Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.2021.v07i01.003
Year: 2021, Volume: 7, Issue: 1, Pages: 16-20
Original Article
Sonali Banwait1, Madhu Gupta2
1Department of Anaesthesia, Vardhman Mahavir Medical College and Safdarjung Hospital, New Delhi, India,
2Department of Anaesthesia, Employee’s State Insurance Hospital, Basaidarapur, New Delhi, India
Address for correspondence:
Dr. Sonali Banwait, Department of Anaesthesia, Vardhman Mahavir Medical College and Safdarjung Hospital, New Delhi, India. Phone: +91-9811783404. E-mail: [email protected]
Introduction: Patient satisfaction is an important goal of health-care services and involves various aspects health-care delivery. Dissatisfaction expressed by patients’ compromises health-care delivery taking a toll on the both human resources and infrastructure. Perioperative care is an important aspect of healthcare delivery. Various validated questionnaires have been constructed to evaluate patient satisfaction. We undertook a study to measure perioperative patient satisfaction using Leiden perioperative care patient satisfaction questionnaire.
Objectives : The aim of this study was to assess perioperative patient satisfaction using a validated and structured questionnaire.
Methods We conducted this prospective cross-sectional observational study with Leiden perioperative satisfaction questionnaire translated to Hindi. The questionnaire had a total of 39 questions covering various dimensions such as information provided, side effects, fear and concern, staff-patient relationship, professional competence, and services received.
Results: Our results showed almost equal satisfaction among males and females. Demographic factors did not play a major role in patient satisfaction. Vomiting was the most common side effect observed in both general and regional anesthesia followed by hunger, which resulted in dissatisfaction. However, staff-patient communication and relationship with regard to information received by patient and fear and concern about surgery and anesthesia resulted in dissatisfaction.
Conclusions: Our study highlighted the communication barrier between health-care professionals and patients resulting in dissatisfaction. Thus, health-care providers need to be more sensitive to the emotional and mental health if the patients in the perioperative period.
KEY WORDS:Perioperative care, patient satisfaction, questionnaire
Patient satisfaction is defined as the patient’s reaction consisting of a “cognitive evaluation” and “emotional response” to the care, they receive.[1] For health- care providers, patient satisfaction is important as it helps to know the actual impact of health-care processes on the patients themselves.
Satisfaction comprehends various aspects of patient’s behavior, such as global consumption of health-care resources, compliance with treatments, or steadiness of relationship with practitioners.[2,3] If the patient experiences a discrepancy between expected and provided health-care service, a feeling of dissatisfaction arises which ultimately results a compromised health- care delivery.
Patient satisfaction helps in the tracing and correction of health-care system impotencies and problems. This approach helps to meet patients’ desires and expectations, thus resolving their speculations. Thus, this study helped us to know efficacy of our perioperative care, our patient’s level of expectations and helped to improve our perioperative care.
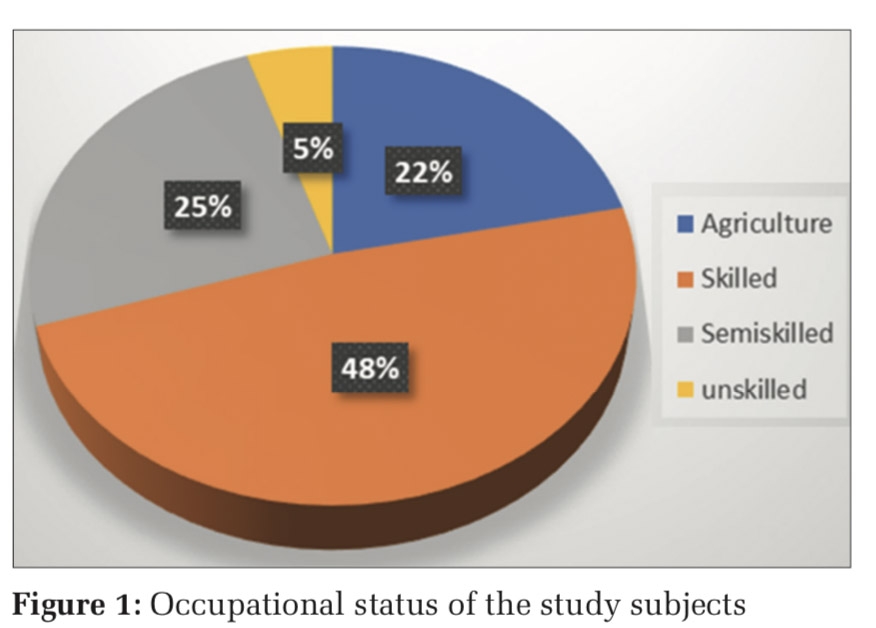
Our hospital comes under employee state insurance scheme (ESI) of India, which is a social security scheme tailored to provide protection to workers and their dependants in contingencies such as sickness, maternity, and death or disablement due to occupational hazards. The employee and employer do the contribution for the finances of the ESI scheme. ESI scheme has the Motto insured person (IP) is very important person (VIP) (IP is VIP). Thus, it is imperative that the medical services tendered meet the satisfaction level of the patients.
Perioperative patient satisfaction has been measured in various studies in different countries with various validated questionnaire such as Iowa satisfaction with anesthesia scale,[4] Evaluation du Vécu de l’Anesthésie Générale,[5] The Leiden Perioperative care Patient Satisfaction questionnaire (LPPSq),[6] and Heidelberg Perianesthetic questionnaire.[7] Sarah et al.[8] have reviewed LPPSq and Heidelberg questionnaire as a research tool for perioperative patient satisfaction. Pilot study done in our institution with both these questionnaires resulted in highly acceptable responses from our patients with LPPSq.
LPPSq is a validated tool measuring various aspects of perioperative patient satisfaction such as information, discomfort and needs, fear and concerns, staff-patient relationship, and services.
The aim of our study was to assess patient satisfaction in the Indian scenario with a structured and validated questionnaire. Due to increasing awareness among patients, we undertook this observational study as means to improve our existing perioperative care.
We conducted this prospective cross-sectional observational study with Leiden perioperative satisfaction questionnaire translated to Hindi. The English questionnaire, translated by a bilingual researcher into Hindi, was administered to 10 individual patients to reach a consensus between the two versions. The Hindi version administered to 25 random patients, that is, ruled out any problem with its comprehensibility as all the patients understood and answered the questionnaire. The questionnaire had a total of 39 questions covering various dimensions such as information provided, side effects, fear and concern, staff-patient relationship, professional competence, and services received.
The Institutional Ethical Committee approved the study. Patients older than 18 years with literacy in Hindi language were included in the study. Patients undergoing elective surgery in surgical specialties (general surgery, ear nose throat, orthopedics, gynecology, and urology) were included in the study. The study was explained to patients’ with an assurance of confidentiality and voluntary participation. On the day of surgery, in the pre-holding area, patients who fulfilled the inclusion criteria were included in the study. The patients’ were sequentially given the questionnaire but only completed questionnaires were included in the study. An independent registrar administered and collected the questionnaire next day after the surgery.
Statistical analysis
Statistical Package for the Social Sciences system version 17.0 was used for statistical testing. Continuous variables are presented as mean ± standard deviation (SD) or median interquartile range for non-normally distributed data. Categorical variables were expressed as frequencies and percentages. Reliability was assessed by Cronbach’s α, inter-item correlation, and item discriminant validity. By definition, a Cronbach’s α from 0.61 to 0.80 represents a substantial correlation and from 0.81 to 1.00 a good correlation.
The inter-item correlation describes the Spearman rank correlation between items scores and their dimension score. Each item was correlated with their own dimension. The item discriminant validity describes the Spearman rank correlation between item scores of a given dimension with the other dimensions. Normally distributed continuous variables were compared using the unpaired t-test (for two groups) and ANOVA (for 3 or more groups), whereas the Mann–Whitney U-test and Kruskal– Wallis test were used for non-normally distributed data. Categorical variables were analyzed using either the Chi-square test or Fisher’s exact test.
For all statistical tests, P < 0.05 indicated a statistically significant difference. For the purpose of sample size calculation, patient satisfaction with perioperative care was expressed by the total LPPSq score. With reference to the study by Jhala et al.,[7] the mean total LPPSq score was found to be 96.8 with a SD of 7.29.
Considering the same mean, with a 20% SD of mean within two precision error of estimation, 300 cases are needed at an alpha level of 0.05. Factoring a dropout/refusal rate of approximately 15%, we calculated that 350 patients would be required.
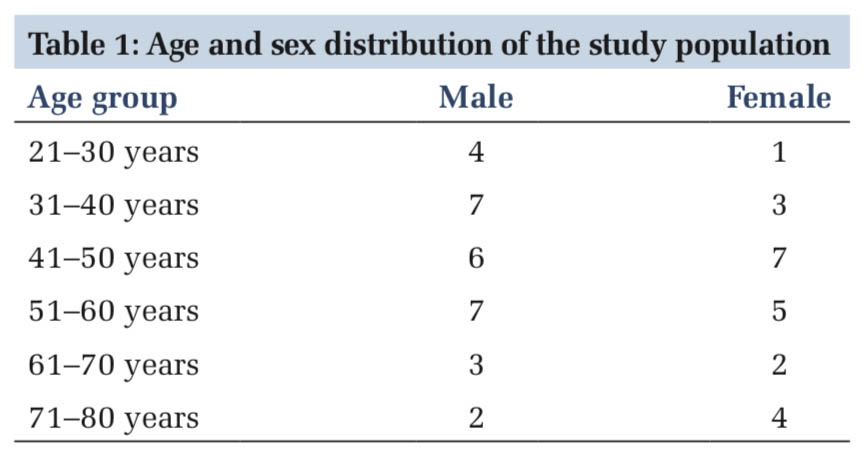
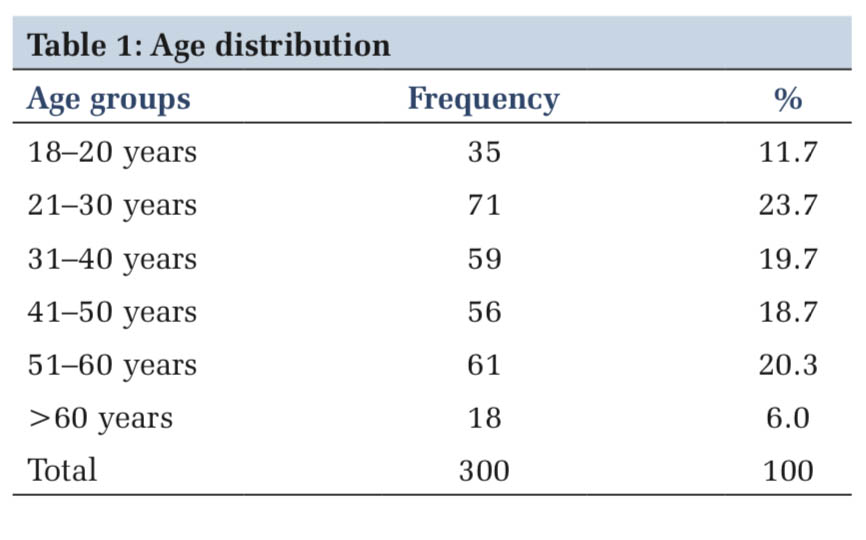
A total of 360 patients over a period of 6 months were enrolled in the study and 300 patients returned fully filled questionnaire. Table 1 depicts age-wise distribution.
The mean age of patients was 40 years. Patients older than 50 years were more satisfied than with age < 50 years (P = 0.044).
Male-to-female ratio was similar (50%). Out of 300 patients, 78% were married while 3% of patients had experienced death of a spouse. In terms of literacy, 58% of patients were high school pass and around 32% had completed secondary school. The mean satisfaction score for females was 105 while for males was 107, it was statistically insignificant (P < 0.44), implying gender had no influence on patient satisfaction level. According to marital status and education, the mean LPPSq was statistically insignificant, 0.595 and 0.154, respectively.
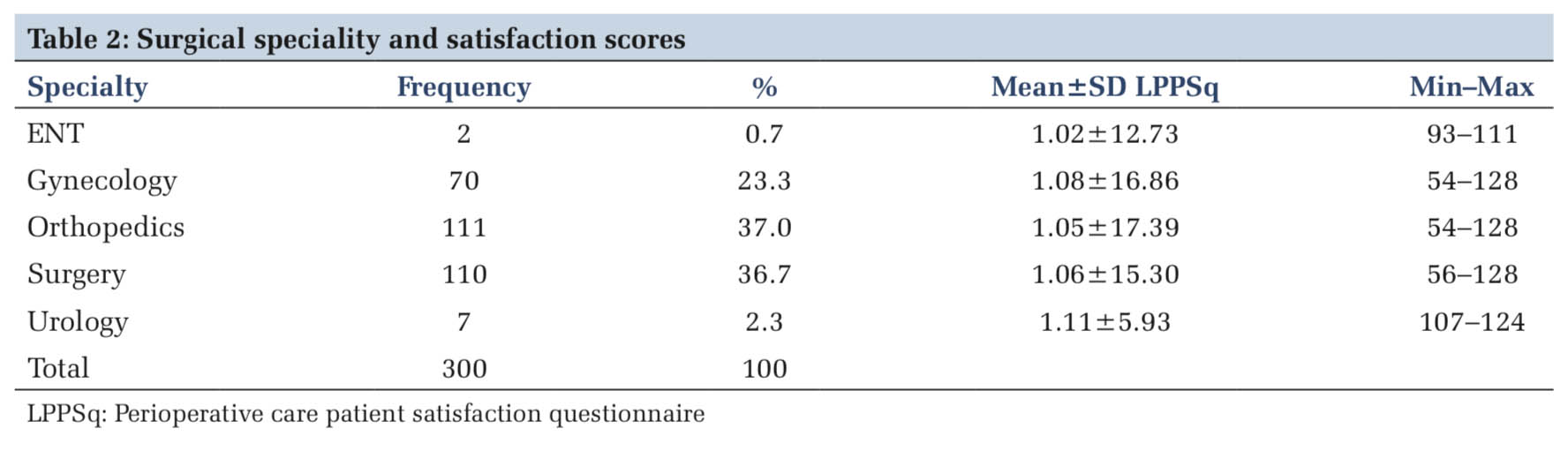
Table2 shows patients’ distribution according to surgical specialty. Surgical specialty did not influence patient satisfaction (P = 0.748). Out of 300 patients, 59% were administered regional anesthesia while 41% received general anesthesia. The type of anesthesia had did not have any effect on perioperative satisfaction score (P = 0.133).
With regard to the American Society of Anesthesiologists (ASA) grading, ASA Grade I patients were 246 and ASA II were 54. ASA Grade II patients were more satisfied than ASA Grade I patients (P = 0.018).
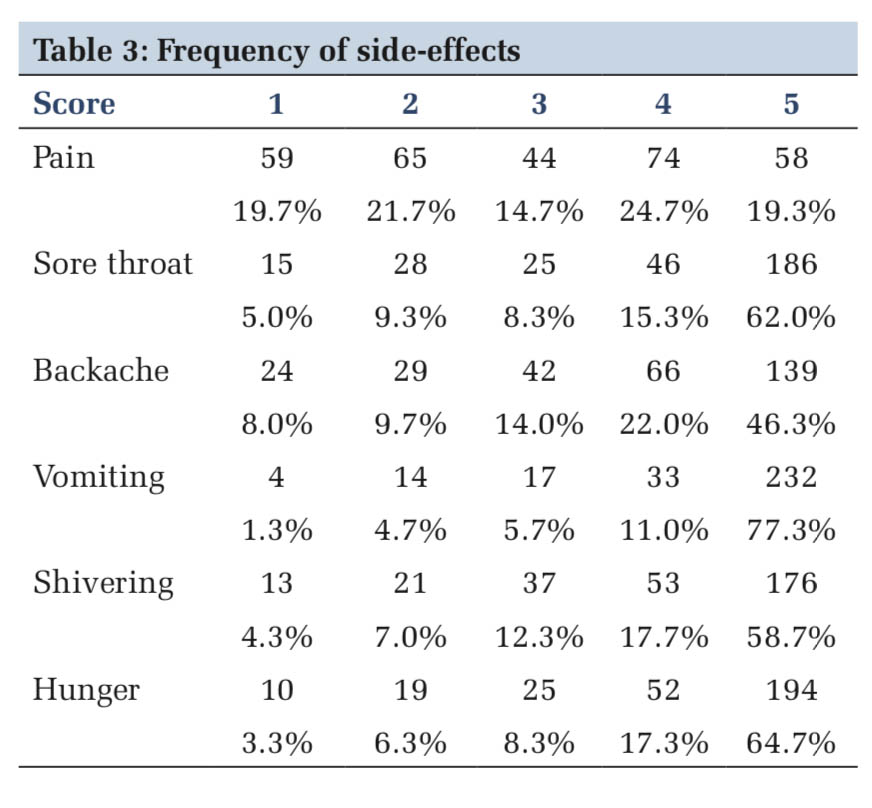
Previous history of any surgery (P = 0.075) and pre-operative administration of premedication (P = 0.628) were found to have no effect on the perioperative satisfaction levels of patients. Table 3 shows the frequency of side effects in patients.
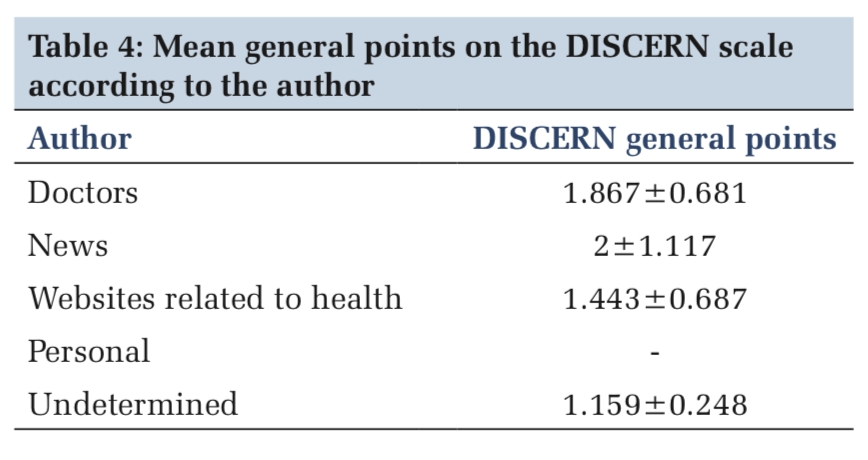
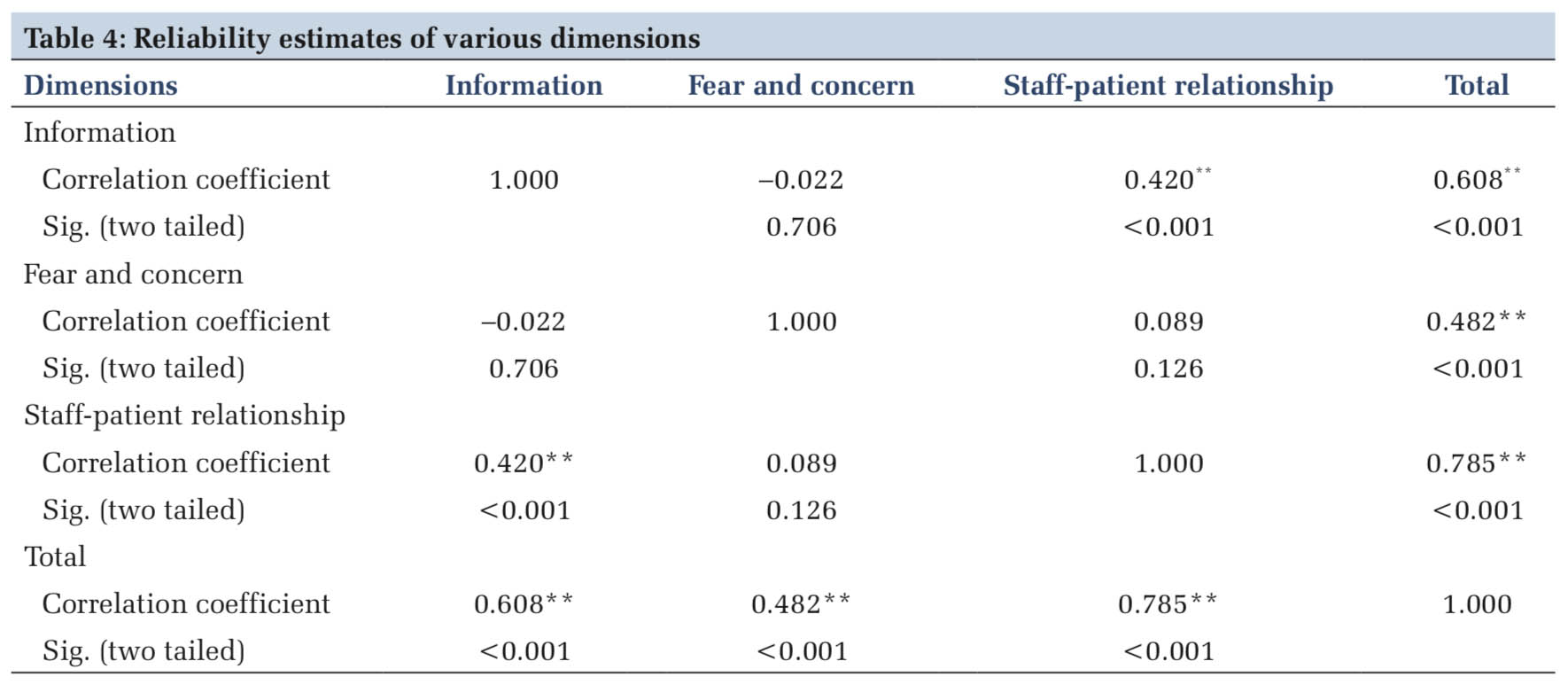
Among the severity of side effects, vomiting was most common complaint of patients followed by hunger. Pain was the least common side effect. Under both general and regional, anesthesia vomiting was most common side effect while pain was the least common one, both being statistically insignificant. Table4 depicts that the correlation coefficient regarding information, staff-patient relationship, and fear and concern was statistically significant with sig. (two tailed < 0.001).
The major factors contributing to dissatisfaction among patients were information received with regard to anesthesia and surgery, not allaying their fear and concerns regarding perioperative period and the staff-patient relationship.
Patient satisfaction is an important measure for the health-care provider to improve patient outcome. Any level of patient dissatisfaction reflects the goal of health-care services is lagging. Patient satisfaction has not been measured by a validated questionnaire in the Indian scenario.
The Hindi translated version of LPSSq comprehensively measured all aspects of perioperative care and was easily comprehended by the patients. The response rate was 83% with equal male-to-female participation. This was higher than the response obtained in studies by Fung et al.[9] (71%) and Whitty et al.[10] (73%). Administration and collection of the questionnaire by the same investigator have resulted in higher participation.
The mean satisfaction score for male and female patients was similar. In our study, demographic factors such as gender, marriage, and education did not contribute to dissatisfaction. With regard to age, patients more than fifty years old were more satisfied. Kouki et al.[11] showed no difference in satisfaction levels with age, sex, and education level. In a systematic review of patient satisfaction, Wu et al.[12] found that increasing age and female gender had increased satisfaction levels.
Furthermore, patients had similar satisfaction experience across various surgical specialties. In the study by Caljouw et al.,[5] age, gender, and specialty had an impact on satisfaction level. With respect to the type of anesthesia administered, whether general or regional satisfaction scores were similar which mirrored study by Jlala et al.[13]
In our study, history of previous surgery and premedication did not affect the satisfaction scores. As ASA II patients, required preoperative optimization with multiple pre-anesthesia visits the satisfaction level between ASA II patients and I was statistically significant. This was in contrast to a study by Heidegger et al.[14] showed that ASA grade had no effect on overall satisfaction levels. Vomiting was the most common side effect observed in both general and regional anesthesia followed by hunger. Vomiting was also most severe side effect complained by patients across general and regional anesthesia. In a study by Kouki et al.,[11] shivering was the predominant side effect and that pain had least impact on satisfaction levels. Jlala et al.[13] reported pain and thirst as major side effects in both regional and general anesthesia while Caljouw et al.[6] also reported pain as a major side effects with increased frequency in general anesthesia.
There was dissatisfaction among patients with respect to information received and staff-patient relationship that implies that there is a communication barrier still exists between health-care professionals and patients and needs to improve upon. The patient also expressed dissatisfaction with regard to fear and concern regarding undergoing anesthesia and surgery. This concurred with the study by Ebremedhn et al.[15]
that communication in the pre-operative visit was key in allaying fear about surgery and anesthesia. Fung et al.[16] found that communication with the hospital staff was key to obtain higher satisfaction levels among patients. Myles et al.[17] too reported that patient-staff interaction is the key to obtain higher satisfaction scores. Capuzzo et al.,[18] in their study, inferred that having dedicated perioperative nursing had profound effect on patient satisfaction. Thus, as health-care providers, we need to be more sensitive to the emotional and mental health of the patients in the perioperative period.
Our study did not include patients who underwent monitored anesthesia care, surgeries under local anesthesia, or had day care procedures. Therefore, a certain subset of patient population was excluded in our study.
Our study highlighted that the side effects relating to anesthesia and surgical procedures do not have much bearing on overall satisfaction scores. The lacunae in giving information to patients regarding anesthesia and surgery are a major cause of dissatisfaction among patients. Communication skills of health care workers and building of a rapport are key to achieve satisfaction amongst patients. Thus, as health-care professionals, we should address the emotional and mental well-being of the patients. Thus, our study pointed out the lacunae in our perioperative health- care services and the various aspects, which need to be addressed to improve health-care delivery.
Thus, we conclude that patient satisfaction is governed by various dimensions which includes emotional, cognitive and social needs. Ideal healthcare will be achieved when the healthcare services and workers address all aspects of patient well-being.
Subscribe now for latest articles and news.