Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.2015.v01i01.004
Year: 2015, Volume: 1, Issue: 1, Pages: 19-20
Case Report
Thanh Trung Phan1, Rachel Bird2, Andrew Turley1
1 Consultant Cardiologist, Department of Cardiology, The James Cook University Hospital, Middlesbrough, England, United Kingdom,
2 Senior House Officer, Department of Cardiology, The James Cook University Hospital, Middlesbrough, England, United Kingdom
Address for Correspondence:
Dr. Thanh Trung Phan, James Cook University Hospital, Marton Road, Middlesbrough, TS4 3BW, England, United Kingdom.
Tel.: +01-642850850. E-mail: [email protected]
We present here an unusual cause of paroxysmal atrial fibrillation in a 40-year-old Caucasian woman diagnosed years later with echocardiography of a large left atrial mxyoma together with an image of the excised tumor and its histology. This case informs general medical physicians to be aware of uncommon causes of paroxysmal atrial fibrillation and have a low threshold for arranging transthoracic echocardiography not only look for structurally heart disease, but also cardiac tumors during their medical takes.
KEY WORDS: Atrial fibrillation, echo, histology, myxomas, pathology
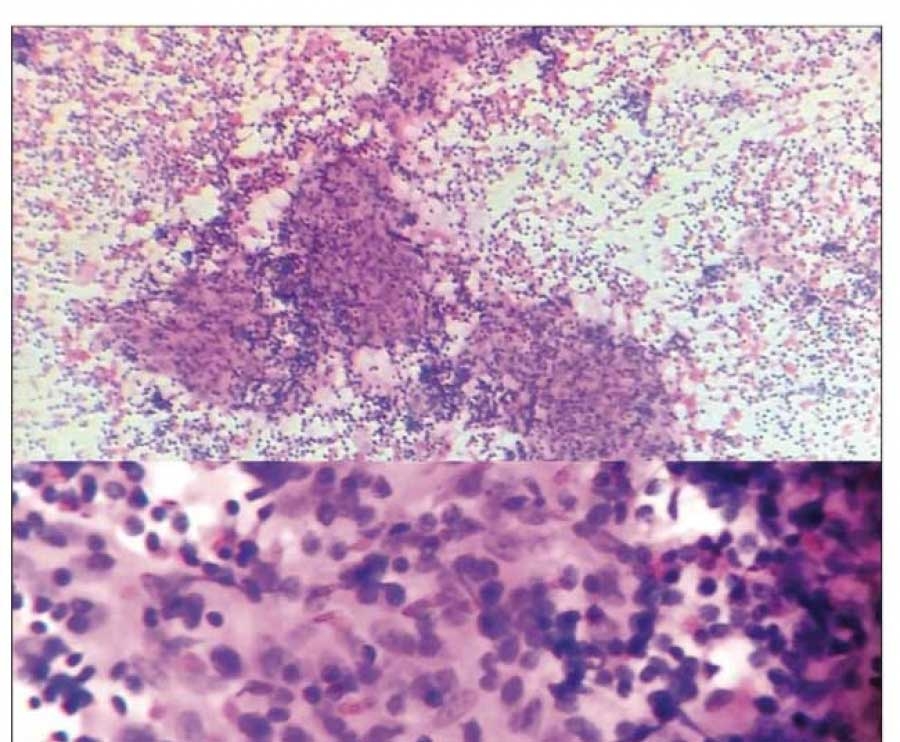
IntroductionAtrial fibrillation is often associated with ischemic heart disease, hypertension, diabetes or other systemic disease such as thyroid disease. However, uncommon causes such atrial myxoms are often overlooked and should be part of one’s list of differential diagnosis. Atrial myxomas are the most common primary cardiac tumor, with higher prevalence in women.[1] Macroscopically they are often pedunculated and arise from the region of the fossa ovalis, with 75% located in the left atrium and 25% in the right atrium. Interestingly, right atrial myxomas are associated with tricuspid stenosis as well as atrial fibrillation.[2] Microscopically, these tumors are benign although local recurrence due to inadequate resection may occur, and they may behave in a malignant manner due to invasion, obstruction of valve leaflets and embolization. |
||||
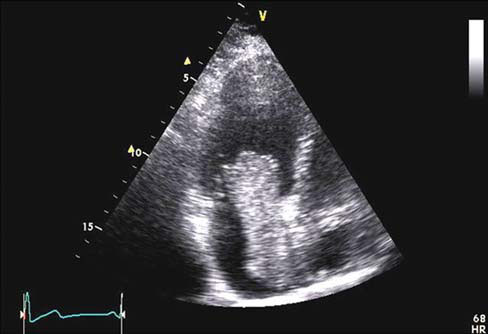
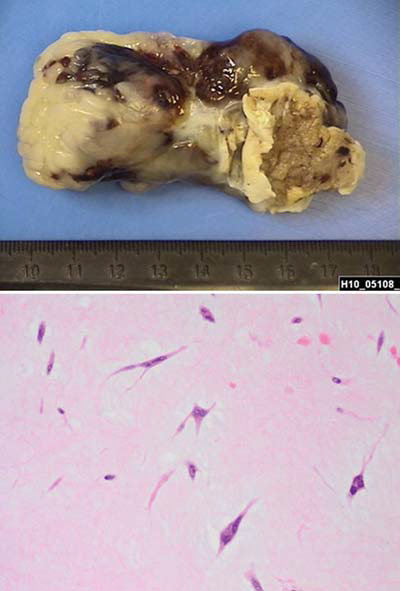
Case ReportA 40-year-old woman presented to the hospital with a 6-h history of palpitations associated with dyspnea and chest tightness. 12-lead electrocardiogram revealed atrial fibrillation, which reverted spontaneously to sinus rhythm, which subsequently settled her symptoms. Clinical examination was unremarkable. It transpired that she has had recurrent episodes of palpitations over the last 7 years, intermittent in nature, irregular and fast with duration up to 12 h. No previous investigations were performed. An echocardiogram was performed. This revealed a large left atrial (LA) mass measuring 7.9 cm × 2.75 cm, which prolapsed through the mitral valve causing significant valvular obstruction (Figure 1). The mass appeared to be attached to the mid portion of the interatrial septum. She subsequently underwent surgery to remove the large LA mass. During the surgery, they found a broad-based myxoma attached to the atrial septum. The tumor was excised completely with the septal defect repaired with an autologous pericardial patch (Figure 2). |
||||
|
||||
DicscussionCl inical presentation depends on the size, location and mobility of the tumor. Well-recognized presentations are with systemic embolization, conduction disturbances and valve obstructions, which can result in sudden death. Transthoracic echocardiography is often diagnostic.[3] The rate of growth is unknown with the mainstay of treatment being surgery as was with this case.[4] The risk of operative mortality is < 5% with a risk of recurrence in the order of 5% and therefore follow-up is required. The risk of recurrence is higher in the familial myxoma syndrome.[5] Learning point for clinicians Th is case informs general medical physicians to be aware of uncommon causes of paroxysmal atrial fibrillation and have a low threshold for arranging transthoracic echocardiography to not only look for structurally heart disease but also cardiac tumors during their medical takes. |
||||
Authors’ ContributionsTTP and RB were major contributors in writing the manuscript. All authors read and approved the final manuscript. |
||||
AcknowledgmentsWe would like to thank Dr. Paul Travado for providing the histology pictures. |
Subscribe now for latest articles and news.