Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.2021.v07i03.006
Year: 2021, Volume: 7, Issue: 3, Pages: 19-25
Original Article
Anupama P Gupta1 , Dharitri M Bhat1 , Suprita P Nayak2 , Aanchal Lohiya3 , Vrushali Mahajan2 , D T Kumbhalkar4
1Associate Professor, Department of Pathology, Government Medical College, Nagpur, India,
2Assistant Professor, Department of Pathology, Government Medical College, Nagpur, India,
3Resident, Department of Pathology, Government Medical College, Nagpur, India,
4Professor, Department of Pathology, Government Medical College, Nagpur, India
Address for correspondence:
Anupama P Gupta, Associate Professor, Department of Pathology, Government Medical College, Nagpur, India. E-mail: [email protected]
Introduction : Ophthalmic pathology including orbital, intraocular, and periorbital is unique. Wide spectrum of infections and neoplasia; benign as well as malignant are seen in this area. Many neoplastic conditions mimic non-neoplastic inflammatory conditions and needs differentiation before definitive therapy. Cytology is a simple, safe and fairly accurate technique for differentiating inflammatory from neoplastic and benign from malignant conditions thus avoiding more invasive surgical biopsies in these delicate areas. Present study was aimed to evaluate the role of fine needle aspiration as a tool in diagnosis of intra orbital and peri ocular adnexal lesions. Material and Method : FNAC was performed in a series of 20 patients presenting with intra orbital and peri ocular adnexal masses after clinical and radiological evaluation. Smears were analysed by a cytologist and histopathological confirmation was done as indicated. Results : The age ranged from 19 to 70 years. Male: Female ratio was 11:9. Of 20 cases, 03; 04; 03; 10 were infective, benign cystic lesions, benign neoplastic and malignant respectively. Of malignancies 02; 03; 02; 01; 01; 01 were of basal cell carcinoma, sebaceous carcinoma, squamous cell carcinoma, adenoid cystic carcinoma, micro cystic adnexal carcinoma and diffuse large B cell lymphoma respectively. Confirmation was done in 16 /20 cases. Concordance rate of FNAC with histologic diagnosis was 100% in broadly classifying them into infective, benign cystic, benign neoplastic and malignant neoplastic pathology. However, histopathology and Flow cytometry was helpful in subclassifying them in select cases.
Keywords: Fine Needle Aspiration Cytology, Orbital Lesions, Ocular Adnexal Lesions, lid
The orbit and lid are a location for mass lesions such as inflammatory and infectious diseases, cysts, various primary and secondary neoplasms.[1] Fine needle aspiration cytology (FNAC) being simple and minimally invasive, plays important role in diagnosis of lesions of delicate areas of orbit and lid especially in categorizing them into neoplastic and non-neoplastic, benign and malignant. It can be used for eyelid and palpable orbital, intra ocular lesions thus avoiding more invasive surgical biopsy. Even deep-seated ocular lesions/ tumours can be aspirated with the aid of ultra-sound and computed tomography (CT) guidance; thus, management becomes easier. Ultrasound-guided FNAC had also made the technique safer especially in cases where mass is posterior to the equator and in close relation to vital structures such as optic nerve and central retinal artery.[2] We present here a series of interesting cases diagnosed on FNAC ranging from benign to malignant with the aim to study the role of FNAC in eyelid, ocular and orbital lesions.
This is a descriptive study done over a period of one year from January 2018 to December 2018 at tertiary care hospital after taking ethical clearance and informed consent. It was aimed to highlight the role of cytology in orbital and ocular adnexal lesion and to study cytomorphological spectrum in these lesions. FNAC was performed using 24 gauze needles by non-aspiration as well as aspiration techniques in a series of total 20 patients of all age group presenting to cytology outpatient department with orbitaland ocular adnexal masses as a part of diagnostic procedure. Radiological guided FNAC was done as and when needed. Both wet fixed and dry smears were kept and stained with haematoxylin and eosin (H E), Papanicolaou (Pap) and May Grunwald Giemsa (MGG) stains. Special stains were done as and when indicated. Cytology diagnosis was confirmed by histopathology and ancillary tests like flow cytometry and immunohistochemistry as and when needed.
Of total 20 cases male: female was11: 9. Age ranged from 19- 70 years. Left: right eye; 12:8, eyelid: intra ocular; 12:8 was involved respectively. Lesions comprised of (n=03; 15%) infective (one each of Abscess, molluscum contagiosum and cryptococcosis); (n=04; 20 %) Benign cystic lesions (03 epidermal cyst, 01 conjunctival retention cyst); (n=03; 15 %) Benign Neoplasm (02 Pleomorphic Adenoma; 01 Schwannoma) and (n=10; 50 %) Malignant neoplasms (02 Basal Cell Carcinoma (BCC); 03 sebaceous carcinomas; 02 Squamous Cell Carcinoma (SCC);01 adenoid cystic carcinoma; 01 micro cystic adnexal carcinoma and 01 Diffuse large B cell Lymphoma (DLBCL)) respectively. (Table 1)
FNAC is a simple and valuable diagnostic procedure with high level of accuracy before surgery and also in deciding extent of surgery. It is also important in diagnosing recurrent lesions. FNAC of orbital tumours dates backs to 1975, as a rapid and minimally invasive diagnostic technique.[3] This area being delicate with wide range of possible lesions, their relative rarity and difficulties in direct surgical approach encourages the use of FNAC in the diagnosis of these lesions.[4] The limitations of the procedure include the varying sensitivity (50-98%) and the possible complications as haemorrhage, globe rupture, and ptosis.[5] The diagnostic accuracy of FNAC for orbital and adnexal lesions have been reported to be 47% to 100% in various studies and associated aid of ancillary tests increases its diagnostic value.[6–13]
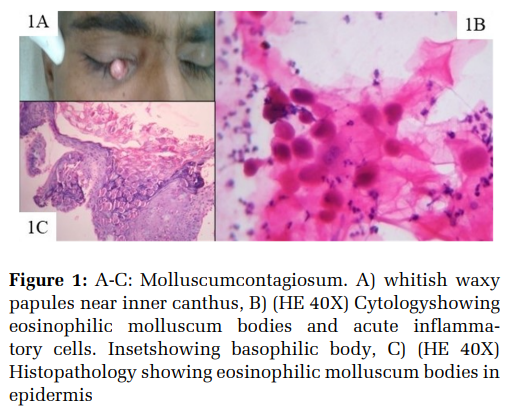
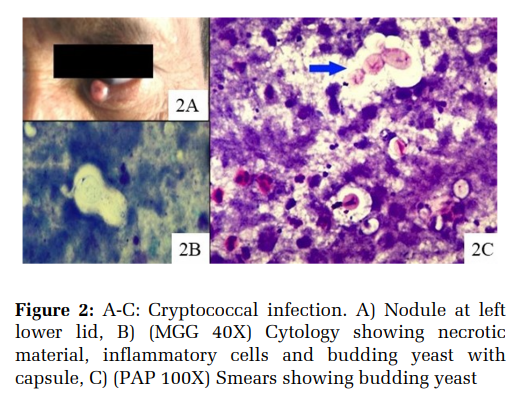
In a series by Nag et al the sensitivity and specificity of FNAC in the diagnosis of orbital lesions was 86.6% and 100%, respectively.[14] We had spectrum of interesting cases ranging from infective, benign and malignant. Location varied from lid, canthus of eye and intraocular. Clinically lesions ranged from nodular, cystic, ulcerated and fungating. Amongst infective lesions we had one acute inflammatory lesion of lower lid where staphylococci were detected and it resolved after antibiotics so no biopsy was done. One interesting case of molluscum contagiosum in Human immunodeficiency virus (HIV) positive patient showed eosinophilic molluscum bodies on cytology which was confirmed on histology. (Figure 1 A-C) A male patient on anti retro viral therapy for 3 years presented with lower lid swelling for 2 months. FNAC revealed budding yeast morphologically consistent with cryptococci which resolved after antifungal therapy. (Figure 2 A-C) Both the HIV positive patients had low CD 4 counts (50, 150 cells / cubic millimeter of blood respectively). Facial molluscum and fungal infections can be marker of severe immunosuppression in HIV patients and FNAC diagnosis can help in treatment planning.[15]
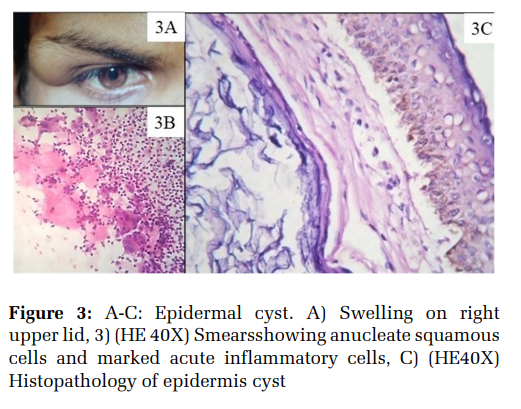
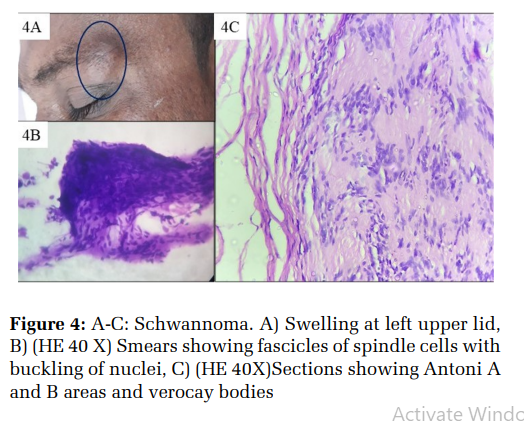
Benign cystic lesions included three epidermal cysts which showed anucleate squamous cells in keratinous background. One of which one was infected epidermal cyst at outer canthus of eye with giant cell reaction (Figure 3 A-C). One case of tiny nodule at bulbar conjunctiva revealed clear fluid on aspiration and diagnosed as conjunctival retention cyst. It resolved with therapeutic aspiration, topical steroids, and antibiotic drops. A right upper lid nodule which was painful while aspiration showed features of benign peripheral nerve sheet tumour of upper eyelid on cytology and was confirmed and subtyped as schwannoma on histopathology. (Figure 4 A-C) Of the two pleomorphic adenomas (PA) one was of right eye (upper lid outer canthus) with classical cytology and histomorphology. (Figure 5 A, A1) Other case was known case of PA of lacrimal gland operated one year back who presented with lobulated soft tissues lesion with solid cystic changes suggesting recurrence or malignancy. Cytology showed chondromyxoid stroma and epithelial and myoepithelial cells and some metaplastic and dysplastic squamous cells and was given as recurrent PA with dysplastic squamous cells. It was excised and confirmed as recurrent PA. As metaplastic and dysplastic squamous cells were seen on cytology, immunohistochemistry markers were also done to rule out any possibility of carcinoma ex Pleomorphic Adenoma. It showed positivity for CK 14, SMA, focal GFAP, Ki 67 index 5% thus ruling out possibility of malignancy. (Figure 5B-F) Lacrimal gland PA is known for recurrence and infiltrate adjacent structures extensively if not excised properly and are prone for even malignant transformation.[16]
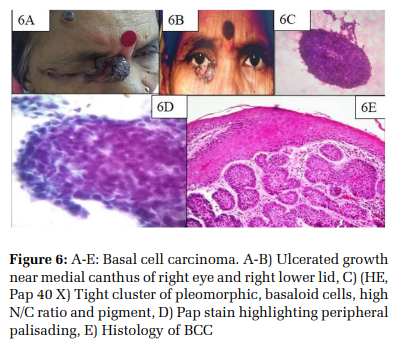
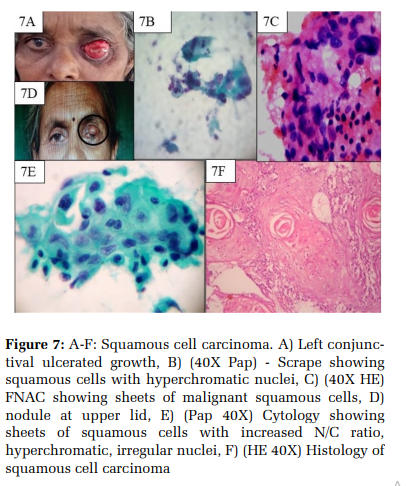
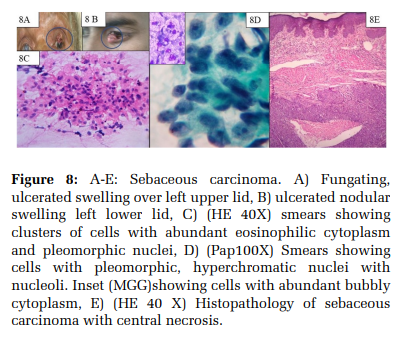
Of ten malignancies two were basal cell carcinoma (BCC), two squamous cell carcinoma, three sebaceous carcinomas, one adenoid cystic carcinoma, one micro cystic adnexal carcinoma of lacrimal gland and one diffuse large B cell lymphoma with deposits in lid Table 1 Cases of BCC showed basaloid cells with palisading on cytology, of which one showed prominent pigmentation which was later confirmed histologically as pigmented BCC. (Figure 6 A-E) Case of conjunctival ulcero-proliferative lesion was aspirated using non aspiration technique as well as scrape was taken and was diagnosed as squamous cell carcinoma. (Figure 7 A-C) This patient refused treatment and expired within few months. Other patient had 1x1 cm nodular swelling on left upper lid, slight ulceration was diagnosed on FNAC as SCC and confirmed on histopathology. (Figure 7DF) Of the three cases of sebaceous carcinoma one had ulcero-proliferative lesion in left upper lid and two cases had lower lid nodule and were clinically suspected as chalazion. All three showed features of malignancy with cytoplasmic vacuoles, mitosis and scattered foam cells which were diagnosed as sebaceous carcinoma and later confirmed on histopathology (Figure 8 A-E).
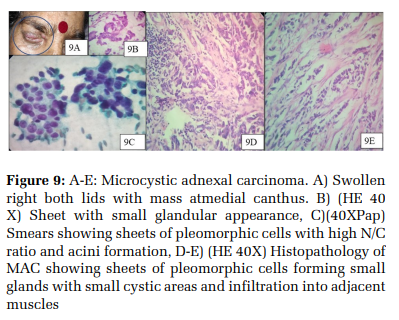
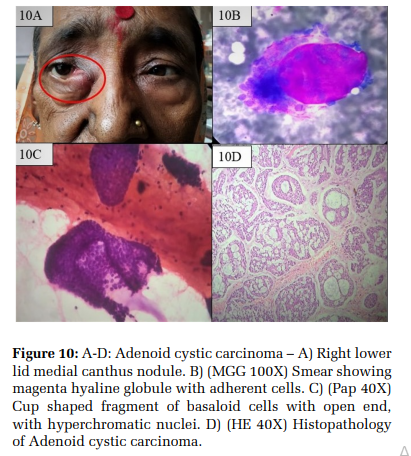
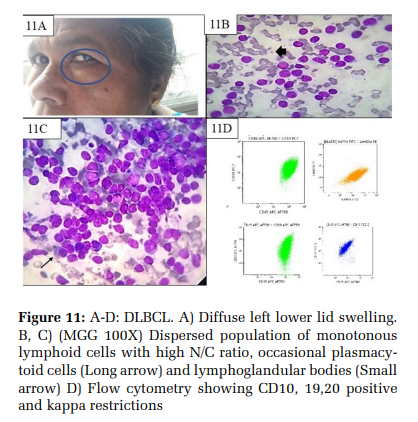
One interesting case of 69 years female who was referred as carcinoma in situ with inflammation on biopsy from other centre with no other details available. Patient presented with periorbital swelling and nodularity after 3 months. FNAC from nodule at medial canthus was done and given as adenocarcinoma. Later right eye ball with lids were removed showing grey white tumour of 2x2x2 cm shifting eyeball to opposite side. Histology revealed features of micro cystic adnexal carcinoma infiltrating into deeper tissues with peri neural invasion and no vascular invasion. Other structures from eye ball were free from tumour. (Figure 9 A-E) Microcystic adnexal carcinoma (MAC)is a rare, locally invasive malignancy occurring on face but can rarely invade orbit. Rare cases of primary orbital MAC have been also reported.[17] A case of adenoid cystic carcinoma had lower lid swelling and showed cup shaped fragments of tumour cells with nuclear enlargement and moulding, coarse chromatin, naked nuclei and hyaline globules with adherent tumour cells which was confirmed on histology to be adenoid cystic carcinoma. (Figure 10 A-D) A 61 years female presented with left sided periorbital swelling of size 3x1x1cm for 6-7 months. CT revealed well defined homogenous mass in left adnexa. Ultra-sonography showed well defined heterogenous lesion in inferiorlateral aspect left orbit suggestive of neoplastic (metastatic) aetiology. FNAC showed medium to large sized lymphoid cells with large nuclei, occasional nuclear clefts and scant cytoplasm. Cytological diagnosis was given as lymphoreticular malignancy favouring non-Hodgkin’s lymphoma. Re-aspiration and Flow cytometry revealed CD 3, 4,5, 7, 8 negative and CD 45, 10, 19,20 positive and kappa positive (Figure 11 A-D). Thus, confirming diagnosis as Diffuse large B cell lymphoma (DLBCL). Bone marrow also revealed atypical lymphoid cells and CT revealed intra-abdominal lymphadenopathy and mild splenomegaly. Primary orbital and periorbital DLBCL though uncommon, DLBCL is the second most common lymphoma after Mucosal Associated Lymphoid Tissue (MALT) lymphoma in orbit. Alkatan et al encountered only 5 cases in their institute over 25 years of ophthalmic practice. They concluded ophthalmologist to be aware in order to avoid delays in the proper diagnosis and treatment.[18]
We had 100% concordance between cytology diagnosis and final diagnosis by histopathology and flow cytometry in broadly classifying lesions into inflammatory, cystic, benign and malignant. However specific typing of benign peripheral nerve sheath tumour into schwannoma in one case, adenocarcinoma of lacrimal duct into microcystic variant of adenocarcinoma in one case and nonHodgkin’s lymphoma into DLBCL in one case was done on histopathology and flowcytometry. Roozitalab et al found the consistent definitive diagnosis and the accuracy of FNAC to differentiate benign from malignant lesions were 85% and 100% respectively.[19]
We did not encounter any complication in our study. However, some of the studies have reported serious complications, such as intraocular and orbital haemorrhages and damage to the optic nerve.[20] Whereas Roozitalab et al had no complication as they did direct aspiration on anterior palpable orbital and eyelid lesions, and emphasized that with due care these complications could be avoided.[19]Due to high accuracy of FNAC and the inherent risks associated with surgical biopsy in deep-seated orbital lesions, it is advisable to perform FNAC under CT-scan or sonography guidance.[21]
Many malignancies mimic benign or inflammatory or non-Neoplastic inflammatory conditions and needs differentiation before definitive therapy is planned. Thus, skillful and innovative sampling techniques like non aspiration, scrape or aspiration technique using precise imaging from sensitive ocular lesions rewards with adequate cytological material for accurate diagnosis and at times it can eliminate the need for further surgery.[13,22]
Limitation of study – Being an unusual location and delicate area of face number of samples are limited and comparison group is not available. More extensive sampling is needed.

FNAC of orbital and periorbital lesions when done with adequate safety precautions, clinicalradiological correlation and skill of cytologist prove to be safe, rapid and invaluable diagnostic technique in diagnosing various orbital lesions especially in early diagnosis of malignant lesions and deciding extent of surgery.
Subscribe now for latest articles and news.