Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.v9i1.22.374
Year: 2023, Volume: 9, Issue: 1, Pages: 118-120
Case Report
Teleflo Boopathy1 , S Kanimozhi2 , V Ramya2 , P Lakshmi Piriya3
1Associate Professor, Department of Pathology, Government Kilpauk Medical College, Chennai, India
2Assistant Professor, Department of Pathology, Government Kilpauk Medical College, Chennai, India
3Postgraduate, Department of Pathology, Government Kilpauk Medical College, Chennai, India
Address for correspondence:
P Lakshmi Piriya, Postgraduate, Department of Pathology, Government Kilpauk Medical College, Chennai, India.
E-mail: [email protected]
Received Date:22 August 2022, Accepted Date:06 January 2023, Published Date:15 May 2023
Diabetic mastopathy is an uncommon fibrous tissue lesion of the breast which is usually seen in patients with longstanding type 1 diabetes mellitus. We report a case of diabetic mastopathy in an insulin dependent type 2 diabetes mellitus patient. 47-year-old postmenopausal woman, presented with two lumps, one firm mobile mass and another, a firm-hard mass in the upper inner quadrant of the left breast. Mammography and ultrasonography came out to be BIRADS III lesion. Fine-needle aspiration cytology [FNAC] was performed showing features of fibroadenoma with fibrocystic change. Histopathological examination and Immunohistochemistry studies revealed it to be fibroadenoma along with lymphocytic mastopathy.
Keywords: Fibroadenoma, Lymphocytic mastitis, Mimicker, Diabetes
Lymphocytic mastopathy, a rare benign breast disease, is commonly associated with long-standing diabetes, hence also named Diabetic mastopathy or sclerosing lobular mastopathy. This is usually seen in young to middle-aged women(34-47years). It constitutes less than 1% of benign breast entities. 1 The condition is also seen associated with other autoimmune disorders. Though commonly seen in Insulin Dependent Type I diabetes mellitus, some cases have been reported in insulin dependent type II diabetes mellitus patients also. 2 Clinically presents as a palpable mass, mimicking malignancy. Misinterpretation can lead to mastectomies causing distress to the patient. Imaging features are non-specific; hence core needle biopsy or excision is done. 3 Here we report a case of a 47-year woman with two lumps in left breast, one clinically mimicking malignancy. Histopathological examination and IHC studies revealed it to be fibroadenoma along with lymphocytic mastopathy.
A 47-year-old female came to the surgical outpatient department with complaints of palpable mass in her left breast for one year. The swelling was initially small and later progressed to the current size. She is a known case of Type II Diabetes Mellitus and is on Insulin treatment for 9 years. Her past history does not include any other disease. She attained menarche at 14 years, with regular menstrual cycles. Parity - P2L2, her last child birth was 23 years back. She attained menopause at the age of 46.
On physical examination, left breast reveals two ill-defined masses of size 4cmx3cm in upper inner quadrant, hard in consistency, moves along with breast tissue and another lump measuring 3x2cm in upper inner quadrant, firm in consistency. Right breast examination shows no abnormality. Lymph nodes not palpable in both axillae.
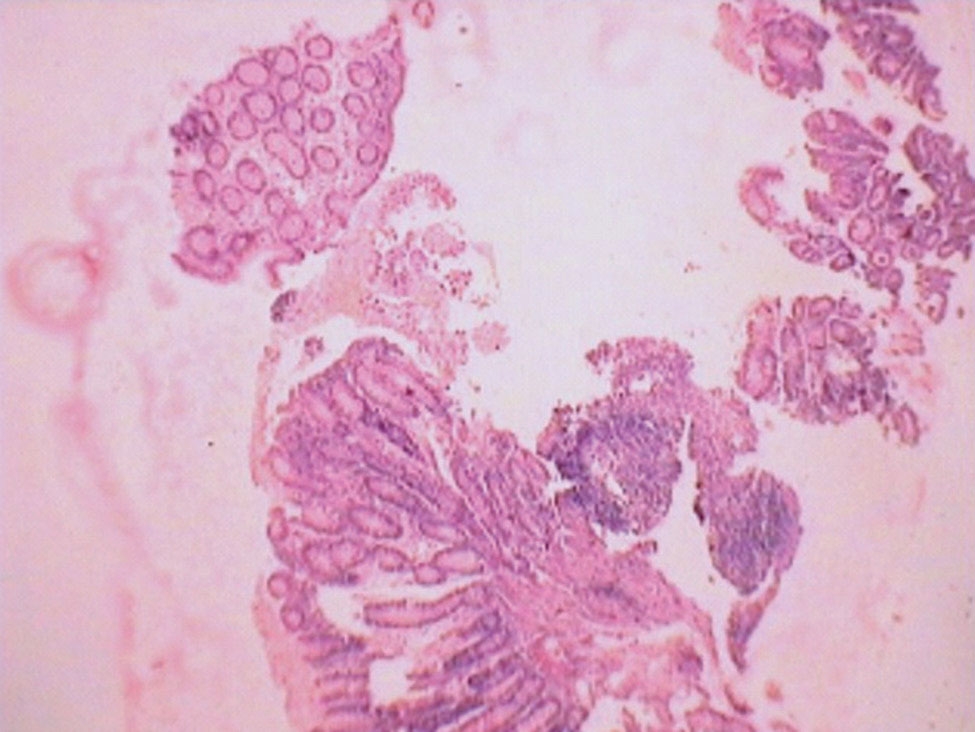
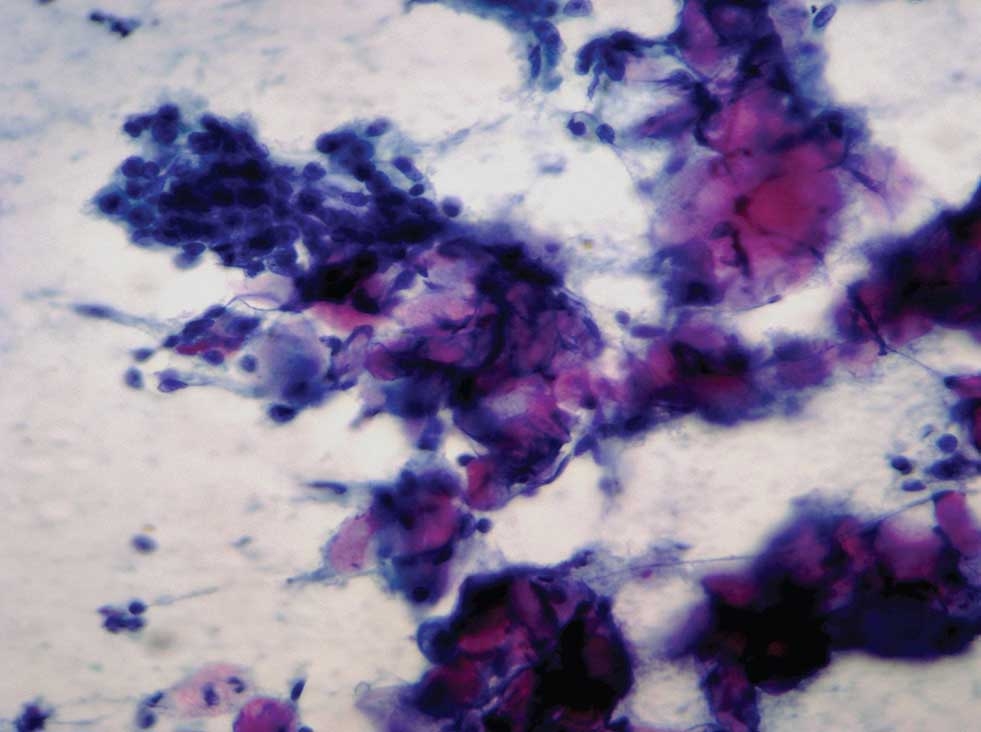
The patient’s haematological investigations were within normal limits. Ultrasonogram was suggestive of BIRADS III. Fine needle aspiration was done which came out to be fibroadenoma with fibrocystic change. Patient was admitted in surgical ward and wide local excision was done. Grossly, the lesions were of sizeFigure 1]

Histopathological examination revealed breast parenchyma composed of benign ducts exhibiting pericanalicular and intracanalicular pattern lined by bilayered epithelium surrounded by fibromyxoid stroma suggesting features of fibroadenoma. The larger lesion with grey white areas showed dense sheets of lymphocytes along with periductal and perivascular infiltration of lymphocytes in a dense collagenous fibrous stroma which suggests features of lymphocytic mastitis. [Figure 2] Immunohistochemical analysis was done, which showed, CD20 positive in 60% of lymphocytes and SMA positive in spindle shaped stromal cells. [Figure 3, Figure 4] CD 3 – focal positive in 15% of lymphocytes. Thus, confirming the diagnosis of fibroadenoma along with lymphocytic mastitis.



Lymphocytic mastitis is an uncommon fibroinflammatory benign breast lesion. This lesion mimics malignancy both clinically and radiologically, and constitutes less than 1% of all breast lesions. 4 The lesion appears either as single or multiple ill-defined hard mass, painful or painless, unilateral or bilateral.
Lymphocytic mastitis is characterised histologically by dense, keloid-like parenchymal fibrosis with epithelioid fibroblasts and lymphocytic infiltrates, in perivascular, periductal and perilobular areas, predominantly being small lymphocytes and few scattered plasma cells. 5 These lymphocytes are predominantly B cells, can be detected using immunohistochemical analysis.
Pathogenesis is unclear, yet thought to be multifactorial. Association with type I diabetes and insulin dependent type II diabetes suggests that hyperglycaemia can be one of the factors involved. Autoimmune disorders like Sjogren’s syndrome, Hashimoto’s thyroiditis can also be seen associated commonly with lymphocytic mastitis. 6
Ultrasonography and mammographic assessment of these lesions have been challenging because of its features such as microcalcifications, posterior acoustic shadow etc., mimics malignant features. MRI is superior to these and can detect the nature of lesion to be benign. 7, 8 Fine needle aspiration sample, is usually hypocellular, making the diagnosis even more challenging. Hence image guided core needle biopsy will be required. Even though core biopsy can be sufficient to a conclusive diagnosis of lymphocytic mastitis, the presence of a suspicious lesion in postmenopausal age women warrants excision. And also, the lesion has a tendency to recur. According to Camuto et al, about 60% cases have tendency to recur with more breast tissue involvement, which suggests the multicentric effect of diabetes on breast tissue. 9
This case, fibroadenoma with lymphocytic mastitis is reported for its rare presentation, in a postmenopausal, insulin dependent diabetic patient. However, this combination of fibroadenoma and lymphocytic mastitis could not be found in literature search. Clinically, the suspicious lesion mimicked to be malignancy and being a postmenopausal woman, wide local excision was done. Lymphocytic mastopathy has to be considered as a differential in a patient with long standing diabetes or other autoimmune diabetes. 10 It poses diagnostic difficulties as it presents as hard mass clinically resembling malignancy. Hence the usage of clinical, imaging, histopathological and immunohistochemical analysis is important to differentiate it from malignancy, thereby aiding in deciding the management for the patient and preventing radical surgeries.
Subscribe now for latest articles and news.