Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.2019.v05i01.009
Year: 2019, Volume: 5, Issue: 1, Pages: 47-49
Case Report
Archana A Randale, Sanjay N Parate, Milind A Bhatkule, Saroj A Meshram, Shilpa P Tathe
Department of Pathology, Government Medical College and Super Speciality Hospital, Nagpur, Maharashtra, India
Address for correspondence:
Dr. Archana A Randale, C/o B C Narnaware, 4B, Jeevan Jyoti Apts, Rahate Colony, Wardha Road, Nagpur - 440 010, Maharashtra, India. Phone: +91-9860130404. E-mail: [email protected]
ABSTRACT: Mature cystic teratomas (MCTs) (dermoid cyst) make up almost 20% of all ovarian neoplasms and 88% are unilateral. They constitute the most common ovarian tumor in childhood. However, it is sparsely seen in postmenopausal woman. Malignant transformation is seen in approximately 2% of all cases of MCT and risk gets doubled in postmenopausal woman. Here, we present a case report of MCT occurring in postmenopausal multiparous woman masquerading as lithopaedion on imaging which is a rare phenomenon. Thus, the mystery behind Monsters egg is finally resolved by morphology.
KEY WORDS:Lithopaedion, mature cystic teratoma, postmenopausal woman, postmenopausal woman
Mature cystic teratomas (MCTs) make up almost 20% of all ovarian neoplasms. In classic type, ectodermal derivatives are seen in 100% of the tumors, mesodermal in 93% and endodermal derivatives in 71% of the cases.[1] Ectodermal origin derivatives most commonly found are skin, hairs, hair follicle, and sebaceous or sweat glands. Hence, it is also called as dermoid cyst. They constitute the most common ovarian tumor in childhood.[2,3] It is sparsely seen in postmenopausal woman.[4] Malignant transformation is seen in approximately 2% of all cases of MCT.[5] Here, we report a rare case of MCTs (dermoid cyst) in a postmenopausal multiparous woman masquerading as lithopaedion clinicoradiologically.
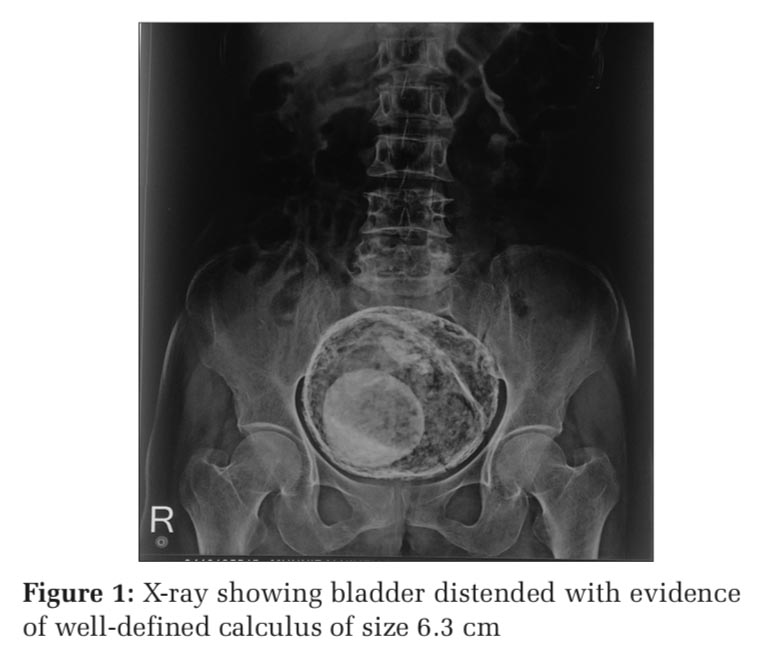
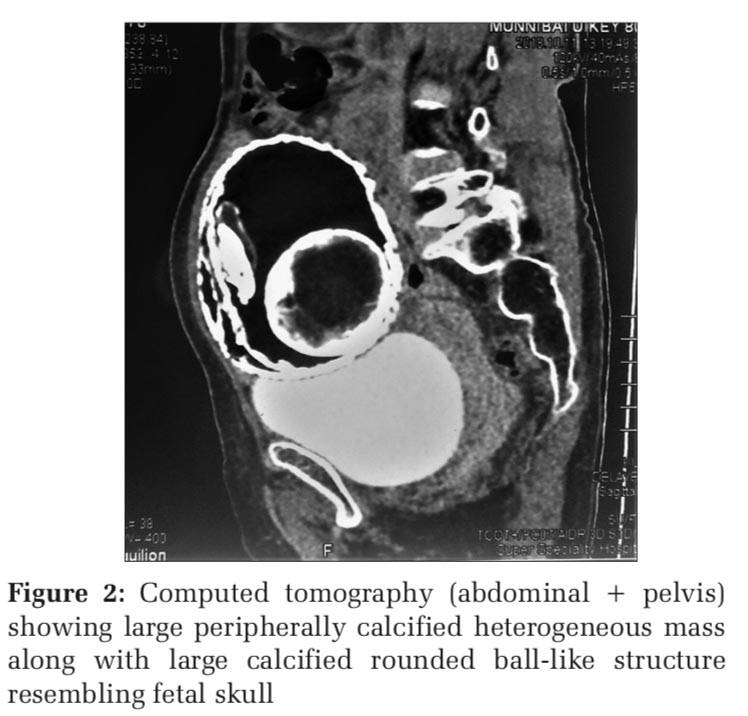
An 80-year-old multiparous female presented to the urology department with a history of pain in the lower abdomen in the past 1 month and burning in micturition in the past 1 week. X-ray abdomen-pelvic and an abdominopelvic ultrasonography revealed bladder which was well distended with irregular 11mm wall thickening with trabeculations and sacculations. There was evidence of well-defined calculus of size 6.3 cm showing movement with the gravity (Figure 1). Further, the patient was subjected for computed tomography (abdominal + pelvis) which showed large peripherally calcified heterogeneous pelvic abdominal mass measuring 11.8 cm × 9.9 cm × 9.7 cm with calcified septa in it. The lesion showed soft tissue density along with large calcified rounded ball like structure resembling fetal skull as a part of calcified density component. It also showed eccentrically placed soft tissue density structure with few varying shaped chunky calcified foci. The urinary bladder was normal and distended with no evidence of calculus within. The uterus and right adnexa were appearing normal. However, the left ovary was not visualized. With these imaging features, lithopedion versus MCT were the differential diagnosis offered clinically (Figure 2).
With these imaging findings, the patient was subjected to exploratory laparotomy. Large pedunculated cystic mass of size 12 cm × 10 cm × 8 cm was removed with ease. The uterus and right adnexa were found normal; however, the left ovary was not visualized by the surgeon.
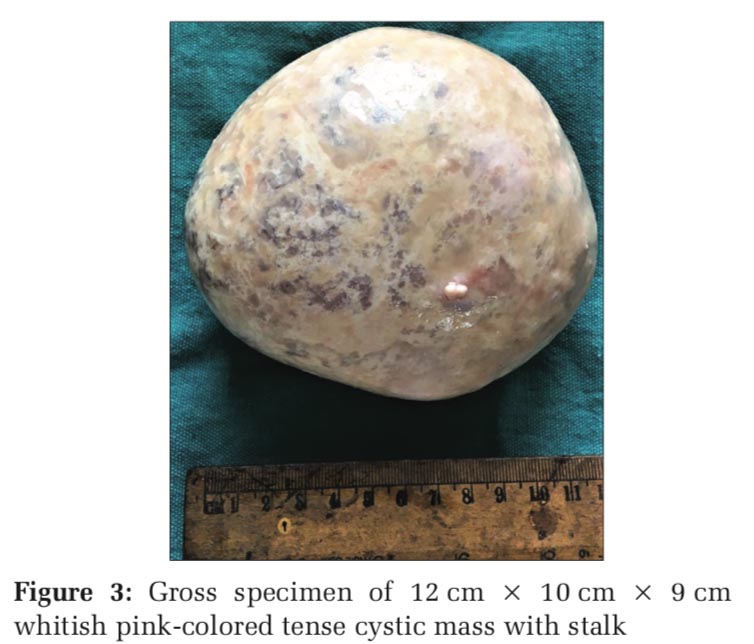
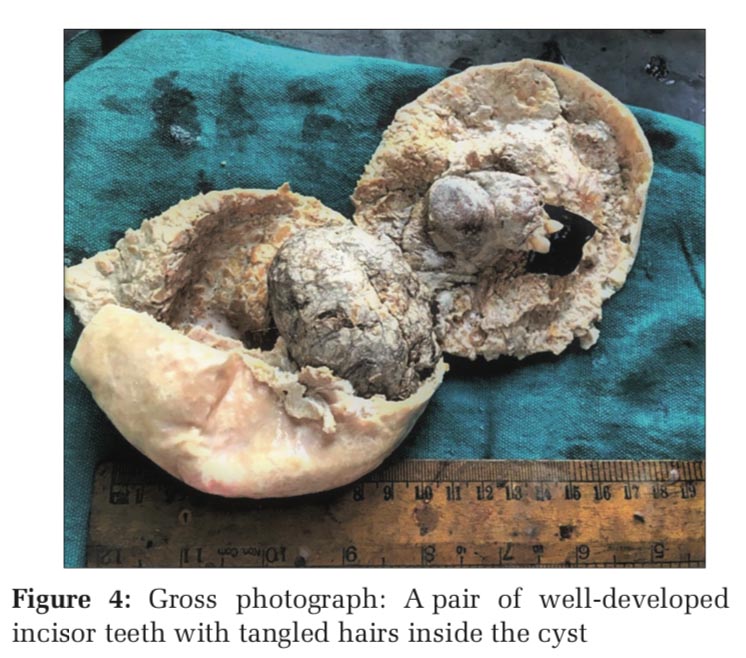
We received a gross specimen of 12 cm × 10 cm × 9 cm whitish pink-colored tense cystic mass with small stump attached to it (Figure 3). Cyst was gritty to cut and filled with yellowish thick viscous fluid. Cyst also contained a mass of tangled hair ball mixed with cheesy material. On removing hair ball and fluid, a solid protuberance of size 3 cm × 2 cm × 2 cm and a pair of well-developed incisor teeth also seen (Figure 4). Multiple sections from representative areas were taken/E-stained sections showed fibrocollagenous wall with deposition of plenty of amorphous calcification.
Sections from Rokitansky’s protuberance showed stratified squamous epithelium, sebaceous glands, hair follicles, and adipose tissue along with dense amorphous calcification. Diagnosis of MCTs was confirmed histomorphologically probably arising in the left ovary as it was not visualized intraoperatively.
The word teratoma is derived from the Greek word teratos which means “deformity”/“monster” and oma which means a tumor. Thus, the teratoma is a monster tumor. It was initially used by Virchow in 1863. The term “dermoid cyst” was coined by Leblanc in 1983.[6] MCTs (dermoid cyst) is the most common germ cell tumor of ovary accounting for about 20% of all ovarian neoplasm. It is the most common ovarian tumor of childhood as well.[2,3] However, occurring in a postmenopausal woman is a rare phenomenon.[4,7,8] They are unilateral in 88% of cases and provoke mostly symptoms relating to the mass. But sometimes presents as a surgical emergency with acute abdominal pain due to associated complications as torsion, hemorrhage or infectionn.[6] Our patient presented with unilateral mass and symptoms due to mass effect.
With imaging, unilocular lesion with fat and the nonfat components and calcification and/or ossification are diagnostic of dermoid cyst.[6,7] However, with large well-defined peripherally calcified pelvic-abdominal mass with calcified septae and having all three components (fat/soft tissue/internal chunky calcification), it can mimic lithopaedion (stone baby) in a postmenopausal woman,[9] a close differential of MCT on imaging. In our case, the first diagnosis was lithopaedion with the differential of mature teratoma on imaging.
Most of the MCT presents as 5–10 cm in diameter cyst on gross, and on sectioning, they usually contain thick sebaceous material, tangled hairs, and various dermal structures. In our case, gross and microscopic appearance was of classical MCTs confirming the diagnosis. Malignant transformation in the form of a neoplasm with somatic-type features is an uncommon event in MCT, probably in approximately 2% of all cases.[5] Mrkasian et al. reported that, in a 612-case series, malignancy risk was doubled over 50 years of age.[10] Park et al.[11] indicated that 45 years of age as the patient age and 99 mm as the tumor size were the optimal cutoffs for malignant transformation in MCT. It should be noted that in our postmenopausal multiparous patient (80 years) MCT, a benign tumor occurred despite of its largest diameter 12 cm.
To conclude, MCTs (dermoid cyst) occurring in postmenopausal multiparous woman masquerading as lithopaedion on imaging is a rare phenomenon. Thus, the mystery behind Monsters egg is resolved finally by morphology.
Subscribe now for latest articles and news.