Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.2020.v06i02.010
Year: 2020, Volume: 6, Issue: 2, Pages: 50-53
Case Report
Imran Ahmad1, Lalit Agrawal2, Khurram MF3, Naveen Khubchandani2
1Professor, Department of Plastic Surgery, Jawaharlal Nehru Medical College and Hospital, Aligarh, Uttar Pradesh, India, 2Resident, Department of Plastic Surgery, Jawaharlal Nehru Medical College and Hospital, Aligarh,
Uttar Pradesh, India, 3Associate Professor, Department of Plastic Surgery, Jawaharlal Nehru Medical College and Hospital, Aligarh, Uttar Pradesh, India
Address for correspondence:
Dr Lalit Agrawal, F166/1 SBI Flats Rajouri Graden, New Delhi - 110 027, India. Phone: +91-9711532815. E-mail: [email protected]
Extensor tendon injuries are much commoner when compared to flexor tendons. Extensor tendon injuries can cause serious functional loss if not repaired on time. Injured tendon should be repaired immediately to avoid tendon shortening which can cause flexion lag after repair of injured tendon. We are reporting a case of extensor tendon injury in a 26-year-old female who suffered injury over her right wrist by glass bangle. She presented a month after injury. She suffered right-hand extensor zone VII injury with involvement of middle and ring finger extensor digitorum communis tendons. The method of surgical repair and post-operative regime had given a good functional outcome in our case. However, timely intervention would have resulted in the primary repair of tendon instead of tendon graft as required in our patient.
KEY WORDS:Extensor tendon injury, glass bangle, pulvertaft repair, zone VII injury.
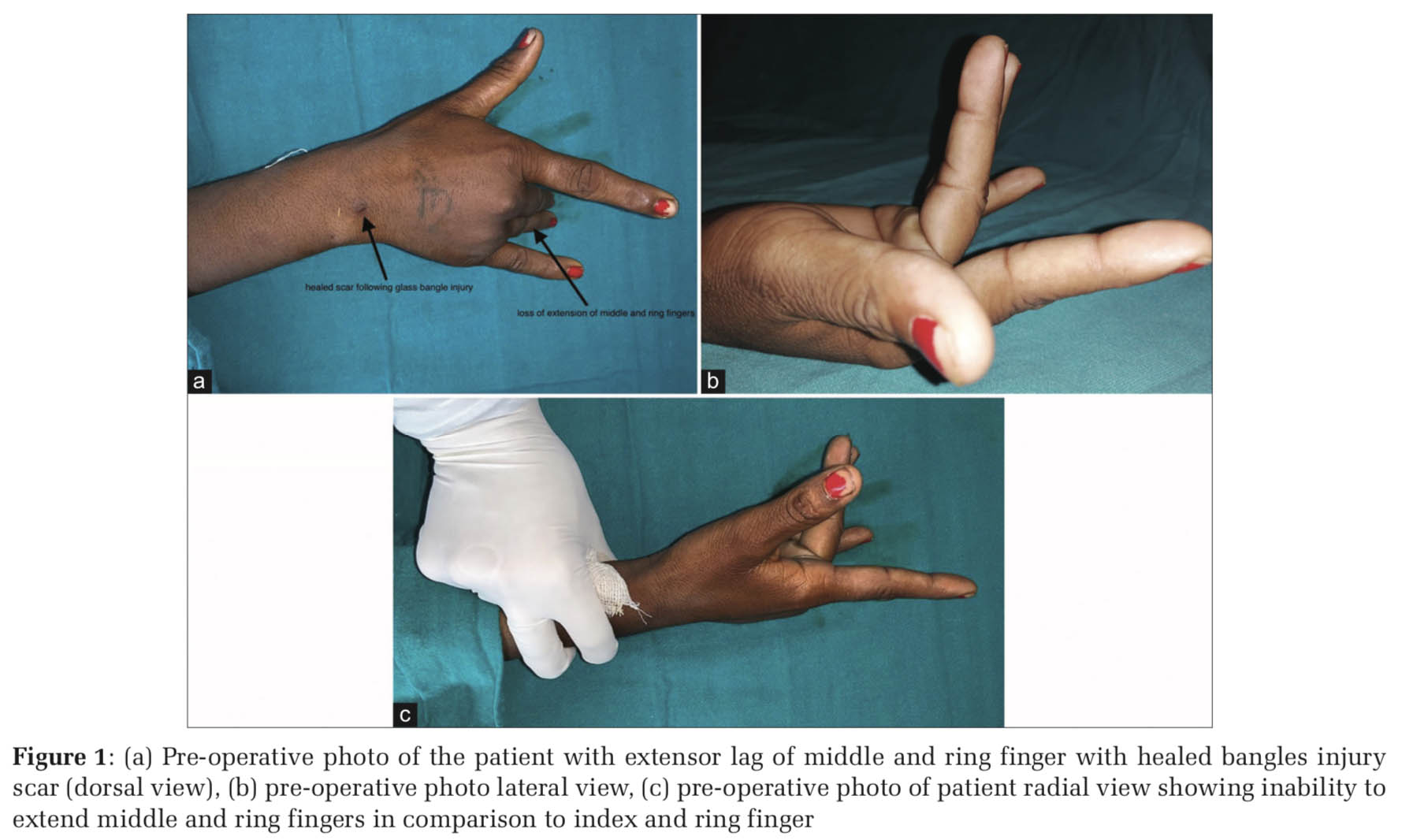
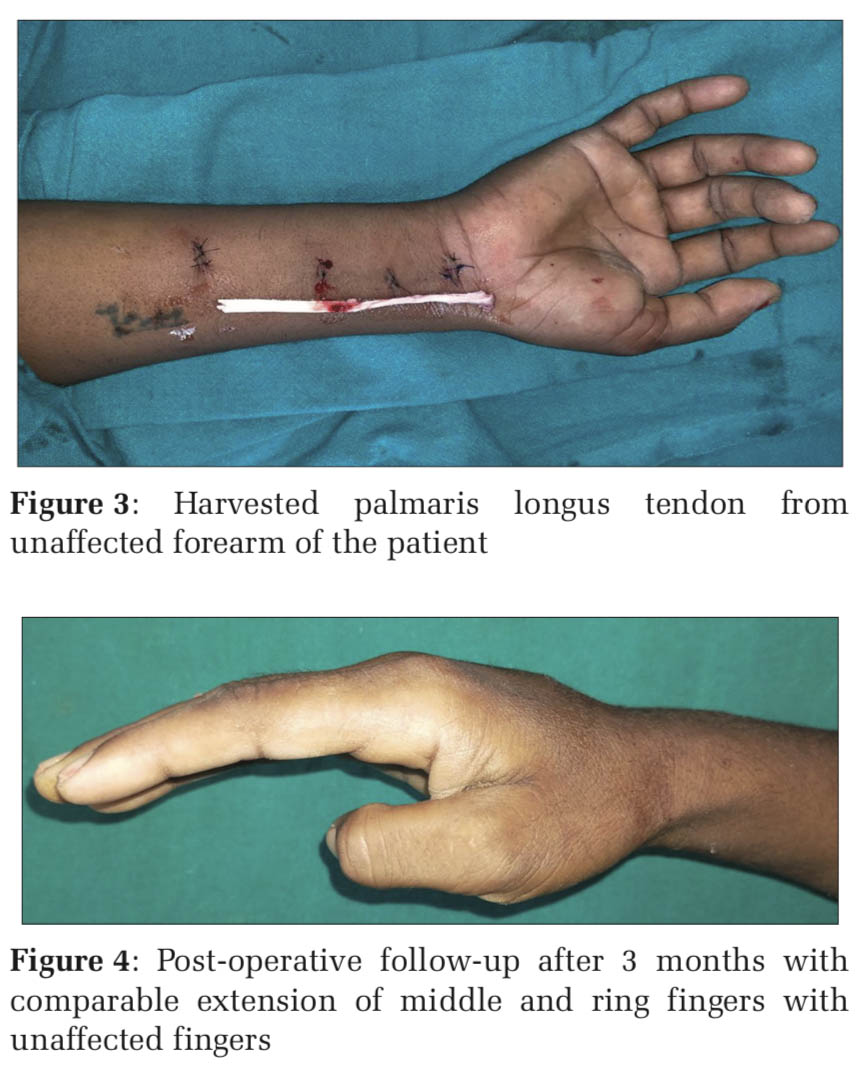
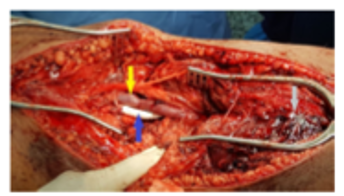
IntroductionExtensor tendon injuries are much commoner than flexor tendon injuries.[1] Lack of subcutaneous tissue and superficial location predisposes them to injuries.[2] Despite being more frequently injured, less attention to extensor tendon injuries are given in the literature.[3] Kleinert and Verdan divided extensor tendons injuries into eight zones.[4] Verdan defined eight zones with odd-numbered being on joints and even number in between increasing from distal to proximal.[5] Extensor tendon is more difficult to repair due to their small size as compared to flexor tendon. Extensor tendons lack collagen bundle linkage, leading to decreased grip strength available for the tendon suturing.[6] Penetrating hand injuries are much commoner nowadays. Sometimes, these tendon injuries may go unnoticed initially and later present with significant fibrosis and retraction with shortening of the proximal fragment. We are reporting a case of a 26-year-old female with bangle injury to extensor zone VII. To the best of our knowledge, no such patient with bangle injury to extensor tendons has been reported in the literature. Case ReportA 26-year-old female presented to plastic surgery outpatient department with inability to extend middle and ring finger of the right hand. She was a homemaker and was right-handed person. On detailed history, she gave a history of accidental injury to the right wrist dorsum with glass bangle 1 month back. As the injury was minor and the patient was not aware, where to get treated for this injury, she went to some quack for the initial management. The wound was regularly dressed, and subsequently, it healed. However, later she noticed her inability to extend right-hand middle and ring fingers. On examination, there was healed scar on dorsum of the right wrist in extensor zone VII (4th extensor compartment) of the size of 1 cm × 0.6 cm. The patient was completely unable to raise her right middle and ring finger (Figure 1a-c). She had normal blood counts, erythrocyte sedimentation rate, and other pre-operative investigations. Ultrasound report showed a complete defect in the extensor tendon of middle and ring finger right hand at the level of the wrist. The proximal torn end was lying at the level of distal forearm and the distal end close to metacarpals base (Figure 2). The distance between torn ends was 8.5 cm. Intraoperatively, 7 cm gap was noted between the proximal and distal end of extensor digitorum communis tendons of the right middle and ring finger. Both the torn ends were dissected to free them from adhesions and bring close to each other. Fourteen centimeters, palmaris longus tendon graft was harvested from ipsilateral forearm (Figure 3). The graft was divided into two halves one for each injured tendon. Pulvertaft repair was done at proximal and distal end of both the injured tendons. Postoperatively, below elbow splint was given with wrist in 30-degree dorsiflexion and metacarpophalangeal joint in 20-degree flexion with interphalangeal joints completely extended. Now, the patient had completed 12 weeks postoperatively and had satisfactory extension of injured digits when compared to uninjured digits; however, some degree of extension lag is still present (Figure 4). DiscussionThe forearm injuries can injure various components of forearm affecting the functionality of the hand. An accurate and timely diagnosis of extensor tendon injury can prevent a patient from being functionally incapacitated.[7] Detailed history elucidating mechanism of injury, position of fingers during injury, and handiness are necessary while planning the management. Appropriate investigations such as ultrasound or magnetic resonance imaging (if required) should be carried out to know the level of injury, gap between torn tendon ends. Either conservative or surgical treatment can be an option depending on the zone of injury. In our patient, she had injury in zone VII of extensor tendon with functional disability, so surgical option was chosen. Long-term results of extensor tendon repair show 63–83% favorable results in proximal zones (5–8) with < 50% good results in distal zones (1–4).[8] Post-operative rehabilitation plays an equally important role in management. In our patient, passive extension with active flexion exercises was started 48 h postoperatively, which was changed to controlled active extension at 4 weeks. Chester et al. compared early active mobilization with early controlled mobilization in extensor zone IV–VIII. He found better range of motion in patients with the early controlled mobilization.[9] Depending on the duration of the presentation, like our patient presented 1 month after injury, the primary repair of tendon may not be possible. In such cases, free tendon graft is the modality of management.[10] Other treatment options could be suturing the distal torn end of extensor tendon to the adjacent intact extensor tendon in side to side fashion. However, in that case, independent motion of the affected digit will not possible as achieved in our patient.[11] Another option can be a tendon transfer, in which extensor indicis proprius and extensor digiti minimi can be used for extensor digitorum communis of the middle finger and ring finger. Such option should be used when the proximal muscle belly is non-functional or fibrotic.[12] Furthermore, the harvest of extensor indicis proprius leads to decrease in isolated index finger extension strength.[13]
|
ConclusionWe, in this study, found how severe can a bangle injury be. Bangle trauma, although seems to be minor, had caused a serious injury in our patient. Every clinician should be vigilant and should not neglect minor injuries. If she would have attended or referred timely to plastic surgeon, primary repair of tendon would have been done. The functional morbidity, which the patient had suffered due to lack of proper initial treatment, could have been reduced. |
Subscribe now for latest articles and news.