Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.v11.i2.24.98
Year: 2025, Volume: 11, Issue: 2, Pages: 121-128
Original Article
Mehak Sethi1 , Matuli Das2 , Saswati Sen3 , Manmath Kumar Das4 , Vanaja Iyer1
1Postgraduate, Department of Ophthalmology, Kalinga Institute of Medical Sciences, Bhubaneswar, Odisha, India,
2Professor, Department of Ophthalmology, Kalinga Institute of Medical Sciences, Bhubaneswar, Odisha, India,
3Associate Professor, Department of Ophthalmology, Kalinga Institute of Medical Sciences, Bhubaneswar, Odisha, India,
4Consultant, Department of Ophthalmology, Kalinga Institute of Medical Sciences, Bhubaneswar, Odisha, India
Address for correspondence:
Saswati Sen, Associate Professor, Department of Ophthalmology, Kalinga Institute of Medical Sciences, Bhubaneswar, Odisha, India.
E-mail: [email protected]
Received Date:25 March 2024, Accepted Date:14 February 2025, Published Date:12 May 2025
Objective: To compare refractive error and ocular biometry in children with spontaneously regressed ROP and those treated with laser or anti-VEGF. Methods: Purposive sampling was used. Three groups ROP regressed spontaneously (Group1), treated with laser (Group 2) and anti-VEGF injections (Group 3) were made. Axial length (AL), Keratometry (K1 and K2), Anterior chamber depth (ACD), Spherical equivalent (SE), Lens thickness (LT), Central Corneal Thickness (CCT), Posterior segment length (PSL) Anterior segment to posterior segment Ratio (ASL/PSL) and refractive error status were measured and compared. Results : 85 cases were included. Visual acuity (VA) was better in Group 3 (mean of 0.67 ± 0.38). Mean AL was less in Group 2 (20.60 ± 0.93 mm) compared to Group 1 (21.41 ± 1.38 mm) and 3 (21.76 ± 0.98 mm). Mean SE was greater in Group 2 ( -3.13 ± 1.63 D) as compared to Group 1 (-1.85 ± 2.05 D). Group 2 showed significantly thickened lens with a mean of 4.26 ± 0.37 mm. Mean ACD observed 3.00 ± 0.26mm which was comparatively deeper in the patients in the Group 3. Mean PSL of 13.48 ± 1.00 mm in Group 2 was shorter than other two groups. Number of high myopes was more in the Group 2. Conclusion : Spontaneously regressed ROP showed best results in terms of visual acuity and biometric parameters. Both anti-VEGF and laser are viable options for treatment of ROP. But anti-VEGF’s cause less treatment-related retinal damage and show quicker remission of active ROP and plus disease resulting in better visual outcomes.
Keywords: Retinopathy of prematurity, Anti-VEGF, Refractive error, Laser, Gestational age, Low birth weight
Retinopathy of prematurity (ROP) formerly called retrolental fibroplasia is a key factor contributing to avoidable blindness around the globe. It promotes vascularization of retina, the risk of which increases with reducing age of gestation (GA) thus making preterm low birth weight infants vulnerable.1 Vasoconstriction, via vasogenic factors like vascular endothelial growth factor (VEGF), and compensatory neovascularization are some of the potential mechanisms of injury that have been proposed. These processes can result in severe extraretinal fibrovascular proliferation and retinal detachment. With a frequency ranging from 35 to 60%, ROP is primarily restricted to preterm children with weight at birth (BW) below 1750 g or a GA of fewer than 34 weeks. 2
Laser is done in ROP as per guidelines recommended by ETROP (Early treatment retinopathy of prematurity) study, but now-a-days, intravitreal Anti-VEGF injections, particularly Bevacizumab (AVASTIN®) is being increasingly used in ROP, especially in APROP (aggressive posterior ROP) babies, and in those who are hemodynamically too sick to undergo laser ablation therapy.
Despite laser photocoagulation being the most effective treatment, there is a much higher risk of development of refractive errors, strabismus and amblyopia in these children.3, 4 It has been shown in studies that risk of development of refractive errors, high myopia is more in those babies treated with laser photocoagulation. 5 According to ETROP research, up to 29% of children treated for ROP go on to acquire significant visual impairment, and over 60% of those successfully treated for ROP have less-than-ideal vision. 6
The profile of ROP in such kids appears to be different from those in the West because the risk factors and availability of health facilities are different. Thus, it is important to study the ocular growth and biometric profile of children who develop ROP at birth to observe for the progression and development of refractive error in these children.
It is well known that newborns are normally slightly hyperopic. 7 This kind of hypermetropia is largely axial, with emmetropization gradually reducing the amount of hypermetropia over time.
Contrastingly, myopia is known to be linked to premature delivery despite shorter axial lengths. Prematurity affects vision during early childhood as well as in school going age group; the ametropic propensity lasts into adulthood. Myopia of preterm (MOP), a kind of myopia of infancy that is brought on by a halt in anterior segment development and is regardless of ROP status, can occur in premature newborns. Infants with mild ROP have refractive status that is comparable to preterm newborns without ROP but different from term infants. 8
The study was performed in the department of Ophthalmology of a tertiary care centre. All children were identified by reviewing past medical records of all patients admitted in NICU with history of ROP. Older children were recruited directly from the OPD. A total of 85 cases were included in the study using Purposive sampling. All children had been diagnosed and treated for ROP at least three years before the study commenced. Three groups were made as per the treatment administered. The first group was of patients where ROP regressed spontaneously, second was of those treated with laser and third was of those given anti-VEGF injections.
Informed consent was procured from the parents or natural guardians of all the children included in the study. A detailed ocular and medical history were taken. Visual acuity (VA) was recorded for both near and distance. Snellen’s visual acuity was converted to the logarithm scale of the minimum angle of resolution (logMAR). IOP was recorded by non-contact tonometer. A detailed biomicroscopic examination of the anterior segment was done. The biometric profile included: Axial length (AL), Keratometry (K1 and K2), Anterior chamber depth (ACD), Spherical equivalent (SE), Lens thickness (LT), Central Corneal Thickness (CCT), Posterior segment length (PSL) {PSL = Axial length – [Anterior Chamber Depth + Lens thickness]} Anterior segment to posterior segment Ratio (ASL/PSL) [ACD + LT / PSL]
All the above parameters were measured on the IOL master 700 (Carl Zeiss Meditech, Germany).
All children underwent cycloplegic refraction. It was done by instilling 0.5% cyclopentolate eye drops applied twice at 15 minutes interval followed by retinoscopy by a streak retinoscope. Those with refractive error were included after post cycloplegic acceptance. Status of binocular vision, presence of amblyopia and strabismus was evaluated. Detailed fundus examination was done.
Data was coded and recorded in the MS Excel spreadsheet program. SPSS v23 (IBM Corp.) was used for data analysis. For continuous variables, descriptive statistics was done like medians/IQRs and means/standard deviations. Right eye was considered for analysis. For Gaussian data distribution, for numerical variables analysis of variance (ANOVA) was used. For continuous data, Mann-Whitney U test was used for intergroup comparison. Chi-square test was used to assess associations between categorical variables among three groups made on the basis of treatment administered. P-value < 0.05 was considered statistically significant.
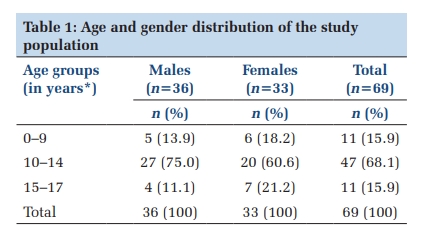
A total of 85 children were included in the study.30 out of them had spontaneously regressed ROP, 30 were treated with laser and 25 of them were treated with anti-VEGF injections. Baseline parameters of the study population was recorded (Table 1). The mean age at presentation was lower in patients treated with laser followed by those treated with anti-VEGF and the spontaneous regression group respectively. Gestational age and birth weight on the other hand was lower for anti-VEGF treated group followed by laser treated and spontaneous regression group respectively. Majority of patients in whom ROP regressed spontaneously had changes in ‘Zone 3 of retina and none had plus disease. In the laser treated group changes were present mostly in Zone 2 as against anti-VEGF treated group where maximum patients had changes in Zone 3 at the time of presentation. 17 patients in anti-VEGF treatment and 8 patients in laser treated group had plus disease. The details have been outlined in Table 2.
|
Parameters |
Spontaneously Regressed ROP |
Laser treated |
Anti-VEGF treated |
|
(n = 30) |
(n = 30) |
(n = 25) |
|
|
Mean ± SD |
Mean ± SD |
Mean ± SD |
|
|
AGE (in years) |
4.7 ± 1.20 |
4.33 ± 1.12 |
4.44 ± 1.08 |
|
Gestational age (in weeks) |
31.13 ± 2.62 |
30.43 ± 3.03 |
28.73 ± 2.48 |
|
Birth weight (in Kg) |
1.56 ± 0.48 |
1.53 ± 0.40 |
1.35 ± 0.35 |
|
Stages and zones |
Spontaneously Regressed ROP |
Laser treated |
Anti-VEGF treated |
|
(n = 30) |
(n = 30) |
(n = 25) |
|
|
Mean ± SD |
Mean ± SD |
Mean ± SD |
|
|
Zone 1 stage 2 |
- |
3 |
9 |
|
Zone 1 stage 3 |
- |
1 |
13 |
|
Zone 2 stage 2 |
1 |
7 |
- |
|
Zone 2 stage 3 |
- |
10 |
3 |
|
Zone 3 stage 2 |
18 |
2 |
- |
|
Zone 3 stage 3 |
11 |
7 |
- |
|
RIGHT EYE (OD) |
Spontaneously Regressed |
Laser treated |
Anti-VEGF treated |
p value |
|
ROP (n = 30) |
(n = 30) |
(n = 25) |
||
|
Mean ± SD |
Mean ± SD |
Mean ± SD |
||
|
VA (log MAR) |
0.74 ± 0.43 |
0.94 ± 0.36 |
0.67 ± 0.38 |
0.032 |
|
Axial length (AL) in mm |
21.41 ± 1.38 |
20.60 ± 0.93 |
21.76 ± 0.98 |
0.001 |
|
Spherical equivalent (SE) |
-1.85 ± 2.05 |
-3.13 ± 1.63 |
-2.08 ± 1.57 |
0.015 |
|
Anterior chamber depth (ACD) in mm |
3.23 ± 0.47 |
2.86 ± 0.27 |
3.00 ± 0.26 |
0.001 |
|
Lens thickness (LT) in mm |
3.62 ± 0.41 |
4.26 ± 0.37 |
3.67 ± 0.40 |
0.001 |
|
Keratometry (K1) in Dioptre |
43.21 ± 0.76 |
43.12 ± 1.13 |
43.25 ± 0.56 |
0.846 |
|
Keratometry (K2) in Dioptre |
44.99 ± 0.69 |
44.90 ± 1.21 |
45.08 ± 0.82 |
0.762 |
|
CCT (in µm) |
529.77 ± 35.35 |
519.98 ± 37.23 |
519.98 ± 33.36 |
0.48 |
The biometric profile of the patients was compared and is listed in Table 3. Uncorrected visual acuity was better in anti-VEGF treated group with a mean of 0.67 ± 0.38 than mean visual acuity of 0.74 ± 0.43 in spontaneously regressed ROP and 0.94 ± 0.36 in laser treated group. The results had a P value of 0.032 which was statistically significant. Axial length (AL) was observed to be very less in Laser treated ROP with a mean of 20.60 ± 0.93 mm compared to 21.41 ± 1.38 mm of mean in spontaneously regressed group and 21.76 ± 0.98 mm in anti-VEGF group (P <0.05). Spherical equivalent (SE) was much greater in laser treated group (mean of -3.13 ± 1.63 D) as compared to spontaneously regressed ROP with a mean of -1.85 ± 2.05 D and anti-VEGF treated ROP group with a mean of -2.08 ± 1.57D. A p-value of 0.015 which is statistically significant showed positive correlation. Shallower ACD was observed in laser treated group with a mean of 2.86 ± 0.27 mm (range 2.59 mm to 3.13mm) compared to that of anti-VEGF treated with mean of 3.00 ± 0.26 mm (range 2.74 mm to 3.26 mm) and regressed ROP with mean of 3.23 ± 0.47 mm. The parameter was statistically significant with p value 0.001. Laser treated group showed significantly thickened lens with a mean of 4.26 ± 0.37 mm (range 3.89 mm to 4.63 mm) whereas lens status in other 2 groups was similar with a mean of 3.62 ± 0.41 mm in regressed ROP and 3.67 ± 0.40 mm in anti-VEGF group (p value <0.05). Corneal curvature was comparatively steeper in anti-VEGF treated group i.e. K1 43.25 ± 0.56 D and K2 was 45.08 ± 0.82 D but the results were not statistically significant.
Central corneal thickness (CCT) in spontaneously regressed ROP with mean of 529.77 ± 35.35 µm, in laser treated mean CCT was 529.77 ± 35.35 µm and anti- VEGF treated showed mean of 519.98 ± 33.36 µm. The results were statistically insignificant.
We compared the posterior segment length with the anterior segment length to know the elongation and pathology possibly contributing to the refractive change. Mean PSL of 13.48 ± 1.00 mm in laser treated group was seen to be shorter than other 2 groups. In anti-VEGF treated mean PSL was 15.09 ± 1.14 mm and in spontaneously regressed ROP group mean PSL was 14.60 ± 1.52 mm (P value obtained was <0.05). Mean ASL/PSL ratio of 0.53 ± 0.07 in laser treated group was seen to be more than other 2 groups. In anti-VEGF treated mean ASL/ PSL ratio was 0.44 ± 0.05 and in spontaneously regressed ROP group ratio was 0.47 ± 0.08.
P value obtained was <0.05 which is statistically significant shows a correlation between treatment given and development of anterior and posterior segment (Table 4).
|
Parameter |
Spontaneously Regressed ROP |
Laser treated |
Anti-VEGF treated |
p value |
|
Posterior segment length (inmm) |
14.60 ± 1.52 |
13.48 ±1.00 |
15.09 ± 1.14 |
0.0001 |
|
ASL / PSL Ratio |
0.47 ± 0.08 |
0.53 ± 0.07 |
0.44 ± 0.05 |
0.0004 |
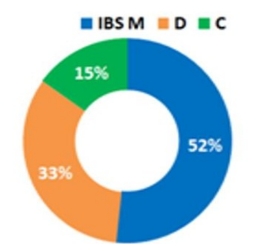
A comparison of type of refractive error found in each of the groups was in our study was done. More number of high myopic children were seen in the laser treated group than in anti VEGF or spontaneously treated as shown in the above graph. Also, more myopic children were seen in Laser group and much less in anti-VEGF group showing better long-term outcome. Results obtained showed more number of emmetropic children in spontaneously regressed ROP (Figure 1).

Anisometropia and refractive errors may be associated with strabismus. In the present study strabismus was seen in 3 subjects (10%) in laser treated group and 2 subjects (6.6%) in spontaneously regressed ROP group. Out of 3 children in laser treated group all 3 eyes had exodeviation and 1 subject developed amblyopia. Those in spontaneously regressed had esodeviation without amblyopia.
The present study discusses the long-term status of refractive errors in children with ROP, as well as how it relates to biometric components. Premature birth may alter normal ocular growth in a variety of ways in both anterior and posterior segments.
In the present study 85 children with history of ROP were subcategorized into as spontaneously regressed ROP (group 1), Laser treated ROP (group 2), and Anti-VEGF treated ROP (group 3).
Understandably, the babies where ROP regressed spontaneously had more birth weight as compared to other groups. The gestational age was also more in this group giving more time for the retina to mature. Hence, at diagnosis most of the babies had ROP in zone 3. 9
In our study visual acuity observed was 0.9 in laser treated group. The reasons for this visual outcome could have been due to late referral, timely management not done, and faster progression of disease, which in turn also resulted in poor structural outcome.
Biometric outcomes in laser treated group were similar to other studies where it was proposed that more chances of high myopia in laser treated ROP contributed to a steep keratometry and a greater LT and a shallower ACD. Our study results show a mean AL of 20.60 ± 0.93 mm despite myopia. The present study corroborates the claim that ablation therapy applied to the whole retina inhibits ocular development, which results in lower AL even when myopia is present. 10 The posterior segment of eye experiences stunted development, for which the anterior segment overcompensates. The mean posterior segment length in our study was found to be 13.48 ± 1.00 mm which is much less with ASL/PSL ratio 0.53 ± 0.07.
We observed a lenticular thickness of 4.26 ± 0.37 mm which can be a contributing factor to myopia. Shallowed anterior chamber would give rise to lens being more anteriorly placed and could account for increased myopia seen in the laser-treated eyes. Most studies show increased lens thickness ranging between 3.81mm to 4.33 mm in support of our findings. Our study revealed an ACD of 2.86 ± 0.26 and a mean keratometry value of 44.01D. We have observed a modest decrease in the ACD and an increase in LT in high myopes.
Mean spherical equivalent in our study was found to be -3.13 ± 1.63 D which signifies more degree of myopia and myopic astigmatism which is similar to other studies. Occurrence of myopia was found to be 93% which was similar to Yang et al.11
The study by Kaur S et al. showed children with spontaneously regressed ROP or prematurity had more myopia and astigmatism which was similar to our study (mean SE in the study was -0.4 D and occurrence of myopia was 69.4%). Mean spherical equivalent in our study was -1.85 D and also occurrence of myopia in this group was 70%. We can conclude that tendency to develop ametropia continue till adolescence.
Flattening of cornea after birth in a full-term child normally makes up for axial elongation occurring thereafter but in children with ROP the flattening of the cornea was less as seen by 1 year of age.12 In contrast study done by Farvardin et al. showed the mean spherical equivalent was not evidently different among the premature children with no ROP, spontaneously regressed ROP, and laser treated ROP. 13
In our study mean AL obtained was 21.41 ± 1.38mm which was similar to AL in study by Farvardin et al. (21.93mm) while AL in Mcloone et al. study was more than the present study. 14
Mean LT and ACD in our study were 3.62mm and 3.23 mm respectively whereas mean ACD in study by McLoone EM et al. was 3.70 mm which is more. Mean keratometry (44.99 D) showed slightly steeper cornea. The results we obtained in the present study support the argument that ROP impacts the baseline magnitude of myopia.
Children that are born at term have emmetropization, which is accompanied with axial elongation and flatness of cornea. 15 In preterm eyes total refractive status may be more heavily influenced by the anterior segment. The present study demonstrates that the posterior segment growth is slowed in children with ROP, and the anterior segment also exhibits reduced corneal flattening. Therefore, in these kids emmetropization doesn't progress normally, therefore myopic tendency continues.
In our study we observed that mean spherical equivalent i.e. -2.08D was less than that in laser group. Also there was lesser degree of myopia seen in anti-VEGF group as compared to laser treated which was similar to result of other studies such as in Milena S. et al. 16 Incidence of high myopia was also less in anti VEGF group than the laser group (although not statistically significant).
Mean ACD observed 3.00 ± 0.26mm which was comparatively deeper in the patients in the anti-VEGF treated group than in the patients in the Laser group (2.86 ± 0.27 mm) similar findings were observed by Lee YS et aland Yen Chen et al. 17, 18 Refractive errors in children with Laser treated ROP have been seen in association with the difference in the anterior segment growth with steeper cornea, shallow anterior chambers, and thicker lenses, not to AL elongation. 19 Pathogenesis of ROP and the changes incurred in the eye due to various treatments restrict the normal process of eye growth eye growth leading to these changes. These changes were not seen anti-VEGF treated ROP in our study. Mean LT was significantly greater in laser treated whereas mean LT in anti-VEGF was less (3.67 ± 0.40 mm). These changes may be attributed to the fact that the treatment process affects the retinal signals and the reception of sclera to these signals required for normal development which in turn causes abnormal development of the anterior segment structures. At birth human lenses are thicker as compared to children and presumably changes in the lens thickness is affected by the retinal laser. 20, 21 Mean AL observed was 21.76 ± 0.98 mm which was more than that observed with laser group. Magnitude or degree of myopia can be attributed to axial component also along with steeper cornea (mean keratometry 45.08 D). In other studies, significant difference was not seen among the anti VEGF treated group and laser treated for AL.
In our study mean PSL of 15.09 ± 1.14 mm was seen in anti-VEGF treated which is much greater than laser group. Laser can cause more stunted growth of posterior segment than anti VEGF. Hence axial elongation can be more in anti VEGF.
In the present study, strabismus was seen in 3 children in laser treated group and 2 children in spontaneously regressed ROP group i.e. 10% in laser treated, 6.6% in spontaneously regressed ROP. Out of 3 children in laser treated group 2 had high myopia and all 3 eyes had exodeviation. Those in spontaneously regressed had esodeviation without amblyopia.
In a study by Burton J. Kushner in 1982 described a series of 38 patients who had history of regressed ROP and those were compared to newborn with similar age of gestation as well as with term baby. Incidence of strabismus was much more in ROP group. Also 6 children in preterm group developed strabismus. Significantly higher incidence was seen in ROP group. 22
In another study by G Holmstrom et al. (1999) Ocular alignment was analysed in 229 children and incidence of strabismus in 3.5 years was highest in children with ROP, in those given cryotherapy (40%), in those with neurological complications (31%). 23
In study by Philippa M et al. in the low birth weight group, the ratio of esotropia to exotropia is 1 to 1, but it is 3 to 1 in full-term infants. Additionally, 12% of strabismus cases were categorised as near exotropia, a rather unusual kind of strabismus. 24
ROP, an increase in refractive error, neurological impairment, and prematurity has all been linked to an increased prevalence of strabismus in preterm infants. 25 Risk factors for strabismus include cicatricial ROP, refractive error, family history, birth weight, anisometropia, maternal age, smoking, ethnic origin, and overall development quotient. 26, 27, 28 Although the cause of strabismus is not well known in general, the significant rise in incidence in the preterm population may point to a shared etiology.
Limitations of the present study were small sample size, not taking into account the laser spot size or time for ROP regression which could have affected the refractive outcome.
The present study found that intravitreal anti-VEGF therapy leads to lower prevalence of high myopia of all grades and better visual acuity compared to laser photocoagulation. Shallower ACD in the laser-treated eyes as observed in our study could lead to the development of angle-closure glaucoma in the future thus requiring regular follow-up. It has been found that anti-VEGF medication and laser photocoagulation are both safe and efficient ways to treat type I ROP. Anti-VEGF medicines may be a viable first-line therapy in some situations, such as eyes with zone I disease or severe posterior ROP. This is because they cause less treatment-related retinal damage and show quicker remission of active ROP and plus disease.
None
None
Subscribe now for latest articles and news.