Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.v10.i2.23.17
Year: 2024, Volume: 10, Issue: 2, Pages: 213-218
Case Series
Simran Ailani1 , Manju Raghava1 , Neha Sethi2 , Maneesh Vijaywargiya2
1Department of Pathology, Mahatma Gandhi Medical College and Hospital, MGUMST, Jaipur, India,
2Department of Oncopathology, Mahatma Gandhi Medical College, MGUMST and Hospital, Jaipur, India
Address for correspondence:
Simran Ailani, Department of Pathology, Mahatma Gandhi Medical College and Hospital, MGUMST, Jaipur, India.
E-mail: [email protected]
Received Date:21 December 2023, Accepted Date:08 March 2024, Published Date:30 July 2024
To evaluate the clinicopathological profiles of patients presenting with testicular lymphomas. In our study from February 2020 to August 2023, 6 rare cases of testicular non hodgkin’s lymphomas were diagnosed in a three and a half year period and were divided based on primary or secondary involvement. Immunohistochemistry (IHC) was performed on all cases and results were compared based on clinicopathological profile. The mean age was 57 years. Most common presenting complaint was unilateral or bilateral testicular swelling, associated with pain in some cases. B symptoms were present only in one case. Out of 6 cases, 3 showed primary involvement and 3 were secondarily involved. On applying IHC, 3 cases were diagnosed as Diffuse Large B-Cell Lymphoma (DLBCL), Non-Germinal Centre subtype and 3 as DLBCL, Germinal Centre subtype.Testicular lymphomas are rare highly malignant tumors and pose a strong diagnostic difficulty for both clinician and pathologist. Hence, clinical suspicion should always be maintained in cases of testicular swelling for proper workup of the patient.
Keywords: Testicular lymphoma, Diffuse large B-cell lymphoma, Testis, Extranodal
Testicular lymphoma is a rare extra nodal manifestation of Non - Hodgkin’s Lymphoma representing 1 to 2% cases. It accounts for 5% of all testicular tumors 1. These tumors predominantly present in elderly and represent as the most common testicular tumor after age of 60 years 2. Secondary involvement of testis is more common than primary testicular lymphoma 3. Most common clinical presentation is of unilateral, painless testicular swelling or mass2.
Among all lymphomas, Diffuse Large B-Cell Lymphoma (DLBCL) is the most common, amounting upto 80-90% cases 4, 5. DLBCL is further categorized into Germinal center B-cell (GCB) and non-germinal center B-cell (non-GCB) also known as activated B-cell (ABC) subtype based on Han’s algorithm 6. The algorithm takes into consideration three immunohistochemistry (IHC) markers, namely CD10, BCL6 and MUM1. Any DLBCL with CD10 positivity or with only BCL6 positivity (CD10 and MUM1negative) are considered to be GCB subtype. Rest all are considered as non-GCB. Despite having low incidence, DLBCL are highly aggressive tumors. Advanced cases can disseminate to other extra nodal sites, like central nervous system (CNS), contralateral testis, pleura and soft tissue 3, 4. In DLBCL, there have been recent advances in understanding effects of BCL-2, BCL-6 and CMYC alterations 7, 8.
Other lymphomas, although rarer, should also be evaluated as they are clinically significant, for example burkitt lymphoma or burkitt like lymphoma which is associated with HIV infection.
The standard treatment approach for testicular lymphoma involves orchidectomy, followed by chemotherapy regimens such as R-CHOP (rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone) or R-CHOP like regimens 9. In addition to this primary treatment, it is highly recommended to consider the addition of central nervous system (CNS) prophylaxis using CNS-penetrating chemotherapy or intrathecal chemotherapy. Furthermore, irradiation or surgical excision of the contralateral testis is also strongly advised 10. These combined approaches aim to achieve optimal disease control and reduce the risk of CNS involvement or disease recurrence.
The goal of this study was to evaluate the incidence, clinical and histological features of testicular lymphoma along with their immunophenotypic characteristics.
The clinical and histopathological data of all cases of testicular tumors submitted to the Department of surgical pathology from February 2020 to August 2023 was retrieved. Out of 81 specimens, only 6 cases were diagnosed with testicular lymphoma. An analysis of clinical and laboratory information was done on these cases. The clinical information included age, symptoms, medical and surgical history was recorded. Laboratory investigations included hematological workup like complete blood count, serum LDH, bone marrow aspiration, bone marrow biopsy and radiologic workup including ultrasonography, CECT and MRI scans. These cases were categorized into primary and secondary as per their involvement. The staging for testicular lymphoma was done using Cotswold- Modified Ann Arbor criteria 11. Detailed histopathological and immunohistochemical study was done for evaluation and further categorization of these tumors.
The research has received no external funding. No conflicts of interest have been declared. There were no ethical issues.
The orchidectomy specimens of 6 cases were processed, including fixation in 10% Neutral Buffered Formalin (NBF). Grossing of the resected specimens was done as per oncology gross protocol. A special mention of invasion of tumor to rete testis, epididymis, tunica, spermatic cord and scrotum was noted. Formalin fixed sections were cut having thickness of 5 microns, these sections were dehydrated in graded ethanol, cleared with xylene and then embedded in paraffin wax. Thin sections were cut using rotary microtome and classic histological slides were prepared by staining with hematoxylin and eosin, dehydrated, air dried and mounted. Immunohistochemistry was performed by using HRP Polymerase system. A known positive internal or external control for antibodies was used. A combination of IHC markers were then used for confirmation of histology and further categorization done according to Han’s algorithm 5.
In each case lymphoma panel was tested in a stepwise manner. These lymphoma markers included B-cell markers like CD19, CD20, PAX5, BCL2, BCL6, CD10, MUM1, CD15, CD30, T/NK cell markers like CD3, CD5, CD56. Other markers used included c-MYC, Ki67, CK, vimentin, PLAP, SALL-4. The results were evaluated by experienced pathologists. MUM1, C-MYC, BCL-6, KI-67 mainly expressed in nucleus. CD10, CD20 expressed in cytoplasmic membrane. BCL-2 expressed in both cytoplasm and cell membrane. Hans algorithm was applied to classify DLBCL into GCB and non-GCB type. CD10, BCL-6 and MUM-1 were considered positive at a cutoff of 30% positive tumor cells. For MYC cutoff was 40% and for BCL-2 50% was considered.
Between February 2020 and June 2023, out of 81 cases of testicular tumors, six cases (7.4%) were diagnosed as testicular lymphoma. The age ranged from 39-70 years, mean age being 57 years. The median age was 58 years.
The most common presenting symptom was unilateral scrotal/testicular swelling, associated with pain in 1 case. Out of 6, 3 cases were of primary testicular lymphoma and 3 had secondary involvement of testis. According to Cotswold Modified Ann-Arbor criteria, one patient had advanced stage tumor. B symptom (fever and weight loss) was present in one case Table 1.
|
Case No. |
Age (years) |
Laterality |
Presenting Symptom |
Origin |
Stage |
|---|---|---|---|---|---|
|
1 |
55 |
Right |
Testicular swelling with pain |
Primary |
I-EA |
|
2 |
52 |
Right |
Testicular swelling, lymphadenopathy (inguinal and retroperitoneal) |
Secondary |
II-EA |
|
3 |
70 |
Bilateral |
Testicular swelling |
Primary |
I-EA |
|
4 |
66 |
Right |
Testicular swelling, lymphadenopathy (mediastinal) |
Secondary |
III-EB |
|
5 |
61 |
Right |
Testicular swelling |
Primary |
I-EA |
|
6 |
39 |
Right |
Testicular swelling, lymphadenopathy (mediastinal) |
Secondary |
IV-EA |
Preoperative ultrasonography in four cases showed testicular enlargement on right side with diffuse or nodular distribution. One case had left testicular mass with right epididymal and paratesticular hypo-echoic nodules.
CECT chest in one case showed mediastinal mass with multiple abdominal lymphadenopathies. CECT abdomen in other case showed bilateral inguinal lymphadenopathy, multiple enlarged retroperitoneal lymphadenopathies.
MRI inguinal and scrotal region in one case showed nodular lesions along superior pole of right testis extending up-to right spermatic cord and superficial inguinal ring.
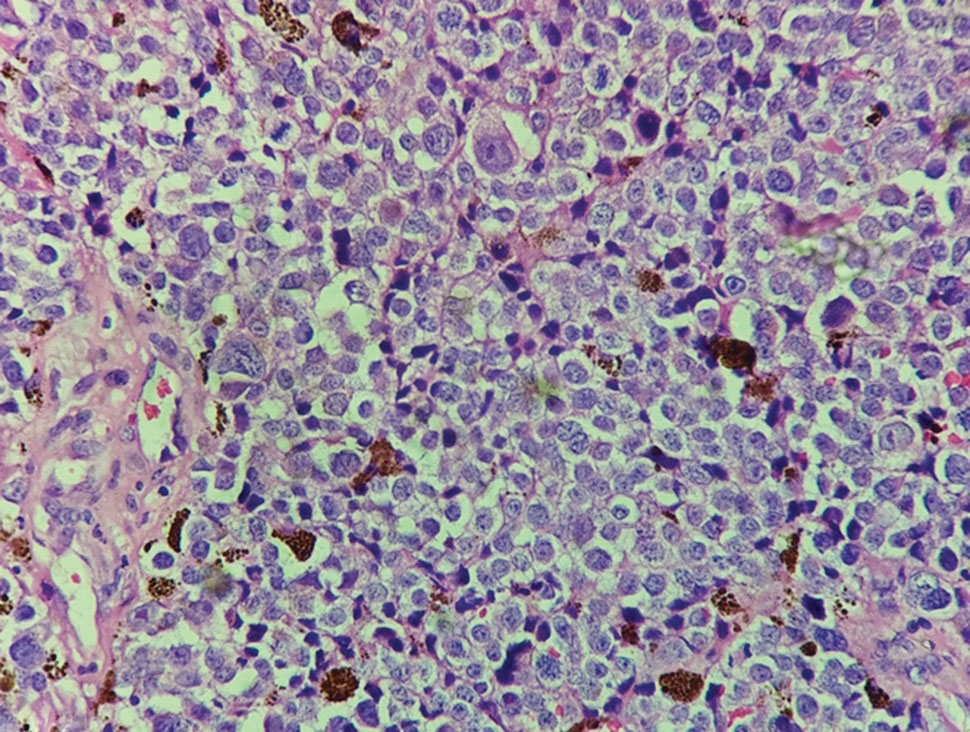
All patients underwent high inguinal orchidectomy of tumor side. Postoperative pathological grossing showed enlarged testis. On cutting a diffuse, solid grey white testicular mass was noted having clear boundaries with median diameter of 6.0 cm (Range 4.5 to 8.0 cm). Figure 1 On microscopy, all 6 cases showed malignant round tumor cells arranged in sheets having scant cytoplasm, irregular nuclear membrane, coarsely clumped chromatin and inconspicuous nucleoli. 3 cases had epididymis invasion, and 2 had spermatic cord involvement. Overlying tunica was involved in 3 cases.

On IHC cells were immunopositive for CD20 in all cases. 3 cases were characteristically CD10 positive. 2 were Bcl-6 negative and MUM-1 positive, one showed Bcl-6 and MUM-1 positivity. C-MYC showed positivity in 1 case and Bcl-2 was positive in 4 cases. All cases were negative for CD3, CD30, PLAP, SALL4. On the basis of Han’s algorithm, 3 cases were diagnosed as DLBCL-GC subtype and 3 were diagnosed as DLBCL-non GC subtype Figure 2, Table 2.
3 patients underwent bone marrow aspiration and biopsy which showed normocellular marrow having no lymphoma cell infiltration.

|
Cases |
CD-20 |
CD-10 |
MUM-1 |
BCL-2 |
BCL-6 |
Ki-67 |
Diagnosis |
Hans class |
|---|---|---|---|---|---|---|---|---|
|
1 |
+ |
- |
+ |
+ |
+ |
80% |
DLBCL |
Non-GC |
|
2 |
+ |
+ |
- |
- |
- |
80% |
DLBCL |
GC |
|
3 |
+ |
- |
- |
+ |
- |
50-60% |
DLBCL |
Non-GC |
|
4 |
+ |
- |
+ |
+ |
- |
80% |
DLBCL |
Non-GC |
|
5 |
+ |
+ |
- |
- |
+ |
60% |
DLBCL |
GC |
|
6 |
+ |
+ |
+ |
+ |
- |
50-60% |
DLBCL |
GC |
Testicular lymphomas are rare neoplasms accounting for 1-2% of non-Hodgkin’s lymphomas and 5% of testicular tumors 1. The median age of presentation is 58 years which is comparable to past study done by Shahab N et al 2 on Indian population but younger when compared to other international studies 12. During primary examination, the most common presentation was of painless unilateral scrotal swelling which has been found in past studies 13. Bilateral testicular involvement has been noticed previously in 35% of cases which often involve CNS 12. In our study 1 case (20%) had bilateral testicular involvement. Systemic B symptoms observed in 25-41% of advanced cases 14, were noticed in one patient.
In previous studies, a higher incidence of tumor spread to the epididymis and spermatic cord has been suggested. In our study, three out of five cases exhibited epididymal involvement, while two cases showed involvement of the spermatic cord.
These tumors exhibit characteristics associated with the deregulation of intercellular immune signaling mechanisms. This includes the activation of the NFkB pathway, oncogenic toll-like receptor (TLR) signaling (via MYD88 activating mutations), and B cell receptor (BCR) signaling (via CD79b mutation). They all contribute to NFkB pathway activation 15. Dysregulation in NFkB signaling is further compounded by pro-survival signals resulting from mutations in PIM1/2, CARD11, and TNFAIP3 16. DLBCL show mutations within genes responsible for immune surveillance, with losses in the HLA class I and II loci associated with reduced expression of major histocompatibility complexes (MHC).
Furthermore, gains and amplifications in the loci of programmed death ligand (PDL) 1 (CD274) and 2 (CD273) enhance protein expression, contributing to the suppression of an anti-tumor immune response 15. Increased serum lactate dehydrogenase (LDH) 17, increased serum B2 microglobulin, and hypoalbuminemia have been associated with an adverse prognosis in testicular
lymphoma. Adverse prognostic factors include age over 70 years, advanced stage of the disease, presence of B symptoms, involvement of extranodal sites other than the testis, and tumor diameter larger than 10 cm 12.
Grossly lymphomas present as enlarged testis with fleshy, lobulated and diffuse grey white firm mass with a homogenous cut surface and well demarcated borders.
The microscopic examination by routine hematoxylin and eosin staining shows diffuse sheets of large lymphoma cells infiltrating between seminiferous tubules. Eventually they replace the entire parenchyma 18. These lymphoma cells often invade and fill the seminiferous tubules. The presence of frequent mitotic figures can be observed 19, and necrosis is commonly seen. Most cases of testicular lymphoma exhibit a centroblastic morphology (90%), followed by immunoblastic morphology (10%).
Immunohistochemistry (IHC) findings in testicular lymphoma commonly reveal the expression of pan B cell antigens, including CD19, CD20, CD79a, and PAX5 20, 21. Additionally, BCL6 is expressed in 75-90% of cases, MUM1 in 40-70% of cases, and CD10 in 20-40% of cases. The proliferative index, as indicated by Ki67 staining, ranges from 40-90% with a mean of 70%.
Virtually all cases of testicular lymphoma show IGH rearrangements. Furthermore, rearrangements involving BCL6 (40%) followed by BCL2 and MYC occuring in 10% and 15% of cases, respectively.
Germinal center B-cell-like diffuse large B-cell lymphomas (GCB-DLBCLs) are characterized by the expression of CD10 and/or BCL6 but negativity for MUM1. On the other hand, non-GCB-DLBCLs are assigned to those that are negative for CD10 and positive for MUM1. GCB subtypes exhibit distinct clinical behaviors, with presence of improved clinical outcomes compared to non-GCB types along with higher survival rates.
Several studies have highlighted the predominance of non-GCB gene expression in primary testicular DLBCL as reported by Al-Abbadi et al 22.
Testicular lymphoma should be differentiated from Seminoma which are characterized by nests, cords, or sheets of tumor cells within thin, fibrous septa, and from Embryonal carcinoma, which presents with various histological patterns such as solid, papillary, or tubular growth patterns. Immunohistochemistry (IHC) findings can aid in distinguishing between these entities. Seminoma typically shows positive staining for SALL4, OCT3/4, CD117, and PLAP, while being negative for CD45, CD3, CD20, and CD30. In contrast, embryonal carcinoma is often positive for SALL4, OCT3/4, SOX2, and CD30, but negative for CD117, CD45, CD3, and CD20. Myeloid sarcoma is another differential diagnosis which exhibits diffuse replacement by blasts with thin nuclear membranes, fine chromatin, and variable prominent nucleoli. On IHC, they are positive for MPO.
Our retrospective study had major limitations. Firstly, because of low sample size sufficient statistical efficacy could not be made. Secondarily, due to insufficient data, certain prognostic scores could not be evaluated.
Our study showed lower age of incidence of testicular lymphomas (median age 58 years) as compared to other published studies (median age 68 years in R Fonseca et al 3 and Gundrum JD et al 12).
Subscribe now for latest articles and news.