Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.2021.v07i03.009
Year: 2021, Volume: 7, Issue: 3, Pages: 39-44
Original Article
Haradanahalli Giriprakash Kshamaa1, Lakshmi V Pandit2,Padmanabha Thiruganahalli Shivaraju3, Manju Aswath4
1Assistant Professor, Department of Psychiatry, Kempegowda Institute of Medical Sciences, V V Puram, Bangalore, 560004, Karnataka, India,
2Professor and Head, Department of Psychiatry, Kempegowda Institute of Medical Sciences, V V Puram, Bangalore, 560004, Karnataka, India,
3Associate Professor, Department of Pharmacology, Adichunchanagiri Institute of Medical Sciences, Adichunchanagiri University, B G Nagara: 571448, Mandya, Karnataka, India,
4Professor, Department of Psychiatry, Kempegowda Institute of Medical Sciences, V V Puram, Bangalore: 560004, Karnataka, India
Address for correspondence:
Manju Aswath, Professor, Department of Psychiatry, Kempegowda Institute of Medical Sciences, V V Puram, Bangalore: 560004, Karnataka, India. E-mail: [email protected]
Background: Clozapine is a gold standard drug in the armamentarium of treatment for resistant schizophrenia. Despite being advantageous in several ways, it is said to be underutilized by psychiatrists world over, more so in India, due to its side effect profile and the nature of monitoring required. Aims: To assess the pattern of use of clozapine in patients diagnosed with schizophrenia in a psychiatry unit of a tertiary care hospital. Methods: Charts of all patients who received a diagnosis of schizophrenia at the psychiatric unit in Kempegowda Institute of Medical Sciences, Bangalore over the past five years were reviewed. Those individuals who received clozapine were assessed for pattern of use of the drug. Results: A total of 120 charts of patients with schizophrenia were assessed, of which 19 received clozapine. Patients with a continuous course of illness, or non-responsive to two or more antipsychotics were found to receive clozapine. Conclusion: Clozapine is more likely to be used in treatment resistant cases with a chronic course of illness. Pattern of usage of clozapine remains the same in tertiary care setting.
Keywords: Clozapine, retrospective study, schizophrenia
Clozapine has been found to be an effective atypical antipsychotic since the time of discovery[1] . However, it was withdrawn from the market in 1976 as there were many reports of fatal agranulocytosis as one of the side effects[1] . Studies later on showed its effectiveness in treatment-resistant schizophrenia, suicide prevention & low propensity for extra pyramidal symptoms when compared to other antipsychotics and hence paved the way for its reintroduction[2,3] . It has also been found that patients on clozapine had lower discontinuation rates, were less likely in need to switch antipsychotics orpolypharmacy[4] , and had decreased relapse rates[5] . The only aspect to be kept in mind in these individuals is regular monitoring of blood parameters for agranulocytosis.[6] .
“Current clinical practice guidelines define treatment-resistant schizophrenia as failure to respond to adequate trials with two unrelated antipsychotics (at least 1 of which should be a non-clozapine second-generation antipsychotic such as risperidone, olanzapine, or quetiapine)”[7–9] .
The need for regular blood tests and distressing sideeffects such as excessive sedation hyper salivation, metabolic syndrome and rarely, risk of myocarditis and cardiomyopathy has been a major concern while prescribing, which in-turn has led to underutilization of this drug[10] .
Studies in India have shown significant improvement in schizophrenics on clozapine, who had previous history of minimal response to other
anti-psychotics. Further, the incidence of serious side effects such as agranulocytosis and seizure are rare[11] .
In this context, the current study aims at analyzing the pattern of use of clozapine in our hospital.
This cross-sectional retrospective study, conducted after obtaining ethical clearance from the Institutional Ethical Committee, included all outpatients (aged 15–64 y) attending a tertiary heath care in the Bangalore between October 2011 – October 2016. Only subjects with a diagnosis of schizophrenia who were prescribed clozapine were included in this analysis (n= 120).
Study data were extracted from the clinical file used at the tertiary heath care center. Data were entered into a custom-designed Microsoft Access database with predetermined response options to ensure data quality and facilitate analysis. Data collected included demographics (sex, age, ethnicity, principal diagnosis, co morbid conditions, duration of mental illness (time, in years, from first contact with a treatment provider until 2015), psychiatric admission history, and treatment data (current and past psychotropic medication history, with total daily dose and route of administration). The principal Axis I diagnosis (International Classification of Diseased 10) documented at the psychiatric assessment closest to October 31, 2015, was recorded as the major mental disorder. Axis I and II co morbidities were recorded if documented at the psychiatric assessment closest to the study review point.
All psychotropic data (including antipsychotics, antidepressants, mood stabilizers, sedative– hypnotics, and drugs used for management of neurologic adverse effects of antipsychotics) were recorded from the medication chart. Information about the type and number of antipsychotics prescribed prior to clozapine was collected. If the drug was used more than once, it was counted as a single antipsychotic treatment.
Inclusion criteria: all patients attending out-patient department in KIMS from 2010 – 2015 diagnosed with schizophrenia according to ICD 10 criteria, who had been administered clozapine.
Exclusion criteria: Patients with other co-morbid Axis I diagnosis, patients with schizo-affective disorders.
Data analyses were conducted using SPSS version 20.
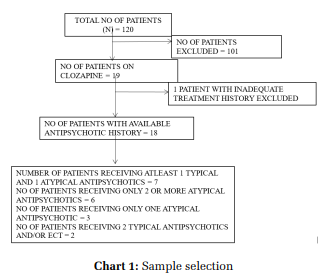
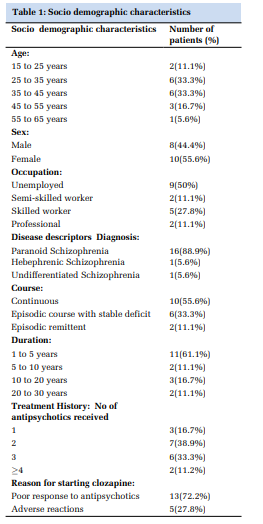
In our tertiary care hospital, in past 5 years, 120 patients received treatment for schizophrenia of which 19 patients (9.5%) were started on clozapine. Among the patients prescribed clozapine 53% were females & 47% were males, in the age group of 25 – 45 years with average age being 36 years. On an average, patients prescribed clozapine were unwell for approximately 5 years. 16 patients were diagnosed with paranoid schizophrenia, 2 with undifferentiated schizophrenia and 1 with hebephrenic schizophrenia. However, 1 patient was excluded from the study due to non - availability of treatment data. [Chart 1]
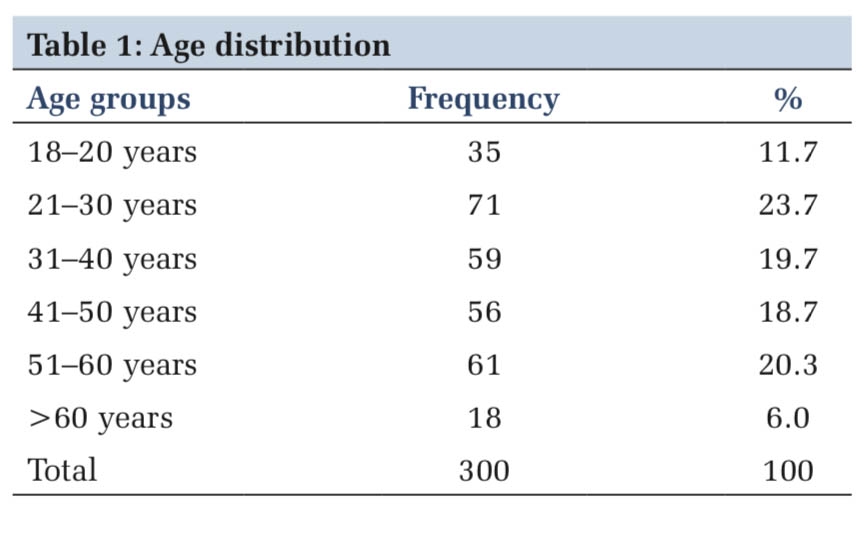
Entire group had data that allowed calculation of duration of contact with treatment provider and clozapine starting year. Among these patients 63% were started on clozapine within 5 years of contact with the treatment provider. No significant difference was found in patient’s age or gender in pre-clozapine treatment duration. [Table 1]
Of the 19 patients 1 patient was lost for follow-up after initial contact. Data of 18 patients was available to analyze history of previous antipsychotics. These patients received an average of 2.28 antipsychotics before starting clozapine (median – 2, SD – 1.447,range – 1-6).
8 among the 18 patients (44%) had received at least one typical antipsychotic, among who 3 received depot antipsychotic. Among them 5 patients (62.5%) required adequate trial but showed poor response to typical antipsychotic. In 3 patients’ antipsychotic was changed due to development of adverse effects (dystonia / EPS).
15 of the 18 patients (83.3%) had received at least one second generation antipsychotic, 10 of whom received adequate dosage but showed poor response to medication. 7 patients developed adverse reaction to atypical antipsychotics, most common being dystonia and akathisia.
Three of the patients receiving clozapine were started on the drug following only one trial of an atypical antipsychotic drug. Among these patients one patient was previously started on risperidone 8 mg given for three months, showed partial response but developed drug induced parkinsonism and hence started on clozapine. One patient was started on paliperidone 9mg, which was given for one month. The patient developed severe anti-cholinergic side effects and extra pyramidal symptoms of tremors and rigidity, with inadequate response to medication, and hence clozapine was started. The third patient was previously treated with amisulpiride 200mg for 2 weeks, and developed rigidity, resulting in clozapine as a choice for treatment.
In summary, the most common reason for starting clozapine in 18 patients was an inadequate response (72%), followed by adverse reactions to previous antipsychotics (28%).
Literature has shown that clozapine use has resulted in significant improvement in positive symptoms, some improvement in negative symptoms as also a reduction of drug induced side effects like Tardive dyskinesia and Extra pyramidal symptoms[12] . It was effective in both paranoid and catatonic schizophrenia, as well as residual schizophrenia, with improvement in symptoms of disorganization[13] . The drug has mostly been started in patients with a mean duration of illness of 10 years[14] .
Most of our study sample who received clozapine were diagnosed to have paranoid schizophrenia (89%), with a continuous course of illness (55%) and a total illness duration averaging 5 years before clozapine administration. These patients were, on an average, on 2.28 antipsychotics before prescribing clozapine. This is in keeping with the world trend of a reported range of 2.8 – 4.3[14–16] .
The available treatment guidelines for management of schizophrenia recommend that clozapine be started after two failed trials with antipsychotic agents (either typical or atypical)[8,17–19] . In our patient population 83.3% of the patients received an adequate trial of at least 2 antipsychotics before starting clozapine. In a previous Indian study by Grover et al., who conducted a retrospective chart review of 200 patients receiving clozapine in a tertiary health center, it was found that 6.5% of them received clozapine due to the side effect profile or poor response. More than 50% of the patients in this study were diagnosed to have paranoid schizophrenia, with a mean duration of illness of 10.8 years, and had responded poorly to adequate trials of antipsychotics (85.5%)[14] . On similar lines, the subjects of the current study were initiated on clozapine due to an inadequate response to treatment with other antipsychotics (72%), and hence received clozapine earlier in the course of illness than in other studies[14] , as well as their side effect profile. In the recent past, there have been different schools of thought on when to initiate clozapine. Many researchers are exploring the use of clozapine as a first line drug in the treatment of schizophrenia. This is based on the following facts - The CUtLASS study manifests a better clinical response - in terms of global psychopathology, improvement in the quality of life and a better degree of satisfaction of patients on clozapine as opposed to those on other atypical antipsychotic drugs. The greater clinical efficacy of clozapine is with regard to the positive symptoms[20] as well as the cognitive ones. Clozapine is known to have low extra-pyramidal side effects and low tendency to elevate prolactin. It has also been shown to diminish the rate of hospitalization[21] . In the CATIE study, the mean time to discontinuation of drug treatment for clozapine was 10.5 months versus 3.3 of quetiapine, 2.8 of risperidone and 2.7 of olanzapine.
In the only randomized clinical trial up to date with clozapine in first psychotic episodes without previous pharmacological treatment, Lieberman JA et al.[22] compared the efficacy of clozapine and chlorpromazine (plus benzatropine). The patients were maintained under treatment with the drug assigned, with double-blind conditions, for two years (or until the clinical conditions led to a switch in therapeutic regimes), completing a total followup period of 9 years in an open study. Of the 2708 patients screened, 160 (80 in each group) were enrolled in the trial. In all, 15% of the patients assigned to clozapine and 22.5% of those assigned to chlorpromazine did not complete the study. Remission rate was 81% in the clozapine group and 79% in the chlorpromazine one. However, remission was achieved in a lesser period in the clozapine group (50% of the patients with clozapine had remitted in 8 weeks versus 12 weeks in the patients with chlorpromazine), with the rate being almost twice in the clozapine group than in the chlorpromazine one. Once remission was achieved, the patients assigned to clozapine remained in remission almost twice the time as those assigned to chlorpromazine. The likelihood of remaining in remission was reduced by 15% for each additional year of psychosis without treatment.
Despite the overwhelming evidence of the superior efficacy and effectiveness of clozapine compared to other antipsychotics in treatment-resistant schizophrenia, clozapine is prescribed infrequently by clinicians. To date, there have been few empirical investigations of the reasons for the infrequent use of clozapine,[23]
, although possible explanations include its strict hematological monitoring requirements and the potential for serious side effects including agranulocytosis, myocarditis, other inflammatory reactions, seizures, sedation, weight gain, diabetes mellitus and other metabolic abnormalities.[24,25] Other possible explanations include lack of knowledge about the benefits of clozapine, or negative attitudes towards the medication among physicians, patients and families.[26] More aggressive marketing of other second-generation antipsychotic medications by pharmaceutical companies may also contribute to the infrequent use of clozapine.[27] Limitation of our study is sample size being small.
Subscribe now for latest articles and news.