Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.v10.i2.23.106
Year: 2024, Volume: 10, Issue: 2, Pages: 183-189
Original Article
Prakash Jha1 , Ratnesh Kumar2 , Siddhartha Yadav3 , Shivendra Singh4 , Shakeel Ahmad Quidwai2
1Senior Resident, Department of Orthopaedics, Hind Institute of Medical Sciences, Mau, Ataria, Sitapur, 261303, U.P, India,
2Professor, Department of Orthopaedics, Hind Institute of Medical Sciences, Mau, Ataria, Sitapur, 261303, U.P, India,
3Assistant Professor, Department of Orthopaedics, Hind Institute of Medical Sciences, Mau, Ataria, Sitapur, 261303, U.P, India,
4Associate Professor, Department of Orthopaedics, Hind Institute of Medical Sciences, Mau, Ataria, Sitapur, 261303, U.P, India
Address for correspondence:
Ratnesh Kumar, Professor, Department of Orthopaedics, Hind Institute of Medical Sciences, Mau, Ataria, Sitapur, 261303, U.P, India.
E-mail: [email protected]
Received Date:01 April 2023, Accepted Date:20 April 2024, Published Date:15 July 2024
Objective: The study is aimed at comparing the outcome of management of DERFs by close reduction and immobilisation by POP cast (CRIPOP) vs. close reduction and immobilisation by intrafocal pinning (K-wire), Kapandji technique. Material and method: 80 patients with DERFs (Frykman I&II/AO23AR) aged 19–68 years, both sexes, and sides (left or right) of involvement were studied at the Department of Orthopaedics, HIMS, Sitapur (U.P.), India, after getting clearance from the institute's ethical committee. The individual's identification, history, clinico-radiological evaluation (pre- and post-op), and follow-up were recorded in a pretested proforma. A standard protocol of pre- and post-operative care and physiotherapy was followed by all patients, irrespective of group. Results: To assess the functional outcome, cases were followed up at 6 weeks, at the time of removal of POP, at 12 weeks, and at 24 weeks. The objective assessment was done on parameters like wrist movement, i.e., palmer/dorsiflexion, radial/ulnar deviation, wrist/finger stiffness, supination, and pronation in forearm functions. The functions were compared with other limb functions. Subjective parameters such as pain, ADL, and work-related activities (satisfaction level) were also taken into account. The difference in distribution among groups was insignificant. Other than a pinhole infection and finger stiffness, there was no significant complication. Conclusion: CRIPOP was found to be an equally better option of treatment methodology in respect of functional outcome at 6 months in extra-articular (Fryman types I and II) or AO/OTS (23A2 and 3). The limitation of the study is the small number of cases and parameters to compare.
Keywords: DERF, CRIPOP, Kapandji, Focal Pinning
The fracture at the distal end of the radius (DERFs) is common in all age groups, more so in the elderly. DERF in the elderly (Colle’s fracture) was first described by Abraham Colle’s in 1814. The rate of unsuccessful treatment and related morbidities in colle’s fractures is high. 1, 2, 3 The majority of such fractures are extra-articular (2R3A2.2). 4, 5 A perfect reduction in terms of alignment of the metaphysis, ulnar variance, radial height, inclination of the radius, and palmar tilt is key to a successful functional outcome.
As per studies undertaken, wrists can become pain-free and obtain good functional flexibility in all ranges of motion, with or without intervention. Treatment modalities for DERFs include interlock nailing, external fixators, close reduction, cast application, etc. Despite advancements in conservative management of DERFs, the primary close reduction (CR) and cast immobilisation method is still the 6, 7
In conservative management, the close reduction and immobilisation followed by physiotherapy is a common and standard practice, but to get the best functional outcome, a perfect reduction and maintenance of the reduced distal fragment by the Kapandji technique (closed reduction) using k-wire were first tried in 1976. During the fracture-healing phase, the intrafocal pinning used in reduction is maintained along with a below elbow plaster of Paris (POP) cast for six weeks post-reduction (Kapandji technique). 8, 9, 10 The Kapandji technique is often appropriate for intra- and extra-articular fractures with a single fracture line and displaced two-part Colle’s fractures without the involvement of the articular surface.
The study is aimed at evaluating functional outcome and related complications of treatment modalities for fractured distal end radius, including close reduction and immobilisation by plaster cast vs. Kapandji technique.
The study was conducted in the Department of Orthopaedics at the Hind Institute of Medical Sciences, Sitapur (U.P.) of northern India, after getting clearance from the institute's ethical committee. Out of 110 cases screened from January 2021 to June 2022, only 80 were found fit to our pre-determined criteria and were included in the study. Such study cases were extra-articular, closed fractures (DER), aged 18 years and above, medically fit for surgery (intrafocal pinning), and without any musculoskeletal and/or neurovascular injury in the same limb. Such selected 80 cases were divided into two groups of 40 each. It was a prospective comparative study. The identified patients were explained the above treatment options, with their merits and demerits, leaving the choice of procedure to them. Accordingly, two study groups (A and B) were formed and managed by-
Group A: closed reduction and immobilisation by POP Cast (CRIPOP).
Group B: CR, intra-focal pinning, and POP casting (Kapandji Technique).
Either procedure was carried out with the written and informed consent of the patients. A minimum of six months of follow-up after treatment and the removal of the POP cast was included in the study.
The patient's identification details, history, and clinico-radiological evaluation were done and recorded (in English) on the pretested proforma. A general and systemic examination was preceded the thorough local examination. In the local examination, deformity, oedema, and ecchymosis, the relative positions of the radial and ulnar styloid processes, pain, crepitus, and bony irregularity were elicited. The wrist and forearm movements, radial artery pulsations, pallor, and paraesthesia were seen and recorded. Preoperatively, the affected forearm was immobilised in a POP slab below the elbow, irrespective of the treatment option.
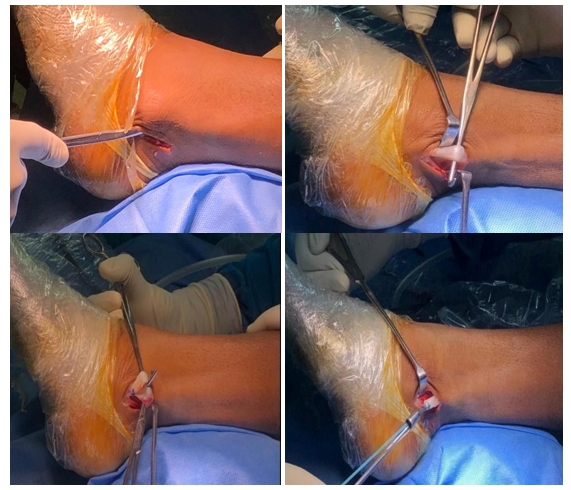
Patients in Group A received CRIPOP under analgesia or short GA, while patients in Group B received Kapandji technique and below elbow POP casting with a regional block. In patients of both groups, a perfect reduction was done under the C-arm, and patients were immobilised for six weeks in a neutral position with standard post-op care and physiotherapy protocols. (Figure 1)

In Group-B cases, k-wires of 1.5–2 mm thickness used to manipulate and hold the fragment were removed after 6 weeks (1.5 months). (Figure 2)

A clinico-radiological evaluation was done at 6, 12, and 24 weeks (1.5 months, 3 months, and 6 months) for the outcome, function in particular, and recorded. In radiological evaluation (PA and lateral views of the wrist in neutral position), callus formation, bone union, radial length and inclination, and volar tilt were evaluated for anatomical restoration. While functional evaluation was done in detail, it included pain, swelling, stiffness, and range of motion of the wrist joint (palmar/dorsal flexion, radial/ulnar deviation, and supination/pronation compared to the other limb).
The collected data were tabulated and analysed statistically. Quantitative variables will be represented in terms of mean standard deviation. Categorical or nominal data were expressed as frequency or percentage. The student’s unpaired ‘t test was used for continuous variables with normal distribution. For the comparison of categorical variables, the Chi-Square test was used. Statistical significance was defined as a p-value of 0.05.
The study population (80) was divided into two groups, A and B, of 40 each, with patients ranging in age from 19 to 68 years. The mean ages of patients in Group-A (CRIPOP) and Group-B (Kapandji Technique) were 45.52±14.08 and 43.18±12.24 years, respectively. The difference in age between Gr. A and Gr. B was not significant (p > 0.05). Similarly, the difference in the distribution of patients in groups according to their sex and side involved was found to be significant (p > 0.05). (Table 1)
|
Age distribution |
|||||
|
Group / Age (yrs ) |
Group-A (Gr.-A) Closed reduction & immobilization by POP cast (CRIPOP) |
Group-B Gr.-B) Close reduction with intrafocal pinning with POP cast (Kapandji) |
|||
|
mean ± SD
|
45.52 ± 14.08 |
43.18 ± 12.24 |
|||
|
|
p-value1 |
0.42 |
|||
|
Sex & side involved, Distribution |
|||||
|
Sex / Side
|
Group-A (n=40)
|
Group-B (n=40)
|
p-value1
|
||
|
|
No.
|
%
|
No.
|
%
|
|
|
Sex |
|
|
|
|
|
|
Male |
16 |
40.0 |
20 |
50.0 |
0.36* |
|
Female |
24 |
60.0 |
20 |
50.0 |
|
|
Side |
|
|
|
|
|
|
Left |
23 |
57.5 |
20 |
50.0 |
0.50 |
|
Right |
17 |
42.5 |
20 |
50.0 |
|
1Unpaired t-test, *Chi-square test
Based on Frykman type and AO/OTS classification, the difference between patients in groups A and B was insignificant (p>0.05). (Figure 3)

On comparison of forearm functions (pronation and supination) between patients of groups at 6, 12, and 24 weeks, pronation was significantly better in group A as compared to group B at different stages of follow-up during the initial 6 months (p = 0.001), while supination was significantly less among patients of group A (CRIPOP) as compared to cases of group B (Kapandji) (p=0.001). (Table 2)
While the compared movement of the wrist (palmar/dorsal flexion) between the groups at 6, 12, and 24 weeks, no significant difference was found (p > 0.05), patients were able to perform all activities requiring palmer and dorsal flexion of the wrist at the end of 6 months of follow-up.
|
Pronation outcome |
Supination outcome |
|||||
|
Time period |
Gr.A (n=40) |
Gr.B (n=40) |
p-value 1 |
Gr.A (n=40) |
Gr.B (n=40) |
p-value 1 |
|
6 wks |
60.62 ± 4.26 |
65.50 ± 5.40 |
0.001* |
60.62 ± 4.26 |
65.50 ± 5.40 |
0.001* |
|
12wks |
65.38 ± 4.44 |
69.98 ± 5.39 |
0.001* |
65.38 ± 4.44 |
69.98 ± 5.39 |
0.001* |
|
24 wks |
65.25 ± 4.22 |
70.52 ± 5.37 |
0.001* |
65.25 ± 4.22 |
70.52 ± 5.37 |
0.001* |
1Unpaired t-test, *Chi-square test
Ulnar deviation in patients in Group A was significantly less than in Group A at 24 weeks follow-up. (p = 0.001), but the radial deviation between patients in groups A and B was insignificant (p>0.05) (Figure 4).

Wrist and finger stiffness was present in 12.5% of patients in group A as compared to 10% in group B and was insignificant (p > 0.05).
The pin tract infection was mild, seen in 12.5% of patients in Group A, and was healed in a week's time.
The distal end radius fracture is one of the most common fractures encountered in the orthopedic emergency room. 11 Inadequate reduction and management results in mal-union, which causes discomfort, poor grip strength, stiffness, carpal instability, and degenerative arthritis later. 12 There are numerous treatment options for DERFs, including CR and immobilization by POP cast, reduction, and immobilization by trans-radial styloid pinning via the Lister's tubercle or trans-ulnar pinning, reduction/manipulation, and fracture hold by percutaneous intrafocal pinning (K-wire) and POP cast (Kapandji technique), open reduction, and fixation with a volar or dorsal plate. But none of the above is accepted as the standard. To decide the treatment option, the age of the patient, lifestyle, functional requirements, hand dominance, associated health conditions, type of fracture, alignment, soft tissue condition, resources, and facilities available, etc. have to be taken into account. 13
The perfect anatomical reduction and stability of the fractures determine the functional outcome. In undisplaced and stable DERFs, little to no immobilization is required as re-displacement is unlikely to happen. 14
The use of percutaneous K-wire is a common treatment strategy for fracture stabilisation, as it is less invasive, relatively rapid, straight forward to perform, affordable, and acceptable to patients. Post-reduction, the duration of cast immobilization can be minimised. However, a need for additional surgery to remove pins and related problems, such as tendon ruptures and re-displacement of the fracture, cannot be ruled out. 11
In the present study, either Modality, namely, the CRIPOP cast or the Kapandji technique was applied to 40 patients in its group, and the results have been studied and compared in terms of functional outcome.
The age range was from 18 to 68 years, with an average age of 44.4 years. The mean ages of cases in Gr. A and Gr. B were, respectively, 45.52±14.08 and 43.18±12.24 years, thus without any significant difference in age (p > 0.05). More than half of the patients in Gr. A and Gr. B were female; therefore, the difference in the male-to-female distribution was also insignificant (p > 0.05). Our findings are similar to those of other studies, which reported mean ages with a standard deviation of 40.66±16.72 and 48.81±14.65 respectively, where the mean ages were 42.03 years. 15, 16
As per fracture side involvement, the left side was involved in 57.5% and 50% of Gr. A and B, respectively, were insignificant (p > 0.05). Singh J. et al. (1921) reported significantly higher right-side involvement without any specific region except the right side being the dominant extremity and coming forward to protect against the fall or to protect the body from injury. 16
As per the AO classification, patients (23-A2) in grades A and B were 55% and 67.5%, respectively, and the distribution difference was insignificant (p > 0.05). On the Frykman classification distribution, half of the patients in Gr. A and B were Frykman type I, thus without significance (p>0.05) as compared to studies by Subash Y. (2018) and Singh J. (2021), which reported 54.5% and 33.3% (Frykman types I and II), and 4.5% and 17.9% in Frykman types VII and VIII, respectively. 15, 16, 17
In all patients, irrespective of group and treatment modality adopted, the functional outcomes at 24 weeks of follow-up were good or excellent.
Salem A. A.-E. A et al. (2022) reported that the Kapandji method of K-wiring was a successful way of reducing the fracture and maintaining it reduced over time, even for fully displaced fractures. A close reduction might be attained with little effort. 18 It is in accordance with our observation; however, our experience was limited to Frykman types I and II only.
This study showed equally good outcomes for functions of the wrist and forearm, viz., pronation and supination, which were significantly higher (p = 0.001) among Gr-A, however, the palmar flexion difference in groups was insignificant. The dorsiflexion was significantly higher (p = 0.03) among patients of CRIPOP (Gr.-A) than Kapandji technique (Gr-B) initially and for the next 12 weeks.
Bansal H, et al. (2020) reported functional outcomes with good to excellent results in cases treated by close reduction and k-wire fixation with a p-value of 0.00054 (by one-way ANOVA test) using the Gartland & Wherley functional scoring system after a six-month follow-up. It was concluded that K-wire was more reliable and efficient, with fewer complications and better functional outcomes as compared to non-operative means for treating DERFs. 19 We could not compare our findings because we did not use the scoring system.
We noted that ulnar deviation was significantly lower (p = 0.001) in Group A than Group B at only the 6-week follow-up. There was an insignificant (p > 0.05) difference in radial deviation between the groups at all stages of follow-up.
In the study, we noted wrist or finger stiffness in 12.5% of patients with group A compared to 10% of group B patients. This difference could be attributed to patients who sincerely follow post-op instructions and do finger exercises during a cast. The surgical intervention is usually taken more seriously by the patients than by conservative management. However, the difference was insignificant (p > 0.05). Pin tract infection was in 12.5% of patients in Group-A and was healed in a week's time, with no such likelihood in Group-A. Other studies also reported a minimal number of problems while providing a stable fixation and satisfactory functional result with the Kapandji technique in such DERFs. Other studies found that except for pin tract infection and joint stiffness, pin migration, and CRPS were the major complications reported by others that were not seen in our series. 16
Sai Vikranth P. (2018) and Singh J. et al. (2022) compared CR, pinning with POP (Group A), and CR and POP immobilization (Group B) at six-month follow-up and reported that the CR and K-wire stabilization produced slightly better functional results than closed reduction and cast application. If patients are carefully selected, CR and casting may be a simple, non-invasive, and safe approach to treating DERFs. Another study showed good outcomes in 40% of cases and excellent to good outcomes in 90% of cases with internal fixation. 16 The overall findings of significantly better functional outcomes in cases managed by close reduction and pinning against close reduction and immobilization by many authors are not in accordance with our findings, where close reduction and immobilization by POP casting (CRIPOP) have been found equally good and better at many parameters and functions. It may be due to the fact that the operating surgeons in our study had long experience in conservative management, whereas the surgeons involved in dealing with the Kapandji technique were young and had less experience. The additional risks of pin-related complications, radiation exposure, operation-related complications, and resources are no longer in CRIPOP. Further sample size and parameters used for comparison were limited, and outcomes are only for the short term (six months), not the long term.
The functional outcome of management of DERFs by CRIPOP vs. Kapandji was studied in 80 patients of both sexes, irrespective of side and type (Fryman types I and II or AO/OTS 23A2 and 3), aged 19–68 years. At the six-month follow-up, CRIPOP showed an equally good functional outcome without the risk of pin-related complication, additional x-ray exposure, or resource requirements of the Kapandji technique. However, a larger number of cases and a longer duration of follow-up in the study are recommended.
The study was approved by the institutional ethics committee under the project no.EC-HIMSA/MD/MS(20)/RD-10/01-21.
Subscribe now for latest articles and news.