Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.v9i3.23.151
Year: 2023, Volume: 9, Issue: 3, Pages: 288-295
Original Article
Sonal Bhati1 , Gunjan Bhatia2 , Shrey3 , Namita Goyal4
1Associate Professor, Pathology Department, RNT (Ravindranath Tagore) Medical College (Rajasthan University of Health Sciences), Udaipur, 313001, Rajasthan, India,
2Assistant Professor, Pathology Department, RNT (Ravindranath Tagore) Medical College (Rajasthan University of Health Sciences), Udaipur, 313001, Rajasthan, India,
3Resident, Pathology Department, RNT (Ravindranath Tagore) Medical College (Rajasthan University of Health Sciences), Udaipur, 313001, Rajasthan, India,
4Professor, Pathology Department, RNT (Ravindranath Tagore) Medical College (Rajasthan University of Health Sciences), Udaipur, 313001, Rajasthan, India
Address for correspondence:
Shrey, Resident, Pathology Department, RNT (Ravindranath Tagore) Medical College (Rajasthan University of Health Sciences), Udaipur, 313001, Rajasthan, India.
E-mail: [email protected]
Received Date:29 April 2023, Accepted Date:30 November 2023, Published Date:15 December 2023
Background: Globally, Breast cancer is the commonest malignancy among women. Neoadjuvant chemotherapy (NACT) is the treatment of choice for patients with locally advanced breast cancer. Pathological evaluation of tumor size remains the gold standard for evaluation of residual tumor after chemotherapy.1, 2 The aim of study was to evaluate histomorphological changes in the post-NACT MRM biopsies and to assess the response to chemotherapy. Method: The study was carried out over a period of one year in 30 patients of breast cancer who received neoadjuvant chemotherapy and underwent MRM. The pathological tumor response was evaluated. Observations: Mean age of presentation was 50.13 years and mean clinical size was 3.86 cm. Post MRM, residual tumor was found in 22 cases. The mean residual tumor size was 2.53 cm. Complete Pathological Response (pCR) was observed in 8 patients, partial response (pPR) developed in 19 patients and 3 patients elicited no response (pNR). The major observation was overall decrease in cellularity along with significant nuclear and stromal alterations. The common stromal changes observed was necrosis (n=24), fibrosis (n=22), desmoplasia (n=20), hyalinization of vessels (n=18) and chronic inflammatory infiltrates. Nuclear changes (n=14) and cytoplasmic vacuolations (n=11) were also observed. Presence of older age group, larger tumor size, DCIS, LVI and necrosis prior to chemotherapy indicated a poor response to treatment. Conclusion: Each patient responds differently to the NACT based on numerous factors like age, tumor size and tumor morphology. Hence, the pathologists must be aware of the vast array of histomorphological changes seen in breast post-NACT.
Keywords: Breast cancer, NeoAdjuvant Chemotherapy (NACT), Pathological response, Histomorphology, Modified radical mastectomy (MRM)
Globally, breast cancer is the commonest malignancy among women. From being fourth in the list of most common cancers in India during the 1990s, breast cancer has now become the first.1 Neoadjuvant chemotherapy (NACT-also known as preoperative or primary chemotherapy) is the treatment of choice for patients with locally advanced breast cancer. The standard NACT regime includes 4 cycles of AC (doxorubicin, cyclophosphamide) followed by 4 cycles of paclitaxel at interval of 3 weeks. NACT reduces the tumour size rendering an otherwise inoperable tumour operable and allows a more conservative surgery.2 The aim of NACT is to improve the outcome of surgery, downstage the disease by obtaining tumor shrinkage and henceforth evaluate the effectiveness of systemic therapy and prolong overall disease-free survival. Breast cancer incidence rates have risen in most of the past four decades; during the most recent data years (2010-2019), the rate increased by 0.5% annually, in contrast, breast cancer mortality rates have declined steadily in recent years (1.3% annually from 2011 to 2020).3 This can be attributed to early detection and timely treatment with NACT and surgical resection.
Clinical and radiologic evaluations of response to neoadjuvant chemotherapy are based on change in tumor size which is often inaccurate when compared with the tumor morphology pathologically. Pathological evaluation of tumor size remains the gold standard for evaluation of residual tumor after chemotherapy. Studies have shown that the patients who do not have any evidence of residual tumour post NACT, correspond with longer disease free and overall survival.4 In principle, the method to evaluate histologic subtype and tumor grade in breast cancer patients who received NACT is the same as that used for patients with non-neoadjuvant cancer. However, it is necessary to consider that chemotherapy can alter the histological architecture, nuclear features, and tumor mitosis.5 The present study involves pathological assessment of response to neoadjuvant chemotherapy and describes the various histopathological changes. These changes could predict the prognosis and also help in tailoring the treatment regimen to be used after surgery.
The present study was carried out in 30 patients of breast cancer who received 6 to 8 cycles of neoadjuvant chemotherapy and underwent Modified radical mastectomy (MRM), over a period of one year (January to December 2022), specimens of which were sent to the Histopathology lab, Pathology department of RNT Medical College, Udaipur, Rajasthan.
Aim of the study: To evaluate histomorphological changes in the post-NACT MRM biopsies and to assess the response to chemotherapy.
Inclusion criteria
Modified Radical Mastectomy (MRM) resection specimens of patients with breast carcinomas who had received NACT prior to surgery were included in the present study.
Only patients where pre-NACT biopsy was also done were included in the present study.
Exclusion criteria
The patients who did not receive NACT, or the treatment defaulters were excluded from the study.
The cases where a biopsy prior to NACT administration was unavailable were excluded from the study.
In each case, a detailed history and clinical examination, radiological investigations, clinical stage prior to NACT, details of chemotherapy and previous biopsy details were collected from the medical records of the patients. The resected specimens obtained after MRM following NACT were studied as per standard protocol. The specimens were fixed in 10% formalin. Grossing and sectioning of the specimen was done as per standard guidelines. Sections were processed and then embedded in paraffin wax. Microtomy was done and thin sections were taken on an albumenised slides, stained by Haematoxylin and Eosin (H&E) stain and examined under the microscope. The histopathological specimens following chemotherapy were evaluated for histomorphological changes in detail. The presence or absence of tumor, Ductal carcinoma in-situ (DCIS) and changes in tumor morphology was noted. The stroma was examined for host response such as inflammatory reaction, lymphocytic response, giant cell reaction and hyalinization. The presence of calcifications, fibrosis, necrosis and hemosiderin laden macrophages was also noted. Nuclear features were assessed such as karyorrhexis, pyknosis and karyolysis.
The pathological response was evaluated as per the Chevallier grading system. 6 Pathological response grading was done as follows:
Pathological Complete Response (pCR)- No residual invasive carcinoma or Ductal carcinoma in-situ (DCIS) in breast or lymph nodes.
Pathological Partial Response (pPR)- Presence of residual invasive carcinoma exhibiting stromal alterations.
Pathological No Response (pNR)- Little change in appearance or original carcinoma.
Lymphocytic response was graded as: 7
Grade 1- scattered lymphocytes in between tumor cells;
Grade 2-formation of microaggregates of lymphocytes;
Grade 3-dense infiltration of lymphocytes destroying tumor cells or forming masses.
If residual tumor was found, the histological grading was also done by Bloom Richardson (RB) grading system as shown in Table 1. 8
|
|
Score 1 |
Score 2 |
Score 3 |
|
Tubule formation |
>75% |
10-75% |
<10% |
|
Nuclear pleomorphism |
Mild |
Moderate |
Severe |
|
Mitotic figures |
<7/10 HPF |
8-14 /10 HPF |
>15/10 HPF |
HPF – High power field; RB – Bloom Richardson score
Finally, the results obtained were tabulated and statistically analysed. All the collected data was entered in Microsoft Excel 2016 and analysed by SPSS 16 software. For qualitative data, rate, percentage was calculated. For quantitative data, mean SD was calculated and statistical T test was used. p value of <0.05 was considered as statistically significant.
A total of 30 cases of female breast carcinoma were evaluated in the present study with age group ranging from 29 to 71 years and mean age of presentation being 50.13 years. It was found that 23 cases were of the age group up to 59 years (76.6%) and 7 cases were 60 years of age and above (23.3%). The patients presented clinically with a palpable breast lump with majority of the cases (16 out of 30) having a clinical tumor size of 2 to 5 cm at the time of presentation, mean clinical size being 3.86 cm with a standard deviation (SD) of 1.60. In our study both right and left breast lumps were encountered in equal frequency. 7 out of 30 cases (23.3%) gave a positive family history of breast carcinoma. These baseline sociographic demographic characteristics can be seen tabulated in Table 2. A biopsy report prior to MRM was available for all the cases, of which the most common presurgical diagnosis was invasive ductal carcinoma NOS.
|
Characteristics |
Number |
Percentage |
|
|
Age |
< 39 |
8 |
26.60% |
|
40- 59 |
15 |
50% |
|
|
>60 |
7 |
23.30% |
|
|
Sex |
Female |
30 |
100% |
|
Male |
0 |
0 |
|
|
Family history |
Yes |
7 |
23.30% |
|
No |
23 |
76.60% |
|
|
Clinical tumor size |
Up to 2 cm |
6 |
20% |
|
2-5cm |
16 |
53.30% |
|
|
>5 cm |
7 |
23.30% |
|
All cases in the present study received 6 to 8 cycles of NACT prior to surgery as per standard regime. On evaluation of post MRM resected tumor specimens, residual tumor was found in 22 cases. The mean residual tumor size was 2.53 cm (SD- 2.04). Lymphovascular invasion (LVI) was noted in 8 cases. On histologic examination, pathological complete response (pCR) with no evidence of viable tumor was observed in 8 patients. 5 cases were found to have DCIS. Pathological Partial response (pPR) developed in 19 patients and 3 patients elicited no response (pNR) to the therapy and showed similar findings as before NACT. Lymphocytic infiltrate was seen in total of 25 out of 27 cases that showed response to NACT, which accounts for 83.3% of the cases. The lymphocytic response was graded into three categories. Out of these, 12 cases (48%) had grade 1 response i.e., scattered lymphocytes in between tumor cells, 8 cases (32%) had grade 2 response i.e., formation of microaggregates of lymphocytes while in 5 cases (20%) grade 3 response was noted i.e., dense infiltration of lymphocytes destroying tumor cells or forming masses. Majority of the residual tumor specimens were ductal carcinomas(n=20), followed by lobular carcinoma (n=2) and remaining had complete response with no residual tumor pCR (n=8). It was observed that there was no change in histological type after administration of NACT. Of the cases studied, RB grade 1 was present in 13 cases, RB grade 2 was noted in 8 cases whereas RB grade 3 was noted in 1 case. The post chemotherapeutic histomorphological changes are shown in Table 3. The various patterns of arrangement of residual tumor were tubules, sheets, nests, cords and trabeculae.
|
Characteristics |
No. of cases |
Percentage |
|
Type of residual Carcinoma |
||
|
Invasive duct Ca NOS |
20 |
66.60% |
|
Lobular carcinoma |
2 |
6.60% |
|
Residual tumor size |
||
|
No tumor |
8 |
26.60% |
|
Up to 2 cm |
4 |
13.30% |
|
2cm to 5 cm |
13 |
43.30% |
|
More than 5 cm |
5 |
16.60% |
|
Post-op RB grade |
||
|
Grade 0 |
8 |
26.60% |
|
Grade 1 |
13 |
43.30% |
|
Grade 2 |
8 |
26.60% |
|
Grade 3 |
1 |
3.30% |
|
DCIS |
||
|
Yes |
5 |
16.60% |
|
No |
25 |
83.30% |
|
Lymphocytic response |
25/30 |
|
|
Grade 1 |
12/25 |
48% |
|
Grade 2 |
8/25 |
32% |
|
Grade 3 |
5/25 |
20% |
|
Tumor response grade |
||
|
pCR |
8 |
26.60% |
|
pPR |
19 |
63.30% |
|
no response |
3 |
10% |
Morphologically, post NACT necrosis of tumor was found in 24 cases. All of the cases showing pCR to NACT showed necrosis while 16 cases of pPR presented with necrosis. Among the nuclear alterations following NACT (pyknosis, karyorrhexis and karyolysis) was seen in 14 cases of which 4 cases had only focal nuclear alterations. Vacuolation was a commonly associated cytoplasmic alteration seen in 11 cases. The stromal alterations seen in majority of the cases were necrosis (n=24) followed by fibrosis (n=22), desmoplasia (n=20) and hyalinisation of blood vessels (n=18). Calcifications (n=5), Hemosiderin-laden macrophages (n=4) and giant cell formation (n=9) was also noted. Mucinous change was noted in 3 cases. These morphological changes have been tabulated in Table 4.
|
Morphological changes |
No. of Cases |
Percentage |
|
Lymphocytic infiltration |
25 |
83.3% |
|
Necrosis |
24 |
80.0% |
|
Fibrosis |
22 |
73.3% |
|
Desmoplasia |
20 |
66.6% |
|
Hyalinization |
18 |
54.0% |
|
Nuclear alterations |
14 |
46.6% |
|
Cytoplasmic vacuolation |
11 |
36.6% |
|
Giant cell formation |
9 |
30% |
|
Calcification |
5 |
16.6% |
|
Hemosiderin-laden macrophages |
4 |
13.3% |
|
Mucinous changes |
3 |
10% |
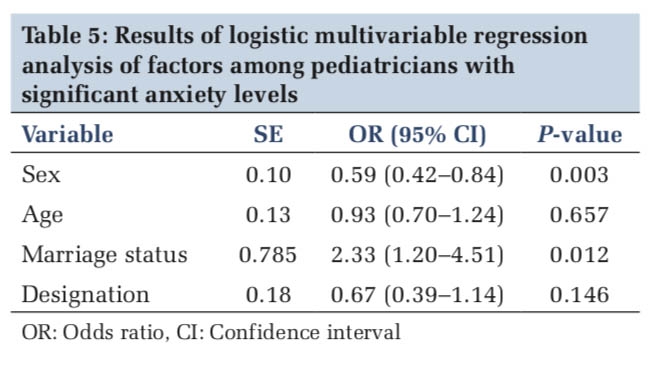
It was observed that majority of patients showing partial tumor response lie in the age group of 40-59 years (n=11). 7 out of 8 cases showing complete tumor response were below the age of 59 years while 2 out of 3 cases showing no tumor response were above 60 years of age. 5 cases that had a positive family history of breast cancer revealed partial tumor response and only 1 case had a complete response. On evaluation of the pre NACT clinical tumor size versus the post operative tumor size, it was seen that no tumor was found in all 8 cases that show pCR. Out of these 8 cases, 6 cases had a pre NACT size ranging from 2-5 cm and 2 with size less than 2 cm. In 2 cases of pPR, the size reduced from more than 5 cm to 2-5 cm’s. Majority of the cases with pPR had residual tumor size of 2-5 cm (n=12). 2 cases with no response had a tumor size of more than 5 cm same as the pre NACT clinical tumor size as shown in Table 5. The relation of tumor size with pathological response was found to be statistically significant. (p value- <0.001). DCIS component was seen in 5 cases diagnosed with pPR and was present in all 3 cases with no response. Tumor necrosis was found in biopsies of 4 cases that responded partially (pPR) and 2 cases with tumor necrosis developed no response.
|
Characteristics |
pPR (19 cases) Pathological partial response |
pCR (8 cases) Pathological complete response |
pNR (3 cases) No response |
P value |
||||
|
Age- |
< 39 |
4 |
50% |
4 |
50% |
0 |
0 |
0.186 |
|
|
40- 59 |
11 |
73.3% |
3 |
20% |
1 |
6.6% |
|
|
|
>60 |
4 |
57.1% |
1 |
14.2% |
2 |
28.5% |
|
|
Sex- |
Female |
19 |
63.3% |
8 |
26.6% |
3 |
10% |
--- |
|
|
Male |
0 |
0 |
0 |
0 |
0 |
0 |
|
|
Family history |
Yes |
5 |
71.4% |
1 |
14.2% |
1 |
14.2% |
0.730 |
|
|
No |
14 |
68.8% |
7 |
30.4% |
2 |
8.6% |
|
|
Residual Tumor size |
NO residual tumor |
0 |
0 |
8 |
100% |
0 |
0 |
<0.001 |
|
|
Up to 2 cm |
4 |
75% |
0 |
0 |
1 |
25% |
|
|
|
2cm to 5 cm |
12 |
100% |
0 |
0 |
0 |
0 |
|
|
|
More than 5 cm |
3 |
60% |
0 |
0 |
2 |
40% |
|
|
Type of cancer- |
pCR |
0 |
0% |
8 |
100% |
0 |
0 |
<0.001 |
|
|
Ductal carcinoma |
17 |
85% |
0 |
0 |
3 |
15% |
|
|
|
Lobular carcinoma |
2 |
100% |
0 |
0 |
0 |
0 |
|
Neoadjuvant chemotherapy (NACT) is a standard part of the multidisciplinary treatment of breast cancer. NACT has been shown to be equivalent to adjuvant chemotherapy in terms of disease free, distant disease-free, and overall survival in several clinical trials and enables more breast cancer patients to receive breast-conserving therapy.9 As NACT is being increasingly adapted for treatment of early-stage malignancies, pathologists need to be aware of these varied constellations of NACT induced changes. 4
To understand the numerous histopathological changes caused by NACT, we have included and analysed 30 cases of breast carcinoma in the present study who have received 6-8 cycles of NACT and have subsequently undergone MRM surgery in our institute. In our study the patients age group range from 29-71 years and the mean age is 50.73 years. The patients in younger age group responded more with a pCR than those with age >59 years as shown in Table 5. These results were similar to a study done by D. Vasudevan et al. (2015) that had a mean age of 50.58 and also revealed that the younger patients responded with a pCR. 8
Tumor type and tumor size- It was noted in our study that most commonly diagnosed carcinoma was invasive ductal carcinoma (66.6%) and only 2 cases of lobular carcinoma (6.6%) were diagnosed as shown in Table 3. According to Galal et al. (2007) invasive duct carcinoma NOS was found in 88% of their cases and invasive lobular carcinoma was about 12%. The mean clinical tumor size in our study at the time of diagnosis was 3.86 cm, with a standard deviation of 1.60.10 Post NACT the tumor size reduced to a mean of 2.53 cm’s with p value <0.001 which is statistically significant indicating a reduction in mean size of the tumor. It was observed that chemotherapy resulted in fibrosis and shrinkage of the tumor causing complete loss of growth in complete response and small scattered islands of tumor in partial response. The results were similar to a study conducted by S. Shareen et al. (2018) where the mean size of the tumor before induction of chemotherapy was found to be 3.75 cm whereas after chemotherapy it was 1.75 cm (p value <0.001). 11
Morphological changes- Chemotherapy induced morphologic changes were first described by Waller in 1960 when he described cytoplasmic swelling and vacuolation caused by administration of busulfan. Kennedy et al. in 1990 further described such changes in patients with breast carcinoma when combination of tamoxifen and cytotoxic drug therapy was used. 11
In the present study, a wide array of morphological changes due to chemotherapy were observed. The major observation was overall decrease in cellularity of the tumor along with significant nuclear and stromal alterations. There was increase in stromal oedema and distortion of glandular architecture post NACT. The most common stromal change observed post chemotherapy was necrosis (n=24), fibrosis (n=22), desmoplasia (n=20) and hyalinization of blood vessels (n=18). Other changes seen were calcifications, mucinous change, giant cells and hemosiderin laden- macrophages as shown in Table 4. Another important feature noted was presence of chronic inflammatory infiltrate mainly comprising lymphocytes, plasma cells and occasionally eosinophils. As shown in Table 3, this lymphocytic response noted in 25 cases, has been graded in our study where 48% cases have shown Grade 1 response, 32% have shown grade 2 response while remaining 20% have shown grade 3 response.
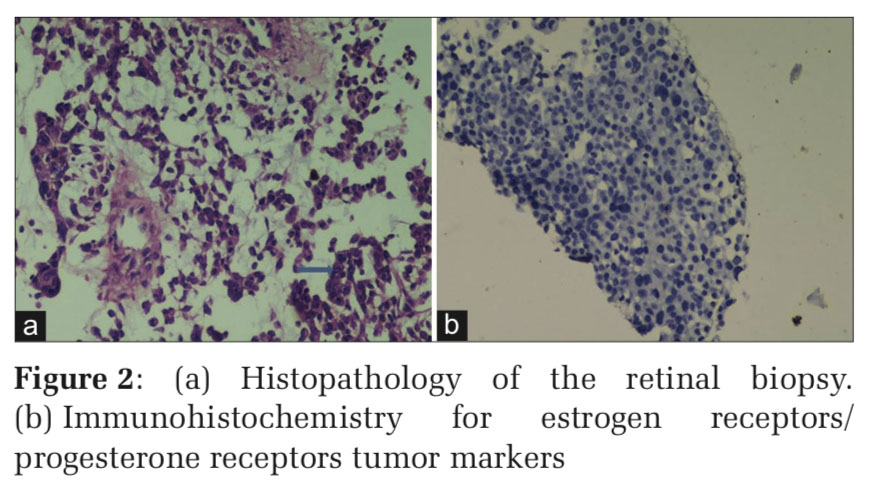
In our study, the residual tumor cells post chemotherapy were mostly scattered in the stroma individually showing discohesion. The nuclear changes (n=14) noted in were increased N:C ratio, bizarre nuclear morphology, multinucleation prominent nucleoli, karyorrhexis, karyolysis and pyknosis. Cytoplasmic vacuolations were also observed (n=11). Similar nuclear findings have also been described by the study of S. Sahoo et al. (2009). 12 Such cytologic changes are seen because of the cellular damage occurring secondary to neoadjuvant chemotherapy as has been hypothesized in other studies and are variable in different tumors after the therapy. Also, the actual change might further differ on the chemotherapy regimen used. The true biological significance of such changes in residual breast cancers, however, has received little attention and is poorly understood. Previously, many other studies have similarly described the morphological changes in the tumor cells and stroma in the patients with previous chemotherapy including fibrosis, collagenization, elastosis, hyalinization, microcalcification, neo-vascularization in the stroma, discohesion nuclear shrinkage, nuclear pyknosis, karyorrhexis, karyolysis, necrosis, cytoplasmic vacuolation and degenerative changes.11 The presence of bizarre cells and nuclear changes demonstrating partial tumor response to NACT in our study has been shown in Figure 1, while complete response with absence of tumor, lymphocytic infiltrate and fibrosis is shown in Figure 2.


Tumor response- Out of 30 cases in our study it was found that 8 cases showed complete response to treatment with no residual tumor (26.6 %) while 19 cases (63%) developed a partial response having stromal alterations and residual invasive carcinoma was seen and 3 cases (10%) had no response to the NACT (P value <0.001, statistically significant). Similar results were seen in a study conducted by Van der wall et al. (1996) where 21% cases had a pCR, 68% cases had a pPR while 11% cases had cNR.13 In another study conducted by Moon et al. (2005) 59% patients responded with pPR, 25% responded with cPR and 15 % cases had pNR. 14
It was also noted in the present study that those with a known family history of breast carcinoma had more percentage of incomplete response to the therapy. Patients that had presence of necrosis before administration of chemotherapy responded poorly to the treatment as none of them developed a complete response. 6 cases had a partial response (pPR) and 3 cases had no response (pNR). The presence of DCIS and Lymphovascular invasion prior to the treatment resulted in partial or no response to NACT. It was also noted that the patients with tumor size larger than 5 cm had a less response to NACT as compared to those with a smaller tumor size as illustrated in Figure 3.

Thus, in our study presence of older age group, larger tumor size, DCIS, LVI and necrosis prior to chemotherapy indicated a poor response to the treatment. The absence of these factors contributed to a better result and maximum patients had complete response. This goes along with the study conducted by Galal et al. (2007) which showed that initial tumor size < 5 cm, absence of ductal carcinoma in situ, and absence of vascular invasion were the best predictors of tumor response to chemotherapy. Their study stated that clinically small sized tumors responded better to chemotherapeutic regime. 10
Neoadjuvant chemotherapy has now become a standard protocol for treatment of nearly all patients with breast cancer as it has invariably benefited the patients long term survival. Histopathology is the gold standard for evaluating a tumor response in breast cancer post NACT. Each patient responds differently to the NACT and numerous factors like patients age, tumor size and tumor morphology that modify its ultimate effect on the patient. Currently, the post NACT MRM biopsies are evaluated by most pathologists similar to the routine non- NACT breast samples whereas studies clearly indicate numerous changes incurred on the tumor morphology due to chemotherapeutic effect. The role of pathologists is hence invaluable in assessing the tumor response to further indicate the treatment protocol thereby affecting overall prognosis of the patient. This will aid to the oncologists to plan further treatment and will ultimately benefit the patient. However, the significance of some of these morphological changes requires further studies on larger sample size.
Subscribe now for latest articles and news.