Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.2021.v07i03.007
Year: 2021, Volume: 7, Issue: 3, Pages: 26-31
Original Article
Saudamini A Naik1 , Amit S Naik1 , Simran A Patel2 , Rajul A Patel3
1Associate Professor, Department of Obstetrics and Gynaecology, SMBT Institute of Medical Sciences, Nashik, Maharashtra, India. Tel.: 9370424274, 2Department of Obstetrics and Gynaecology, SMBT Institute of Medical Sciences, Nashik, Maharashtra, India, 3DNB Paediatrics
Address for correspondence:
Amit S Naik, Associate Professor, Department of Obstetrics and Gynaecology, SMBT Institute of Medical Sciences, Nashik, Maharashtra, India. Tel.: 9370424274. E-mail: [email protected]
Background: This study was conducted in a metropolitan area in Maharashtra (India) to estimate percentage of urban women exclusively breastfeeding their children during 1st 6 months after childbirth & to Assess the factors affecting mothers’ decision to use exclusive breast feeding or Mixed feeding practices during 1st 6 months of childbirth. Methods: This retrospective cross-sectional cohort study among 150 mothers between age group (18-40 yrs.) living in a metropolitan area with regards to breastfeeding practices was conducted by using a self-administrated questionnaire. Results: Out of 150 participants, exclusive breast feeding was done by 39 mothers (26%), while 111 mothers (74%) used mixed feeding. 32.4% mothers having good knowledge of feeding, 32.1% mothers living in joint family & 35.7% mothers delivered vaginally practiced exclusive breast feeding. In this study we found that factors like women living in joint family, good education status, vaginal mode of childbirth, correct knowledge of feeding practices given to them by their health care providers during ANC care are more likely to practice exclusive breast feeding. Conclusion: Health care providers often advice formula/top feed during early period of hospital stay (immediately after delivery) in addition to breast milk due to various reason. Though there are international recommendations support exclusive breast feeding, these common hospital practices can lead to introduction of top feeding in the first weeks of life which are carried forward as mixed feeding practices during 1st year of infancy.
Keywords: Breast Feeding, Lactation, Attitude, Urban population
Feeding practices, in the first year of life, impact the nutritional status of the child, directly affecting his/her health & survival. As our country works towards achieving its commitments to the SDG 2030 (Sustainable Developmental Goals 2030) to reduce Neonatal mortality to at least as low as 12 deaths per 1,000 live births and under-5 mortality to at least as low as 25 deaths per 1,000 live births,[1] adequate nutrition in form of breastfeeding is extremely essential, especially at the very beginning of life. It ensures the growth, health, and development of children to their full potential. Poor nutrition increases the risk of illness, and is responsible, directly or indirectly, for one third of the estimated 9.5 million deaths that occurred in 2006 in children less than 5 years of age. [2]. It is a well-established fact that human milk is the best milk for neonates. World Health Organization (WHO) recommends that infants should be exclusively breastfed for the first six months of life to achieve optimal growth, development and health.[3] Although breastfeeding is the ”gold standard”, not all women breastfeed their infants. About 41% globally and 52% in South Asia are breastfed exclusively from 0 to 5 months of age in 2018.[4] Some mothers might be unable to breastfeed because of medical conditions and some make the choice not to. It is assumed that the uneducated and poor are most likely not to exclusively breastfeed, especially not administer colostrum due to various disbeliefs. [5]However today, educated, urban women have taken a back seat when it has come to breast feeding.[6] Factors like negative attitudes toward breastfeeding, conflicting responsibilities or schedules, convenience, negative breastfeeding experiences, apart from medical reasons are prevalent in the urban society and need to be acknowledged. Keeping the same in mind this study was planned to bring to light the various practices followed, understand & acknowledge the basis for the same so that appropriate intervention can be advised to continue correct breast-feeding practices.
• To Estimate percentage of urban women exclusively breastfeeding their children during 1st 6 months after childbirth.
• Asses the factors affecting mothers’ decision to use exclusive breast feeding or Mixed feeding practices during 1st 6 months of childbirth.
This retrospective cross-Sectional cohort study among mothers of a metropolitan area with regards to breastfeeding practices was conducted after obtaining ethical clearance from Institutional Ethics committee and Informed consent from eligible participants. The study includes 150 mothers whose children, at the time of study, were aged more than 6 months and less than 12 months of age. Exclusive breastfeeding means that the infant receives breast milk (including expressed breast milk or breast milk from a wet nurse) and allows the infant to receive ORS, drops, syrups (vitamins, minerals, medicines), but nothing else.[7]
Sample size: 150 participants (Random method of sampling) form Out Patient Department of private Mother & child clinics in a metropolitan city.
Study Duration: 6 months (1.02.2019 to 31.07.2019)
Inclusion criteria: Mothers aged between 18-40 yrs. whose children, at the time of study, were aged more than 6 months and less than 12 months of age, had breast fed their recent child & willing to give consent to participate in the study and answer all questions.
Exclusion Criteria: Mothers having lactation failure due to underlying medical reasons, in whom breastfeeding is contraindicated, due to any maternal or neonatal reason or residing in rural area.
The questionnaire for data collection was administered to the participant in their local language and response noted at their OPD visit. Basic instructions were given to them and care was taken that there will be no influence, by any idea or thought, regarding the said ideal methods of lactation.
The questionnaire had 3 parts
. Family background (variables such as health of mother, lifestyle of the parents and their socio-economic status).
. Knowledge, attitude & awareness (Normal breastfeeding habits and its dos and don’ts by answering true or false questions).
. Feeding Practices, which studied the actual breast-feeding method (Exclusive breast-feeding vs Mixed feeding practiced) by the participant, and factors affecting it.
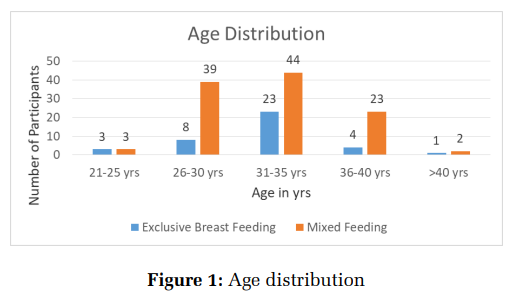
In a study by Al Ketbi et al[8] it was found out that maximum participants were in the age group of 25-29 yrs. however in our study maximum participant mothers, 67 mothers (44.6%) were in the age group of 31-35 yrs. signifying delayed child bearing amongst girls of metropolitan cities due to education, career and delayed marriages. In the various age groups exclusive breast feeding was done by 39 mothers (26%) out of 150, while 111 mothers (74%) used mixed feeding i.e., breast feeding plus top feeding. (Chi square-8.02, P=0.09). Thus, showing that as per various age groups of the mothers no differences were found in exclusive breast-feeding practices. In a study by Singh M.B et al[9] they found that in rural area of Rajasthan only 23% mothersinitiated breast feeding in first 3 days of childbirth and 80% mothers were illiterate and from lower socioeconomic background however in our study all 100% mothers had initiated breast feeding during this period and only 2% were illiterate. In a study by Patro S et al[10] they found that almost 60% mothers living in tribal belt of Orissa discarded the nutritious and immunoglobulin rich colostrum during first 24 hrs. and started prelacteal feeds, exclusive breast feeding was given later which was then continued for 1 year.
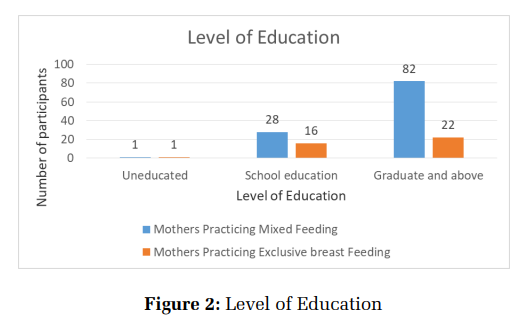
In our study as the level of education increases (graduation and more 69%) a greater number of mothers opted for mixed feed. It was observed 82 (78.8%) out of 104 mothers with education more than graduation used mixed feeding. In school educated mothers 28 (63%) out of 44 used mixed feed. In uneducated the number was same. (Chi square4.32, P=0.11). As Education increased the percentage of mothers adopting mixed feeding increased but statistically it remains insignificant.
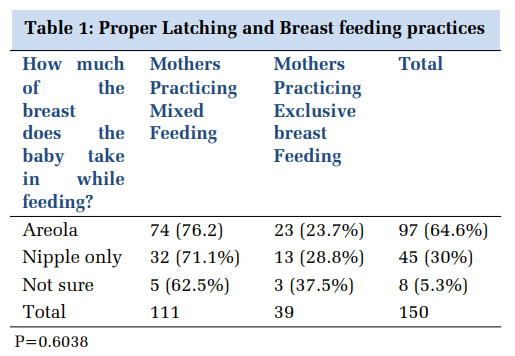
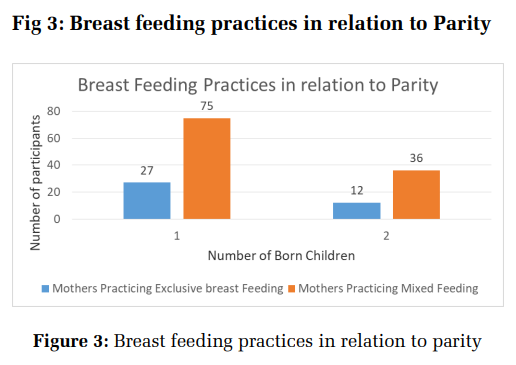
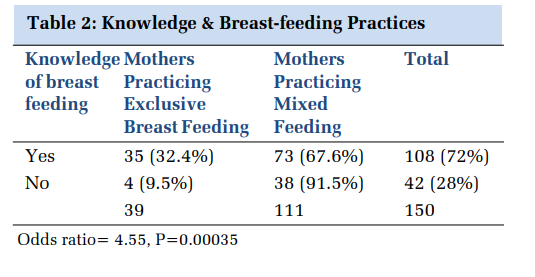
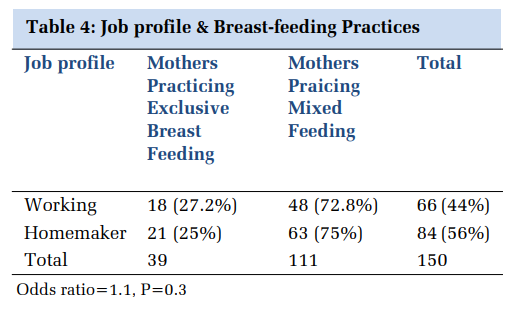
97 mothers (64.6%) out of 150, properly latched the baby on to the breast but amongst them 74 (76.2%) still fed babies with mixed feed as they felt the baby’s requirement was not fulfilled by breast milk alone. Similar percentage of Primi-para (27 (26%) out of 102) and second-para (12 (25%) out of 48) exclusively breast fed their babies rest used mixed feeding. Odds ratio 1.08. This signifies the fact that as per our study parity is not related to exclusive breast-feeding practices 108 mothers (72%) out of 150 had good knowledge of feeding practices, amongst them 35(32.4%) mothers exclusively breast fed their babies rest (67.6%) used mixed feed. 4 (9.5%) mothers out of 42 practiced exclusive breast feeding in spite of having no knowledge about feeding practices. Odds ratio=4.55, P= 0.00035. The source of knowledge as per our study was, health care providers (60%), Family member (60%) & Newspaper, Television and internet was responsible for (50%). As per this study knowledge of correct breast-feeding practices & its advantages increases exclusive breast-feeding practice amongst mothers. In the study by Al Ketbi et al[8] they had divided knowledge component into Good (51%), Fair (43%) and poor (5.5%) and the source of knowledge was Family (66%), Doctors (58%), internet (40%) and nurse (50%).
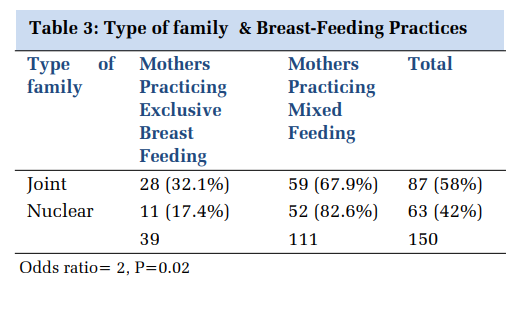
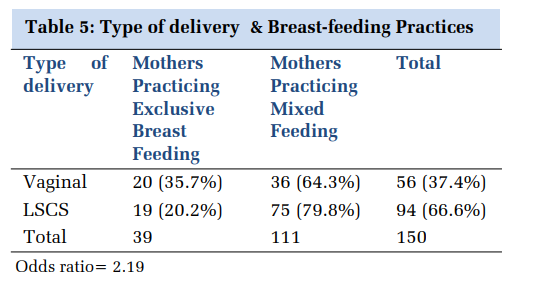
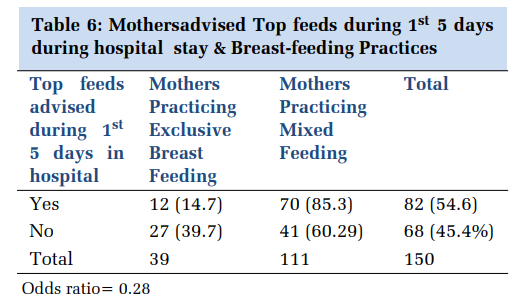
87(58%) mothers lived in joint family out of them 28(32.1%) practiced exclusive breast feeding and 11 (21.1%) out of 52 mothers living in nuclear family practiced exclusive breast feeding. Odds of exclusive breast feeding in mothers living in joint family is 2 and the p=0.02 which is significant. As per this study mothers living in joint family are more likely to do exclusive breast feeding practices as many people are around to help in household work thus giving mother more time to look after the newborn. 20(35.7%) mothers out of 56 delivered vaginally were practicing exclusive breast feeding as compared to 19(20.2%) out of 75 delivering by Caesarean section. Odds of 2.19 tells us that mothers delivering vaginally are more likely to exclusively breast feed the baby. 82(54.6%) mothers were advised top feeds during 1st 5 days of hospital stay (immediately after delivery) in addition to breast milk due to various reason like less milk (colostrum), dehydration of baby, operative pain and of them 70(85%) mothers continued mixed feeding however of the 68(45.4%) mothers not receiving any such advice 41(60.3%) started mixed feeding practices. Odds of 0.2 suggesting that mothers who were never advised top feeds are more likely to practice exclusive breast feeding.
The urban settings differ a lot from rural settings in breast feeding practices like absence of use of prelacteal feeds/ early initiation of breast feeding[8–10]and, In urban settings social and cultural beliefs have a less influence but ease of feeding considering working women living in nuclear family, Affordability & ease of availability of Top feed formulations, good hygiene practices influence a lot of mothers on the practice of exclusive breast feeding. Women in metropolitan city have an easy option of top feeding to exclusive breast feeding making mixed feeding that is top feed along with breast feed practiced more.
In a study by Al Ketbi et al[8] they found that correct breast-feeding knowledge was present in mothers with education above graduation, living in joint family & having a single child. They also found that working mothers, advice of top feeds by health care providers, mothers having no past experience of breast feeding, were more likely to use mixed feeding practices. In our study we have assessed many variables like age, parity, education, knowledge of breast feeding, working/non-working mother type of family, mode of delivery and advice of health care providers. On data evaluation it was observed that mixed feeding is practiced more than exclusive breast feeding. Only 39(26%) mothers out of 150 recruited mothers practiced exclusive breast feeding, whereas 111 (74%) mothers practiced mixed feeding. In our study we found that women living in joint family, Education status, vaginal mode of childbirth, correct knowledge of feeding practices given to them by their health care providers during ANC care practiced exclusive breast feeding.
The findings of our study are similar to study by Vyas[11] which states that in India Breast feeding practice is universal, however exclusive breast feeding is far from desirable. In our study use of prelacteal feeds is reducing but use of top feeds and mixed feeds is increasing in urban locality in spite of good knowledge about correct feeding practices. In their study[11] carried out in rural India only 5.3% children were exclusively breast fed which is very low as compared to our study of 26% exclusive breast feeding. In another study[12] carried out in urban slums of south India it was found that 59% newborns received breast feeds within first hour of birth and 22% received exclusive breast feeding for first four months of life which is comparable to our study result. In both the studies[11,12] there was no significant feeding difference in terms of duration and exclusive breast-feeding practices with respect to the sex of the newborn. Breast feeding is a natural act; however, it needs help from caregivers and motivation from health care workers for optimum practice,[13] this is proved in our study also as the women living in joint families were more likely to practice exclusively breast feeding due to help from family members and also in those women in whom breast feeding was initiated in first hour of delivery. Khan M[14] in his study found that the frequency & practice of exclusive breast feeding reduced in working women at 4-6 months however in our study no such significant difference was found.
Health care providers often advice formula/top feed during early period of hospital stay (immediately after delivery) in addition to breast milk due to various reason like less milk(colostrum), dehydration of baby & operative pain in order to prevent infant morbidity (i.e., infant weight loss, dehydration, jaundice) arising from decreased feeding by/from the mother. Though there are international recommendations and goals to support exclusive breast feeding, these common hospital practices can lead to introduction of top feeding in the first weeks of life which are carried forward as mixed feeding practices during 1st year of infancy.
The importance of exclusive breast feeding is universally well recognized still exclusive breast feeding is not widely practiced. We conducted this retrospective study on a small sample size of 150 participants covering a single metropolitan area. A prospective study on a larger sample size involving multicentric approach covering many different metropolitan areas will help us to understand the breast-feeding practices in-depth and help us develop strategies to plan and promote exclusive breastfeeding practices effectively.
Subscribe now for latest articles and news.