Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.2016.v02i02.008
Year: 2016, Volume: 2, Issue: 2, Pages: 41-43
Case Report
Gopya Naik1, Debasubhra Mitra2, Shivakumar Shetty3, C R Raghuveer4
1Professor, Department of Orthopaedics, Adichunchanagiri Institute of Medical Sciences, Mandya, Karnataka, India,
2Junior Resident, Department of Orthopaedics, Adichunchanagiri Institute of Medical Sciences, Mandya, Karnataka, India,
3Professor, Department of Medicine, Adichunchanagiri Institute of Medical Sciences, Mandya, Karnataka, India,
4Junior Resident, Department of Pathology, Adichunchanagiri Institute of Medical Sciences, Mandya, Karnataka, India
Address for correspondence: Dr. Debasubhra Mitra, Department of Orthopaedics, Adichunchanagiri Institute of Medical Sciences, Mandya - 571 448, Karnataka, India. Phone: +91-8861499864. E-mail: [email protected]
Neural fibrolipomas are hamartomas of peripheral nerves. They are benign, usually manifesting as a soft, slowly growing painless fusiform swelling of a segment of peripheral nerve. This condition is common in the upper limb, but the condition is very rare on foot. We hereby report a case of painful neural fibrolipoma of medial branch of the superficial peroneal nerve of the foot. The patient presented with swelling associated with pain. Histopathological examination of the excised specimen showed features of a hamartoma of the nerve.
KEY WORDS:Histopathological examination, medial branch of superficial peroneal nerve of foot, neural fibrolipoma.
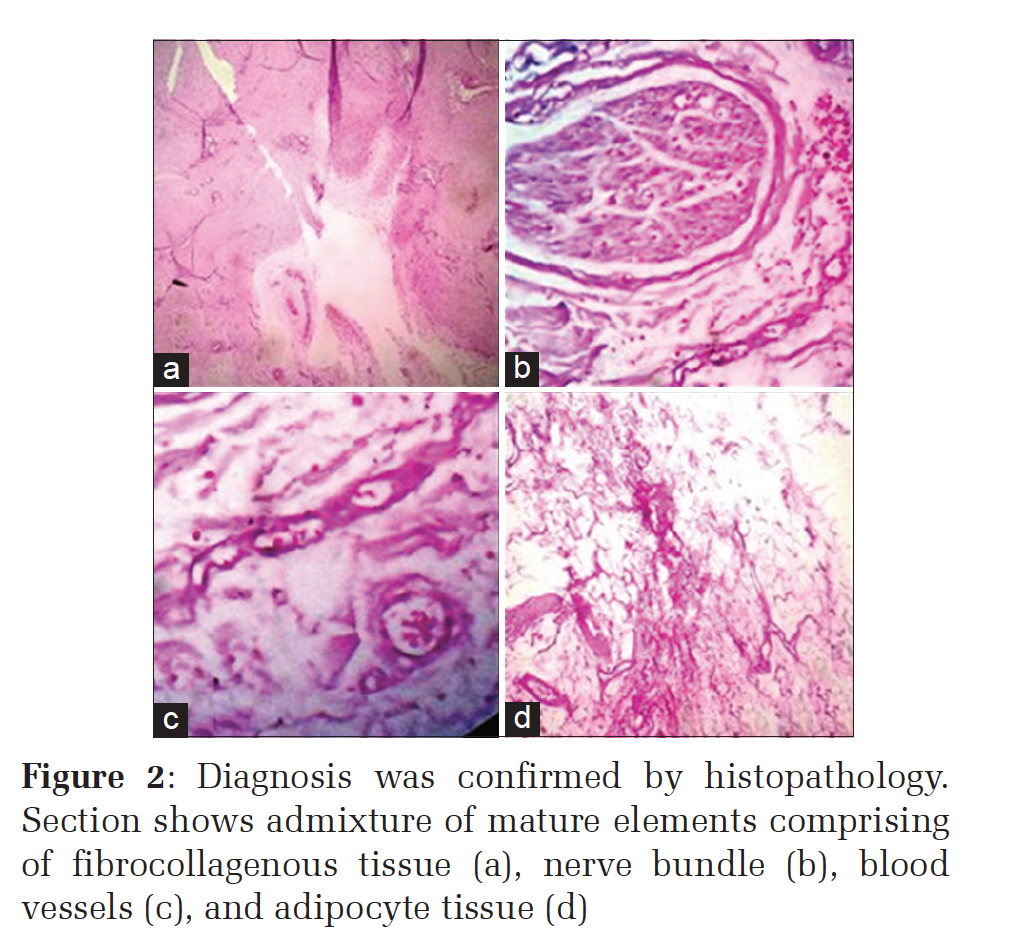
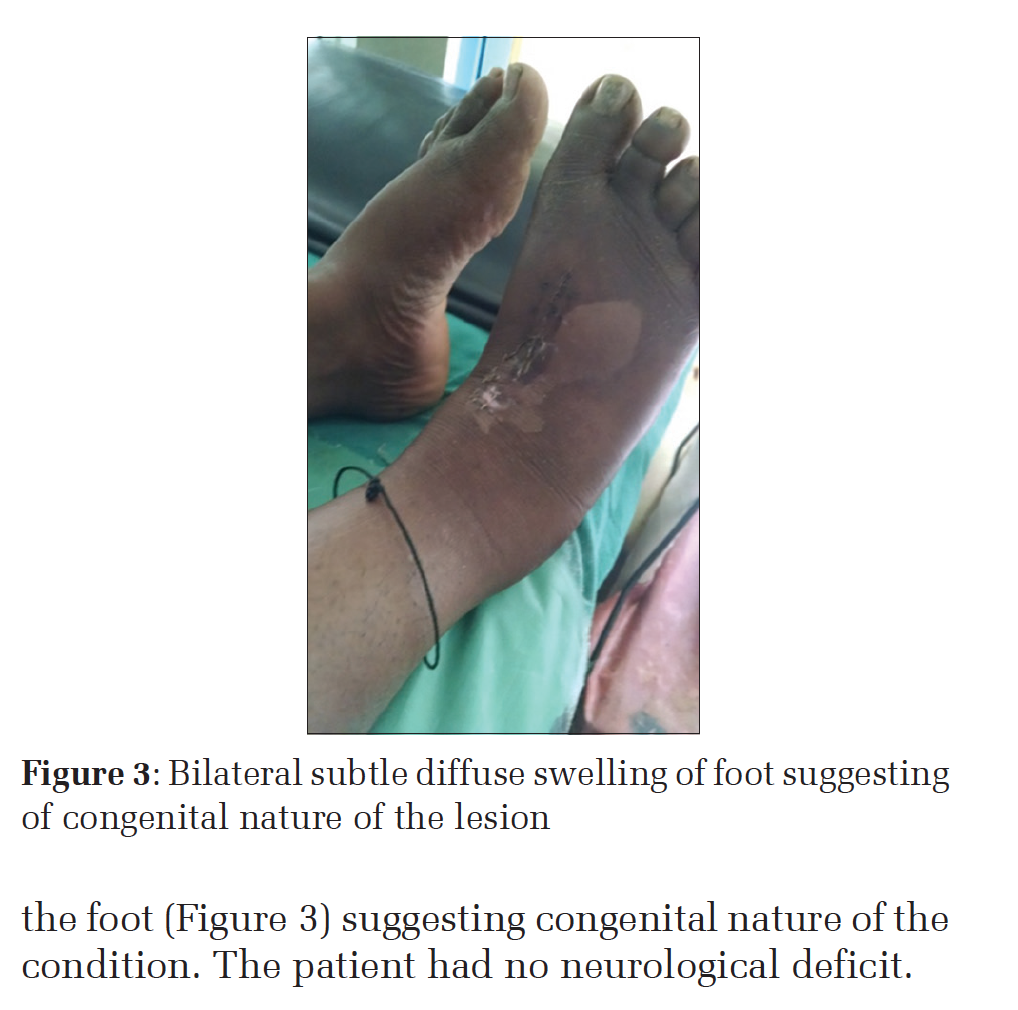
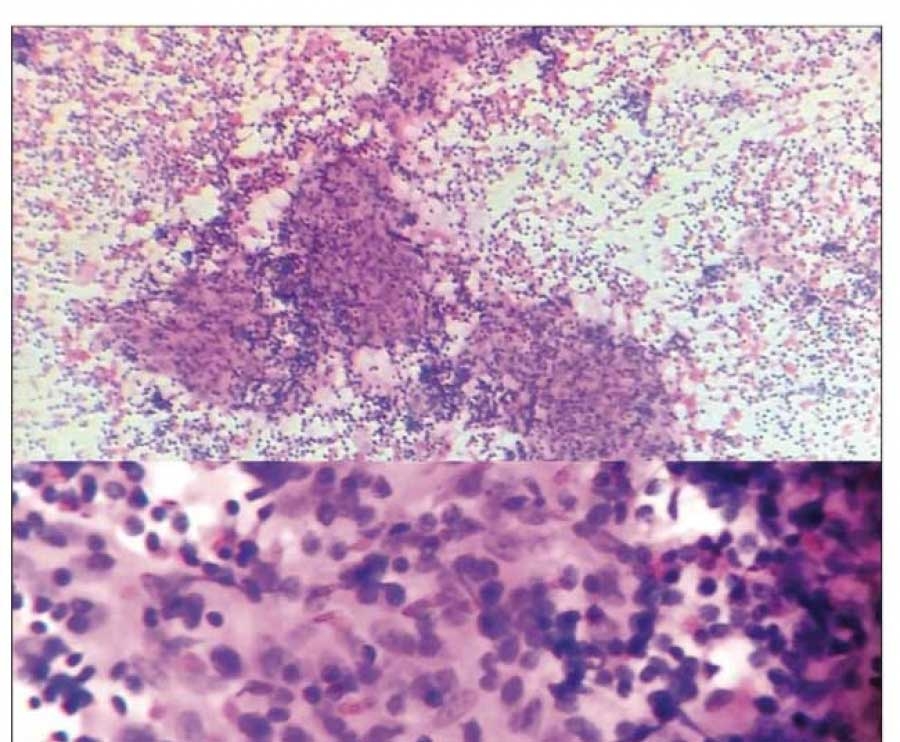
IntroductionNeural fibrolipoma has been called by various names, i.e. fibromatosis of nerve, fibrolipomatous hamartoma of nerve, lipofibroma of nerve, lipomatosis of nerve, and neural lipofibromatosis hamartoma. It has been considered a hamartoma because the fibrous, fatty, and neural components are all essentially mature tissue.[1] Although some consider it to be of congenital origin, the exact etiology remains unclear.[2] Neural fibrolipomas are benign hamartomas that occur as soft tissue swelling in relation to a segment of peripheral nerve.[3] They are fusiform swellings that may or may not move across the peripheral nerve depending on the amount of fibrosis surrounding the swelling. However, they never move along the nerve. If painful they have to be excised, and biopsy confirms the diagnosis. They may be painless also. The histological picture is characteristics. There’s fibrofatty infiltration within the nerve associated with perineural and endoneural fibrosis and thickening of nerve fascicles.[4] The median nerve is most commonly involved followed by the ulnar and radial nerve. Lower extremity cases are extremely rare. Neural fibrolipomas are associated with the overgrowth of bone and macrodactyly in about one-third of cases and are known as macrodystrophia lipomatosa.[5] The differential diagnosis includes ganglion cysts, vascular malformations, traumatic neuroma, and lipomas.[6] Case ReportA 35-year-old female patient was admitted with history of pain in the right foot for 1 year. It was dull aching in nature, gradually progressive. Pain appeared on walking a distance of about 1 km. The pain was relieved on lying down and taking analgesics. She also noticed a swelling on the dorsum of foot 3 months back with gradual increase in the size of swelling. The swelling was associated with pain even at rest. There is no history of trauma or restricted mobility or macrodactyly of toes. Past history, family history, or personal history revealed nothing significant. General examination and laboratory investigations were within normal limits. The systemic examination was unremarkable. On examination, a fusiform swelling in first inter metatarsal space on the dorsum of the right foot was noticed, measuring 3 cm × 2 cm, diffuse border, firm in consistency. The swelling appeared to be prominent on flexing toes against resistance and had limited movement across the nerve. Skin condition was normal, and the skin over swelling could be pinched, swelling was mobile horizontally but not vertically. No neurological deficits were noted. X-ray right foot was normal. A clinical diagnosis of neuroma was made. Ultrasound revealed cystic lesion. Fine-needle aspiration cytology reported it as ganglion. The case was taken for surgery; excision biopsy was done under spinal anesthesia. The removed specimen was a single yellow-white, fibro‑fatty mass of 3 cm × 2 cm, soft to firm in consistency, fusiform in shape. It was engulfing medial branch of superficial peroneal nerve. The swelling was resting on the fascia of first dorsal interossei. The swelling was excised along with the nerve. The specimen was sent for histopathological examination. Macroscopically, the cut surface was gray-white (Figure 1). Microscopically, it showed admixture of mature elements comprising of adipocytes in lobules with interspersed capillary sized blood vessels along with nerve bundles, thick walled blood vessels, and fibrocollagenous tissue (Figure 2). All these features suggested neural fibrolipoma. The wound healed by primary intention. Four months after surgery, the patient had no complaint, no pain, or no significant loss of sensation on foot. The sensation of first interdigital web space was intact. DiscussionNeural fibrolipoma of peripheral nerve was first reported in English literature in 1953. Since then about 100 cases have been documented so far in the available indexed English literature.[7] However, neural fibrolipoma in the foot is very rare. This condition in the foot has to be differentiated from Morton’s metatarsalgia, ganglion, neuroma, neurofibroma, lipoma of nerve sheath, vascular anomaly, neurofibromatosis, and other compressive neuropathy. The combination of a mobile, firm, slowly growing fusiform mass that follows the distribution of a nerve and causes pain only after compression seems to be unique for neural fibrolipoma. In this case, it developed from the medial branch of superficial peroneal nerve of the foot. The majority of cases of neural fibrolipoma presents with a longstanding painless fusiform mass and occurs in adults. Neurological symptoms ensue after several years, mainly due to nerve compression.[8] Compression neuropathy leads to sensory and motor symptoms including pain, tenderness, diminished sensation, paresthesia, and weakness. In our case, the patient presented with pain from the beginning which is unusual presentation of neural fibrolipoma. The patient had bilateral subtle diffuse swelling of the foot (Figure 3) suggesting congenital nature of the condition. The patient had no neurological deficit. The diagnosis is usually made by microscopic findings. The development of neural fibrolipoma includes the proliferation of mature fatty and fibrous tissues within the epineurium and perineurium of a major nerve. The components of the lesion may vary in proportion, thus leading to a variety of histological expression patterns that can make diagnosis difficult. Immunohistochemistry is not essential for diagnosis, although the immunohistochemical profile of a neurofibrolipoma was first reported by Akisue et al. in his case report, in 2002, showing CD34 antigen reactivity on fibrous spindle cells.[9] Several reports have indicated that magnetic resonance imaging may demonstrate the pathognomonic features of neural fibrolipoma, including the serpentine-like appearance of fibroadipose tissue intermingled with nerve fascicles, a coaxial cable-like appearance on axial sections, and a spaghetti-like appearance on coronal images.[10-12] The pathogenesis of neural fibrolipoma is unknown. Some tumors are believed to be congenital without an underlying family history.[13] Antecedent trauma and chronic nerve irritation are regarded as precipitating factors. Neural fibrolipoma can be easily differentiated from neurofibromatosis, in which the painless multiple swellings are present since birth all over the body and which usually shows no growth. The treatment options for neural fibrolipoma are still controversial. They can be treated conservatively or surgically. Surgical treatment options include debulking, external or internal neurolysis, or radical excision with or without fascicular grafts.[14,15] Treatment should be individualized based on the clinical presentation. For neural fibrolipoma causing prominent neuropathy, open biopsy with external nerve decompression can be performed and this may prevent further nerve injury. Nevertheless, for small lesions without neuropathy, excision is the mainstay of treatment. The patient described here had good clinical outcome without complications following excision of the segment of nerve along with swelling. There was no pain and no significant neuro deficit in the follow-up.
|
ConclusionNeural fibrolipoma is one of the uncommon variants of lipoma, presenting with pain and tenderness, maybe associated with paresthesias or loss of function in the area of distribution of the affected nerve. Neural fibrolipoma of foot needs to be differentiated from many conditions of the foot. If the condition is painful, surgical excision is recommended provided the procedure involves negligible morbidity. Longterm follow-up is needed due to the possibility of disease progression or recurrence. |
Subscribe now for latest articles and news.