Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.v8i1.21.125
Year: 2022, Volume: 8, Issue: 1, Pages: 59-64
Original Article
Praveen Panicker1 , Thomas Iype2
1Assistant Professor, Department of Neurology, Government Medical College, Thiruvananthapuram, 2Professor and HOD, Department of Neurology, Government Medical College, Thiruvananthapuram
Address for correspondence: Praveen Panicker, Assistant Professor, Department of Neurology, Government Medical College, Thiruvananthapuram.
E-mail: [email protected]
Background: Sonologic evaluation of the median nerve has been shown to be a useful tool in carpal tunnel syndrome diagnosis. Neurosonology supplants clinical and electrodiagnostic work up. Objectives: To determine the median nerve ultrasound parameters in carpal tunnel syndrome (CTS) patients and find their correlation with patient reported clinical data and electrophysiology findings,to assess diagnostic accuracy of nerve ultrasound in CTS in comparison to clinical evaluation combined with electrodiagnosis as reference standard. Methods: 23 consecutive patients with carpal tunnel syndrome symptoms (46 wrists-35 with nerve conduction study confirmed CTS, 11 without CTS) underwent neurosonologic evaluation with high resolution ultrasound including median nerve cross sectional area(CSA) at carpal tunnel inlet, flattening ratio, Wrist/forearm CSA ratio measurements. Patient reported measures were recorded using Boston carpal tunnel syndrome questionnaire (BCTQ). Results: Statistically significant correlation was found between median nerve CSA at carpal tunnel inlet and disease severity assessed by electrodiagnosis (r=0.545, p value-0.002), hand function status had significant correlation with electrodiagnostic severity class (r=0.422, p value 0.012). Flattening ratio, Wrist/forearm CSA ratio did not show significant correlation with clinical and electrophysiology measures. Sensitivity and specificity for a cross sectional area cut off of 9 cm2 for diagnosis of CTS was found to be 85.7 percent and 64 percent respectively. Conclusion: Median nerve cross sectional area CSA measurement is the most useful neurosonologic parameter and correlates with electrodiagnostic severity. Ultrasound is a useful complementary tool for CTS diagnosis, assessment alongside electrodiagnosis.
Keywords: Carpal Tunnel Syndrome, Neurosonology, Compression neuropathy
Carpal tunnel syndrome (CTS) is the most commonly encountered compression neuropathy in clinical practice. Diagnosis depends on clinical signs and symptoms essentially, however these in isolation lack sufficient diagnostic accuracy. Electrodiagnostic studies are used most commonly to confirm the clinical suspicion of carpal tunnel syndrome, determining the severity of the condition and planning treatment.
However nerve conduction studies can be uncomfortable to the patient, time consuming and costly .This necessitates the utilisation of alternative diagnostic modalities.
Cardinal among these alternative diagnostic modalities are ultrasonography and magnetic resonance imaging. Magnetic resonance imaging provides soft tissue images with excellent resolution helping visualise nerve pathology in detail. However, ultrasonography is more advantageous on account of its lower cost, shorter examination time and easy availability.
Sonography aids in direct visualisation of the nerve pathology, rule out secondary causes such as nerve tumors or tenosynovitis and identify variants such as bifid median nerve.
Both electrodiagnostic studies and sonography provide complementary data regarding the neuropathology of compression neuropathies[1]. A multi-modality approach combining meticulous history and clinical evaluation with electrodiagnosis and ultrasonography improves diagnostic accuracy alongside proper planning of treatment and follow up of patients.
We aimed to study the relationship of median nerve ultrasound findings with patient reported symptoms, hand function and electrodiagnostic severity. We also intended to compare the diagnostic value of ultrasound compared to clinical evaluation combined with electrophysiology as a reference standard
Consecutive patients presenting to the Neurology out patient service at our institution with history suggestive of carpal tunnel syndrome were recruited for the study. Patients were excluded if they gave previous history of hand surgery or trauma. Approval of the institutional ethics committee was obtained and only those who gave written informed consent were included.
Detailed history with emphasis on predisposing factors for development of CTS was collected from all subjects. Motor and sensory examination to look for objective findings in the median nerve distribution along with provocative maneuvers including Tinels and Phalens signs were elicited.
The Boston carpal tunnel syndrome questionnaire, which is a self administered questionnaire was utilised for collection of patient oriented data. The Boston questionnaire[2] has two separate parts-11 questions assessing the symptom severity and 8 questions are for assessment of the functional status of the hand. For each of the questions a score from 0- 5 is given and mean scores are calculated separately for determining the symptom severity and functional status.
Standard median nerve electrodiagnostic evaluation was performed using Nicolet Viking Quest EMG machine. Parameters studied included the median nerve motor distal latency, conduction velocity in the wrist-palm segment, compound muscle action potential (CMAP), F-wave latency, sensory nerve action potential (SNAP) amplitude and median sensory latency.
Internal comparison studies comparing motor latencies of the median and ulnar nerves were performed for diagnosis of mild cases.
Normal limits for the electrodiagnostic values were set as follows on the basis of normative data Median nerve motor distal latency <3.8 milliseconds Median compound muscle action potential amplitude >5.0 millivolt Median motor conduction velocity in wrist-palm segment >50 meter/second Median nerve sensory distal latency <3.5 milliseconds Median sensory nerve action potential amplitude- >10 millivolt
Median, ulnar motor latency difference of >0.4millisecond in the 3rd digit was set as the parameter for diagnosis of mild CTS by internal comparison study As part of the initial screening, 40 patients were selected, 5 were excluded on account of history of previous hand surgery, 4 did not give consent and 8 patients were excluded as they did not satisfy the electrodiagnostic criteria. Finally, 23 patients who were selected after satisfying the nerve conduction criteria underwent clinical and ultrasonographic evaluation. 12 cases had bilateral CTS, 11 were unilateral. Hence, total 46 wrists were included, 35 with electrodiagnostic confirmation of CTS and 11 without.
Based on the electrodiagnostic findings disease severity was graded as mild, moderate and severe categories following the scheme in a previous study by Padua et al[3]
High resolution nerve ultrasound of the median nerve was performed with a real-time scanner with a 12- 4MHz linear array transducer- PHILIPS CLEARVUE 650 MEDICAL SYSTEM Transverse imaging of the median nerve was performed at the carpal tunnel inlet, and distal 1/3rd of the forearm. Also longitudinal view was utilised to confirm the correct identification of the median nerve.
The sonographic parameters assessed were
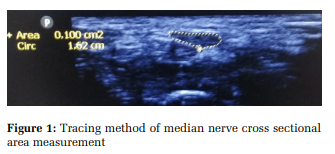
Calculation of the nerve cross-sectional area (CSA) was done at the carpal tunnel inlet (level of proximal end of flexor retinaculum), where the median nerve appeared maximally enlarged.
The circumference of the median nerve and its CSA were measured using a continuous boundary trace of the nerve including the surrounding echogenic rim (Figure 1).
Median nerve cross-sectional area values were obtained using the software of the device . The diagnostic accuracy of this direct method of area calculation has been found to be better compared to the indirect approach[4] .
Cross sectional area was also recorded in the distal forearm for calculating the ratio between the wrist and forearm cross sectional areas.
Ratio between the major and minor axis measurements of the median nerve was calculated to determine the flattening ratio (FR)
Total 23 patients with carpal tunnel syndrome confirmed by electrodiagnosis were included in the study. Of this, 12 cases were bilateral and 11
unilateral. The clinical assessment scores, sonography measurements and electrodiagnostic data was collected considering each wrist as a unique sample as in previous studies with a similar design.[5,6] .
Hence, total 46 wrists were included, 35 with confirmed CTS and 11 without CTS.
47.7 years was the mean age of participants included in the study. Majority of the cases were females (73.91%).Most had duration of symptoms less than 1 year, the most common symptoms reported were numbness paresthesiae involving the lateral three fingers followed by distal hand and forearm pain.
The mean symptom severity score and functional status scores obtained by the Boston questionnaire were 1.9(range 1.0-3.23; SD: 0.51) and 1.66(range 1.0- 3.25;SD:0.61) respectively in the wrists with CTS.
The mean median nerve cross-sectional area (CSA) among the CTS wrists was found to be 12.5 (range12.4-20.4; SD: 3.15) and 9.3(range7.7-12.2;SD:1.56) in wrists without CTS.
The mean flattening ratio and wrist/forearm CSA ratio were found to be 3.03(range 1.15-4.6; SD:1.07)and 1.61(range 1.06-2.23;SD:0.29) in the CTS group.
Among the 35 CTS wrists, 9(25.7%) belonged to the mild category,18(51.4%) moderate and 8(22.9%) severe category as per electrodiagnostic severity. Statistical analysis was performed using IBM SPSS software package version 24. The sonographic data was correlated with patient reported clinical data and electrodiagnostic severity class.
The non-parametric analysis of the correlation was assessed by Spearman’s R test and the comparison of the various electrodiagnostic severity groups was assessed by the Kruskall Wallis test. Significance was set at 0.05.
Among the sonographic measurements, the median nerve cross-sectional are at the proximal carpal tunnel was found have significant correlation with electrodiagnostic severity using the Spearmans correlation coefficient(r=0.545,p value-0.002).
The flattening ratio and wrist/forearm CSA ratio measurements were not found to have significant correlation with the electrophysiologic severity (r=0.197,p vaue-0.256 and r=0.252,p value-0.145).
Patient reported symptoms as guaged by the Boston questionnaire functional status and symptom severity scores did not show statistically significant correlation with the sonographic data. Significant correlation was found between the hand functional status score and the electrodiagnostic severity.
(Spearmans rho r=0.422, p value 0.012). However significant correlation of electrodiagnostic severity with symptom severity score was not found.
Kruskall- wallis test showed statistically significant difference in the median nerve cross-sectional area values between the various electrodiagnostic severity categories. (p value 0.004).However, the flattening ratio and wrist/forearm CSA ratio measurements did not show statistically significant difference between the groups.
Area under the curve value for the ROC analysis of median nerve cross-sectional area measurement was 0.799 which almost equals 0.8 which is the cut off for a good test by ROC analysis.
For a cross-sectional area cut off of 9 cm2 -85.7 percent was the sensitivity and 64 percent was the specificity respectively.
When the cut off was set as 10 cm2 , sensitivity and specificity were determined to be- 74 percent and 73 percent respectively.
The present study attempts to emphasis a multimodality approach towards the evaluation of patients with carpal tunnel syndrome incorporating ultrasonographic evaluation along with clinical data and electrodiagnosis. We attempted to study the relationship between patient reported clinical data, sonographic parameters and electrodiagnostic data.
The sonographic technique employed is easy to perform and easily reproducible as we have used single measurement of the median nerve crosssectional area at the carpal tunnel inlet.
Wong et al[5] took median nerve cross-sectional area measurements at three different points of the carpal tunnel. Using a classification and regression tree, they determined optimal threshold values for each of these levels.
Compared to this approach, the simplified protocol we have used is more feasible in routine settings where there are time constraints. In addition to the median nerve CSA, we recorded the flattening ratio and wrist forearm cross-sectional area ratio . These parameters have been studied and found previously to improve diagnostic accuracy of neurosonologic assessment.[7]
Most previous studies on neurosonologic findings in CTS had a case-control design[8–13] A disadvantage of this design is that while selecting cases and controls , patients with borderline or mild expression of the disease are frequently omitted, potentially resulting in unusually high diagnostic accuracy compared to the actual real life scenario.
Wong et al[5] and Ziswiler et al[6] have studied neurosonologic findings in consecutive patients with carpal tunnel syndrome similar to the pattern followed in the present study. They compared the diagnostic accuracy of sonographic evaluation in comparison to clinical evaluation and electrodiagnostic studies. We found statistically significant correlation between the median nerve CSA measurement and the severity of CTS determined by electrodiagnosis.
Previous studies have documented that the nerve swelling in compression neuropathies is secondary to intraneural edema[14] There is correlation between the neural edema and neuropathology leading to axonal loss as has been shown previously.[15] Given this premise, it is plausible that the crosssectional area increases according to the increasing electrodiagnostic severity.
Patient reported symptoms and the hand function assessed by the Boston questionnaire were found to have positive correlation with the CSA measurements. However, these were not found to reach the levels required for statistical significance. At the same time, the hand functional status score was found to have statistically significant correlation with the electrodiagnostic severity.
Previous studies addressing the correlation of nerve ultrasound with clinical and electrodiagnostic results have had varying results according to the type of patients recruited and variable study design. Lee et al and Kaymak et al[16,17] found that neither symptom severity score(SSS) nor functional status score (FSS)correlated with the CSA of the median nerve. El Miedany and colleagues found that both these scores were related to ultrasound parameters [13] .
Padua et al[18] attempted to correlate patient reported symptoms, clinical disease severity assessed by a validated scale (Hi-ob scale) with median nerve cross-sectional area measurement and the electrodiagnostic severity class. The clinical disease severity correlated linearly with the sonographic findings.The patient reported symptoms did not worsen with the increase of CSA; however, the hand function strongly related to CSA.
These varied findings in literature could be due to varied study designs, inclusion of patients with differing spectrums of disease severity and different sonographic techniques employed in these studies. The measurements of flattening ratio and wrist/forearm ratio of median CSA were found not to have significant correlation either with the clinical data or the sonographic findings in the present study.
Various cut off values for the median CSA have been suggested in literature. A common cut-off value for a diagnosis of CTS suggested is 10 mm.[19] However cut off values of have been reported to vary between 9.0 and 15.0mm2[6] .
Our results of sensitivity and specificity are within the range previously reported in literature. Median CSA was the most useful sonographic parameter, flattening ratio was variable and found not to be correlating with disease severity. Similar findings have previously been reported in literature.[20] Depending on the setting and the purpose, different cut off values of median nerve cross sectional area measurements may be used as suggested by Ziswiler et al.[6]
The major limitation of the study is the relatively small sample size, besides the proportion of patients with severe disease is relatively higher as data is obtained from a tertiary care setting.
Median nerve cross-sectional area (CSA) measurement is the most useful sonographic parameter for diagnosis and correlates with electrodiagnostic severity. Flattening ratio, wrist/forearm ratio are variable and do not correlate with disease severity, patient reported symptoms.
Multi-modality approach incorporating neurosonology along with clinical evaluation and nerve conduction studies is relevant for CTS diagnosis and work up.
Subscribe now for latest articles and news.