Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.2021.v07i03.005
Year: 2021, Volume: 7, Issue: 3, Pages: 13-18
Original Article
Vibhuti Goyal1 , Ranjan Agrawal1 , Nitesh Mohan1
1Department of Pathology, Rohilkhand Medical College and Hospital, Bareilly, UP, India
Address for correspondence:
Vibhuti Goyal, Department of Pathology, Rohilkhand Medical College and Hospital, Bareilly, UP, India. E-mail: [email protected]
Background : Leiomyomas are the most common benign mesenchymal tumor of uterus in women of reproductive age group. They may have unusual presentations in the form of location or undergo various degenerative changes posing great diagnostic difficulties. Aim : To identify the various secondary degenerative changes and histopathological variants of uterine leiomyoma along with review of literature. Material and methods : The study included a total of 150 cases of leiomyomas diagnosed in the department of pathology for a period of 1year. Detailed gross and microscopic examination was carried out and the data recorded. Results: Out of total 150 cases of leiomyoma, intramural was the most common (66.7%) location. Age of the patients ranged from 18-60 years with peak incidence in 41-50 years (43.3%). Secondary changes were observed in 44(29.3%) cases. Out of which hyaline degeneration was the most common type of degeneration and observed in 56.8% cases. Other secondary changes observed were myxoid degeneration, calcific degeneration, hydropic degeneration and hemorrhagic infarction. Only 2 cases of cellular leiomyoma were identified as histological variant. Conclusion : Leiomyomas of female genital tract are common benign tumors. Degenerative changes are more common in intramural leiomyomas. Secondary changes and histological variants may pose diagnostic difficulties. A complete gross and histological examination is mandatory to rule out malignant transformation.
Keywords: Uterine leiomyoma, degeneration, variants
Leiomyoma is a benign tumor of smooth muscle. Uterine leiomyomas are the most common benign tumor that arises from the myometrium of female genital tract. Uterine leiomyomas are also termed as fibroids or myomas. The estimated incidence of uterine leiomyoma is 5-20% in women of reproductive age group.[1] Uterine leiomyomas are incidental or accidental finding in approximately 70- 80% of hysterectomy specimens.
The exact etiology of uterine leiomyoma is not known. Hormonal disturbances and genetic alterations are postulated to have some role in the development of uterine leiomyoma. Molecular studies have shown that uterine leiomyomas have more number of estrogen receptors than the normal myometrium.[2] They rarely occur before menarche and usually regress after menopause. Patient with uterine leiomyoma may have an increased risk of developing breast cancer as both share some of the risk factors such as obesity and estrogen exposure.[3]
Clinically uterine leiomyomas are usually asymptomatic. [3] However, few patients present with menorrhagia, lower abdominal pain, dysmenorrhoea, abdominal mass, urinary frequency and/or urgency, infertility and recurrent abortions. Myomas in pregnant women increase the frequency of spontaneous abortion, fetal malpresentation, uterine inertia and post-partum hemorrhage. These clinical features mainly depend on the size and location of leiomyomas.[4] As per the location leiomyomas are classified as intramural, subserosal and submucosal types.
Uterine leiomyomas may undergo various secondary degenerative changes such as hyaline, myxoid, cystic, fatty or red degeneration and dystrophic calcification. Hyaline degeneration is the most common secondary degenerative change while malignant transformation to leiomyosarcoma, if it occurs at all, is extremely rare.[5]
Histological variants of leiomyoma are cellular leiomyoma, atypical leiomyoma, and epithelioid leiomyoma. Some of these variants exhibit diagnostic difficulty then it becomes problematic to differentiate them from low grade leiomyosarcoma.
In the present study we have made an attempt to know the prevalence and identify the various secondary degenerative changes and histological variants that encountered in leiomyoma in a tertiary care set-up along with review of literature.
A prospective and observational study was conducted over a period of 1 year from January 2020 to December 2020 in the department of pathology at Rohilkhand Medical College and Hospital, Bareilly. The institutional ethical committee clearance was taken.
Inclusion criteria – All the surgically excised hysterectomy specimens of any age group in which fibroid was clinically and radiologically suspected are included in the present study. All the cases in which fibroid was found as an incidental finding along with other lesions and all myomectomy specimens were also included in the study.
Exclusion criteria – Hysterectomy specimens in which fibroid was not observed either on gross or on microscopy were excluded out.
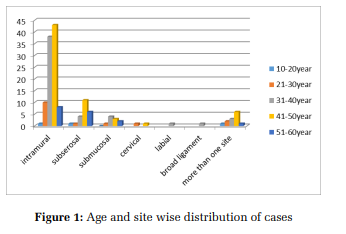
The patient’s demographic data, clinical history and type of surgical procedure were recorded. The surgical specimens were first fixed in 10% buffered formalin for at least 24 hours after slicing them. Detailed gross examination was noted including size, location, number and secondary changes in leiomyoma. Representative tissue sections were taken including the leiomyoma and other associated pathologies. If leiomyomas were multiple in no. then tissue sections were taken from each leiomyoma. Sections were processed using automated tissue processor and embedded in paraffin wax. 3-5 µm thick sections were cut and stained with HemaSingle leiomyoma was observed in 90(60.0%) cases while multiple (2-10) leiomyomas were found in the remaining 60(40.0%) cases. Intramural leiomyoma was the most common site accounting for 100(66.7%) cases followed by subserosal in 23(15.3%) cases and submucosal in 9(6.0%) cases. In 2(1. 33%) cases, leiomyoma was present in the cervix. One case each of leiomyoma in the labia majora, broad ligament and ovary were also found. In 13(8.67%) cases leiomyomas were present in more than one location in the uterus. (Figure 1)
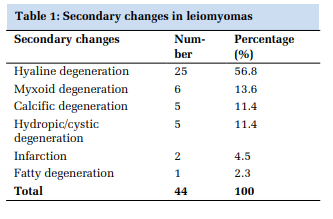
Secondary changes were observed only in 44(29.3%) cases of all leiomyomas. Most of the changes were present in intramural leiomyomas. Hyaline degeneration was the most common observation and found in 25(56.8%) of these cases. Other secondary changes included myxoid degeneration in 6(13.6%), calcific degeneration in 5(11.4%), hydropic or cystic degeneration in 5(11.4%), infarction in 2(4.5%), and fatty degeneration in 1(2.3%) case. Among the variants of leiomyoma, only 2(1.3%) cases of cellular leiomyomas were observed with increased cellularity, closely packed spindle cells some of which showed overlapping, scant mitotic figure and absence of necrosis. (Table 1)
The most common uterine pathology associated with leiomyomas was adenomyosis and was observed in 20(13.3%) cases. Intramural leiomyoma was also found as an additional finding in 2(1.3%) cases of squamous cell carcinoma cervix.
Uterine leiomyomas are the most common benign neoplasm which arises from the smooth muscles of the myometrium. Hysterectomy is the most common gynecological surgery and leiomyomas are found to be the most common clinical finding accounting for about 80% of all hysterectomy specimens. Other common causes of hysterectomy include adenomyosis, prolapse uterus, dysfunctional uterine bleeding and rarely malignancy.[6]
In the present study the most common hysterectomy procedure was total hysterectomy observed in 82 (54.7%) cases, as compared to other studies in which total hysterectomy with bilateral salpingooopherectomy was the most common (66.07%) procedure.[7] This is in discordance with the observations reported in other studies. The possible reason may be to reduce the risk of osteoporosis and cardiovascular diseases.
Since leiomyomas are estrogen dependent, they are more commonly observed in the reproductive age group. The usual age of distribution may range from menarche to menopause.[8] In the present study the age of the patients ranged from 18-60 years. The mean age was 44 years and the youngest patient was 18 years old. Maximum incidence, 65(43. 3%) cases were in the 41-50 years age group. These findings were similar to other studies who also observed that uterine fibroids were more common in the third and fourth decades of life and the youngest patient reported was that of 18 years.[9,10]
The most common symptom in our study was abnormal uterine bleeding. Few presented with lower abdominal pain and dysmenorrhea, correlating with the findings of other studies.[10,11] The cause of abnormal uterine bleeding in fibroids may be due to increased vascularity, enlargement of the endometrial surface and altered uterine contractility.[12] These causes are assumed to be due to being oestrogen dependent.
Leiomyomas can be single or multiple and may be of variable size. In our study 90(60%) cases had single leiomyoma and 60(40%) cases had multiple leiomyomas similar to the study done by Gowri M et al[11] who found 71% single leiomyomas in hysterectomy specimens while in contrast to other studies who had majority of multiple leiomyomas.[13] Uterine leiomyomas are classified according to the location into intramural, submucosal and subserosal types. Majority of the leiomyomas in our study were intramural 100(66.6%) followed by subserosal 23(15.3%) and submucosal 09(6.0%). These findings were similar with other studies by Gowri et al[11] and Abraham J et al.[14] Uterine leiomyomas can be found in more than one location in the same hysterectomy specimen. 13 cases (8.67%) had leiomyoma in more than one location, mainly comprising of intramural and subserosal types.
Leiomyomas can be found in extrauterine locations as well. They usually arise in the genitourinary tract as in the cervix, vulva, ovaries, broad ligament, urethra and urinary bladder but may also arise in any other site e.g. blood vessels, skin etc. Extrauterine leiomyomas are very rare. In our study we encountered 02(1.33%) cases of cervical fibroid, 01(0.66%) case of broad ligament fibroid, 01(0.66%) case of vulval leiomyoma and 01(0.66%) case of ovarian fibroid. The broad ligament leiomyoma, the most common extrauterine site and also known as parasitic leiomyoma, had a very low incidence rate.[15] Cervical fibroids are usually single in number and are similar to uterine fibroids. In another study done by Ibrar et al[8] found incidence of cervical leiomyoma as 3.0%. Leiomyoma of vulva are also very rare and clinically mimic with bartholin cyst. Leiomyoma of ovary are rarest and usually unilateral and small and discovered incidentally. Some extrauterine leiomyomas may mimic malignancy and present with diagnostic challenge.[16] Grossly, leiomyomas are usually round and well circumscribed with a whorled cut surface and are well demarcated from the adjacent myometrium. Microscopically they are composed of spindle cells with elongated nucleus and arranged in fascicles and whorls. Mitotic activity is usually less than 5 mitoses per 10 high power fields and no atypical forms are found.
Several secondary degenerative changes have been identified in leiomyomas. In the present study secondary degenerative changes were observed in 44(29.3%) cases similar to that reported in other studies who also found secondary changes in 22.6% cases.[11] Nggada et al[4] also observed secondary changes in 21% cases of all leiomyomas. The cause of degenerative changes in leiomyomas is inadequate blood supply and is usually observed in large and long standing leiomyomas especially so in intramural leiomyomas. This may result most commonly in hyalinization, most common, followed by cystic, myxoid, infarction, fatty change, calcification and rarely malignant changes. The type of secondary change depends on the degree and rapidity of vascular insufficiency.
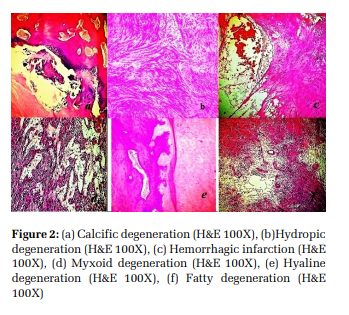
In our study hyaline degeneration was the most common secondary change and found in 25(56.8%) cases similar to the studies by Begum et al[13] and Dayal et al[10] . Myxoid degeneration was the next common finding and found in 6(13.6%) cases. Histologically it shows separation of benign smooth muscles with myxoid material and sometimes poses diagnostic difficulty with myxoid leiomyosarcomas. To differentiate we should look for margins of tumor, cytological atypia and mitosis. Hydropic or cystic change, caused due to accumulation of oedematous fluid, was observed in 5(11.3%) cases comparable to the study of Abraham et al[14] . (Figure 2)
In one case we also found scattered fat cells in a typical leiomyoma. The incidence of leiomyoma with fatty degeneration is very rare with incidence varies from 0.03 – 2.0%.[17] Histologically mature adipose tissue is found in varying amounts in leiomyomas. The differential diagnoses include spindle cell lipoma and atypical lipoma. Leiomyoma with infarction is also very rare and usually associated with pregnancy and is an acute clinical condition. In our study we found 2(4.5%) cases of leiomyoma with infarction. Grossly tumor shows dark red areas and histologically there were large areas of hemorrhagic infarction mixed with benign smooth muscle cells (Figure 2). One case was also showing multiple degenerative changes as hyaline degeneration, calcification and infarction in single leiomyoma. These changes are usually seen in long standing leiomyomas. These changes are also reported in women taking oral contraceptives.[18]
In our study we also found 2(1.3%) cases of cellular leiomyoma. Grossly it was similar to the classical leiomyoma. Histologically it showed fascicular growth pattern with increased cellularity.
However, areas of necrosis and atypical mitosis were absent. Mitotic count was low (<5/HPF). (Figure 3) The differential diagnosis includes leiomyosarcoma and endometrial stromal tumor. These can be differentiated on the basis of cytological atypia and necrosis. Additional immunohistochemical markers as ER, PR and Desmin can also be applied to differentiate.[19]
Uterine leiomyomas are the most common benign tumor of female genital tract. Although symptoms depend on size and location of leiomyoma, various symptoms are associated with certain degenerative changes which can be life threatening. Now a day, these conditions are being more common in young female, so a detailed study can be helpful for the clinicians also to assess early complications and manage accordingly. Although leiomyomas are benign, they are associated with significant morbidity in women of reproductive age group. Early diagnosis and introduction of new minimally invasive management of fibroids can avoid hysterectomy in young patients who wish to preserve their fertility. Secondary degenerative changes and variation in morphology can also present as diagnostic challenge. A detailed gross examination and specific histopathological features along with immunohistochemistry is mandatory to distinguish from benign to malignant.
Studies have been conducted on leiomyoma and secondary changes but in Rohilkhand region it is the first study to be conducted.
Dr. Praveen Garg, Associate Professor, Department of Orthopedics, for helping in literature search and manuscript preparation

Subscribe now for latest articles and news.