
64 /F, post chemo case of left breast carcinoma. Cut surface of Left Modified Radical Mastectomy revealed solid friable ulceroproliferative and infiltrative lesion measuring 14.5 X 14 X 8.5 cm Figure 2. Microscopy showed poorly differentiated invasive ductal carcinoma admixed with large areas of metaplastic squamous cells and pleomorphic spindle shaped cells arranged in a haphazard manner Figure 2. The tumor cells were negative for ER, PR and Her2neu. Pan Cytokeratin (Pan CK) positivity was identified in the squamous cells and Vimentin positivity was observed in spindle shaped cells. Based on the above findings a diagnosis of ypT4bN2a Metaplastic carcinoma was offered.
Received Left Modified Radical Mastectomy from 34 yrs old which on cutting revealed grey white hard tumor measuring 4 X 3.5 X 3 cm. Microscopy showed invasive tumor islands containing well defined rounded spaces surrounded by a desmoplastic stroma Figure 2. The tumor cells were ER negative, PR negative and Her2neu negative. Morphological features were that of ypT2N3cCribriform carcinoma.
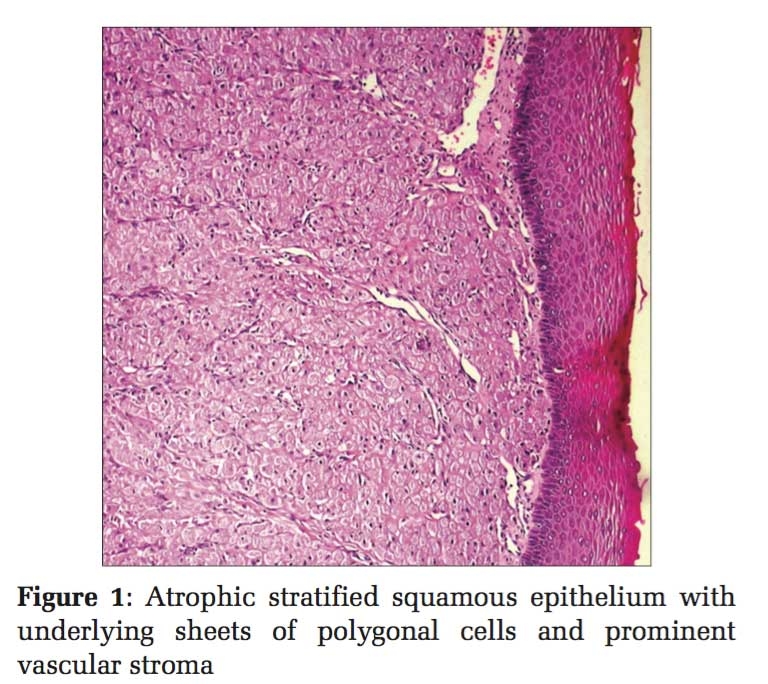
Right Modified Radical Mastectomy from 51/ F on cut surface revealed poorly circumscribed hard tumor measuring 3.9 X 2.9 X 2.8 cm. Microscopy showed tubular and sheet like arrangement of pleomorphic cells and papillary structure with eosinophilic inclusions admixed with dense desmoplastic stroma. Focal area of spindle cells, clear cells with cystic area was also seen. The tumor cells were negative for ER, PR, and Her2neu and positive for p63and SMA in the areas of myoepithelial componentFigure 2. A comprehensive diagnosis of pT2N0 Malignantadenomyoepithelioma was offered.
Right Modified Radical Mastectomy from 54/ male revealed circumscribed, firm to hard tumor measuring 4 X 3.2 X 2 cm. Microscopy showed nests of tumor cells with salt and pepper chromatin Figure 2. The tumor cells were positive for ER, PR and negative for Her2neu. Moreover, the tumor cells showed a variable expression to synaptophysin. Finally, a diagnosis of pT2N1a Invasive breast carcinoma with neuroendocrine differentiation was made.
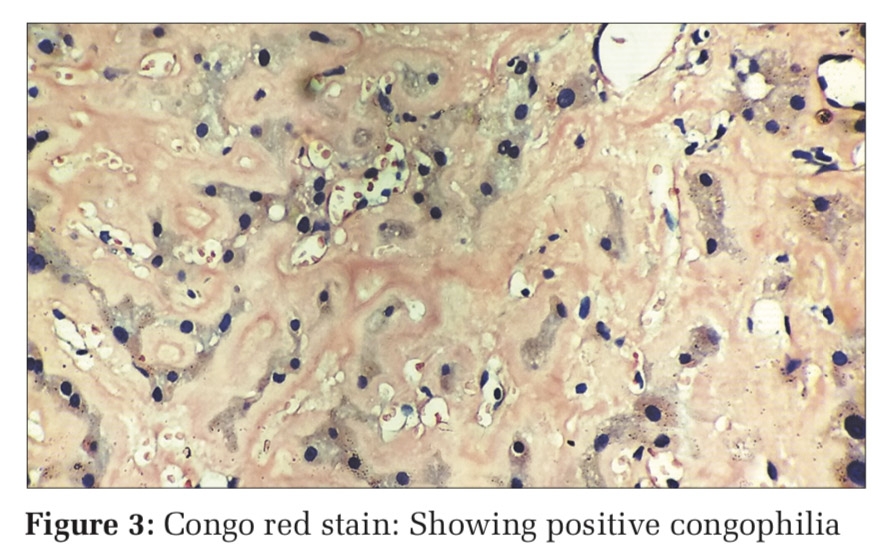
50 years old female with breast mass underwent Right Modified Radical Mastectomy. Cut surface revealed a large tumor measuring 19 X 13.5 X 10 cm which was solid with cystic areas. The tumor cells were arranged in microcystic pattern with intracytoplasmic and extracellular eosinophilic secretions Figure 2. The tumor cells were negative for ER, PR and Her2neu. Based on histomorphology a final diagnosis of pT4N0 Secretory carcinoma was made.
Out of 50 cases diagnosed with breast carcinoma there were 15 special types with distinct morphological features identified in our tertiary care centre. Due to rarity of these special types of breast carcinoma, only limited literature was available. To the best of our knowledge most of the literatures available were in the form of case reports. But in our study, we have highlighted clinical, gross, microscopic and immunohistochemical findings of these rare subtypes of breast carcinoma. Breast carcinoma includes various subtypes which differ in their outcome and treatment option. Thus, a detailed histopathological examination with special mention of variants of breast carcinoma is essential for treatment and to assess the prognosis of patients. This study has been conducted to emphasize the importance of histopathological examination along with IHC in diagnosing special types of breast carcinoma.
Production of abundant extracellular and/or intracellular mucin qualifies the tumor as pure mucinous carcinoma. Presence of 90%, 50-90% and less than 50% of mucin in an invasive breast carcinoma entitles to be called as pure mucinous, mixed mucinous and invasive carcinoma with mucinous differentiation respectively 5. Mucinous breast cancer tends to be slower growing than other types and occurs more often in older women and is less likely to spread to the lymph nodes 6. In our study we have observed divergent results as all the carcinomas with mucinous component presented in their third to fifth decade. Conventionally the above tumor shows rare axillary lymph node involvement which was in contrary to our finding of noticing one case with regional lymph node metastasis. One of the intriguing findings in our study is that two out of the three mucinous carcinomas were multifocal which was not described in any of the studies previously.
Solid papillary carcinoma characteristically has papillae with focal solid areas. It is considered to be an indolent variant of breast carcinoma with no nodal metastasis. Immunohistochemical marker analysis of our case was in concordance with many other studies by exhibiting ER and PR positivity and HER 2 neu negativity. Encapsulated papillary carcinoma (EPC) is a biologically unique category of breast carcinoma which have neoplastic cells arranged in papillary architecture in a well-defined cystic space. The invasive potential of the above tumor is intermediate between ductal carcinoma in situ and IDC of breast. We had observed invasive tumor with spindle cell morphology in our series similar to findings by Hashmi et al who have reported that 43.8% of the EPC were associated with invasive component in his study 7. EPC is usually of luminal A type which was in divergence to our case which turned out to be of the basal type.
Being the second most common epithelial type invasive lobular carcinoma (ILC) comprises of 5%–15% of the epithelial tumors 3. Shakoor et al found that ILC was significantly more likely to spread to distant sites. This behaviour is due to increased expression of E-cadherin which predisposes to discohesiveness of the tumor cells 8. In our study one case was of the luminal A and other one was of the luminal B subtype however Her2neu positivity is very rarely described in literatures. Data released by National Cancer Institute have noted triple negative breast cancer is a type of breast cancer which accounts for 15% of all breast carcinomas 9. In our study there are 7 triple negative breast cancer which accounts for 46.66 %.
Currently carcinoma with medullary pattern, oncocytic carcinoma and invasive carcinoma with neuroendocrine differentiation do not signify to be considered as any special types of breast carcinoma but are now considered morphological patterns of IBC-NST regardless of the extent of differentiation/pattern, and the 90% rule for special subtype is not applied to these tumours 10. Medullary carcinoma represents less than 2% of breast carcinoma with increased incidence in younger age group 11. These highly proliferative tumors are frequently found to be triple negative as justified by our observation. These tumors have decreased frequency of nodal metastasis with disease free survival reaching 95%. In our series oncocytic carcinoma showed neoplastic cells featuring eosinophilic and granular cytoplasm due to high numbers of mitochondria and was of the luminal A subtype. There is an increased frequency of neuroendocrine differentiation observed in mucinous and solid papillary carcinoma when compared to IBC-NOS 12. Presence of occasional foci of histological features of neuroendocrine differentiation qualified our case to be of invasive carcinoma with neuroendocrine differentiation. However its incidence ranges from 10%-30% in the various published literatures 2.
Metaplastic breast cancers are a heterogeneous group of tumors with an incidence of 0.2%–0.6%, and the median age at presentation is 47–61 years 13. Our case of metaplastic carcinoma had a mixture of squamous cell carcinoma, spindle cell carcinoma and carcinoma with osseous differentiation which was found to be even more exceptional. Supporting the literature our molecular profile of the above tumor was found to be triple negative with high Ki67. However, despite being established to be generally a nodal negative tumor our case had multiple axillary lymph node metastasis. Belonging to low grade breast carcinoma family cibriform carcinoma accounts to 0.1%–0.6% of breast cancers 14. The molecular profile of our reported case was divergent from established data by showing triple negative tumor which is noteworthy.
Secretory carcinoma more prevalent in young females had neoplastic cells with granular eosinophilic cytoplasm along with intracellular/extracellular secretion. Having low Ki67 expression these tumors are mostly triple negative as backed by our findings 15. Adenomyoepithelioma (AME) of the breast is a rare disease characterized by a bicellular pattern consisting of both ductal and myoepithelial cells. Most of the AME are benign, and only a few will progress to malignancy. Malignant AME has various morphological features and a definitive diagnosis of it is based on immunohistochemical analysis. Owing to the low volume of data on the above tumor its prognostification and status of lymph node metastasis become difficult 16. Our case was basal phenotype without nodal metastasis.
Six month follow up of all the patients were done. Except for the advanced stage metaplastic carcinoma all other patients fared well and were disease free post treatment. However long term followup with close monitoring is needed to conclude on the behaviour of these rare tumors.
Long term followup with close monitoring is not done and this can be considered as one of the limitations of the study. And also, the behaviour of these rare tumors to chemotheraphy has not been studied.
Special and differentiated breast cancers are a heterogeneous group of malignancies with different histomorphological features and prognoses. This study showed the molecular characteristics of rare histological types of breast cancer along with morphological features. Understanding the molecular features of special types of breast cancer will provide newer approaches and areas for study on treatment modalities. We beleive that this study would be an acquaint for future studies about molecular patterns of special type breast tumors. Although the molecular subtyping of these rare tumors were in concordance with established literature few exceptional findings in our study results are noteworthy. Since, these entities are rare conducting prospective studies focusing on rare breast cancers is unrealistic. A more comprehensive study of the clinical and genomic aspects of rare histological subtypes is needed to provide more personalized treatment for patients with special variants and differentiated ductal carcinomas of breast.
Subscribe now for latest articles and news.