Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.2020.v06i02.005
Year: 2020, Volume: 6, Issue: 2, Pages: 25-30
Original Article
K M Kibballi Madhukeshwar Adarsh1, Prakash Aswathi2, H Pavithra3, Hassan Hadi4, Sunny Jomon5, Rasheed Abdul Valiyapalathingal4
1Assistant Professor, Department of Radiodiagnosis, Yenepoya Medical College, Mangalore, Karnataka, India,
2Consultant Radiologist, Department of Radiodiagnosis, Dr. Gopinath’s Diagnostic Centre, Thiruvananthapuram, Kerala, India,
3Tutor, Department of Community Medicine, Yenepoya Medical College, Mangalore, Karnataka, India,
4Senior Resident, Department of Radiodiagnosis, Yenepoya Medical College, Mangalore, Karnataka, India,
5Senior Resident, Department of Radiodiagnosis, Kerala Institute of Medical Sciences, Thiruvananthapuram, Kerala, India
Address for correspondence:
Dr. Kibballi Madhukeshwar Adarsh, 5C, Kambla Heights, Kadri Kambala Road Dakshina Kannada, Mangaluru - 575 004, Karnataka, India. Mobile: +91-9483469838. E-mail: [email protected]
Introduction: Estimation of fetal weight is necessary for planning and managing labor. At term, macrosomia can be predicted by the estimation of fetal soft tissue and can be done by various ultrasonographic measurements. The correlation of estimated fetal weight (EFW) using fetal soft-tissue thickness with actual birth weight was seen in this study.
Materials and Methods: Seventy ladies with singleton pregnancies were enrolled. The fetal weight was categorized into two groups, above and below 90th percentile respective of the gestational age. Fetal weight estimation was done using Hadlock’s method, mid-thigh soft-tissue thickness (MTSTT) and was correlated with actual birth weight. Fetal abdominal subcutaneous tissue thickness (FASTT) was correlated with actual birth weight as well.
Results:Moderate positive correlation was found between the EFW using MTSTT and Hadlock’s method, and it was statistically significant (P < 0.001). FASTT had a mild positive correlation, which was not statistically significant. Further, MTSTT was found to be more sensitive and specific in the estimation of fetal weight with actual birth weight as a gold standard.
Conclusion: Estimation of fetal weight using MTSTT was more superior to Hadlock’s method with higher sensitivity and specificity values. There was no significant correlation observed between FASTT value and actual birth weight.
KEY WORDS:Estimation of fetal weight, Fetal abdominal subcutaneous tissue thickness, Hadlock’s method, mid-thigh soft-tissue thickness.
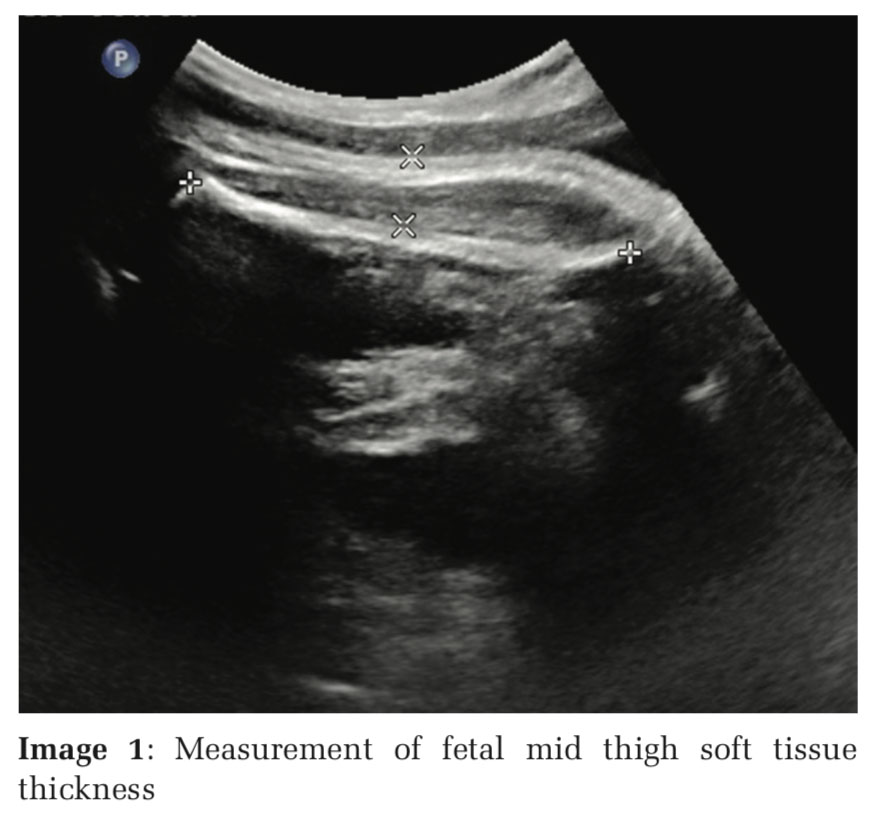
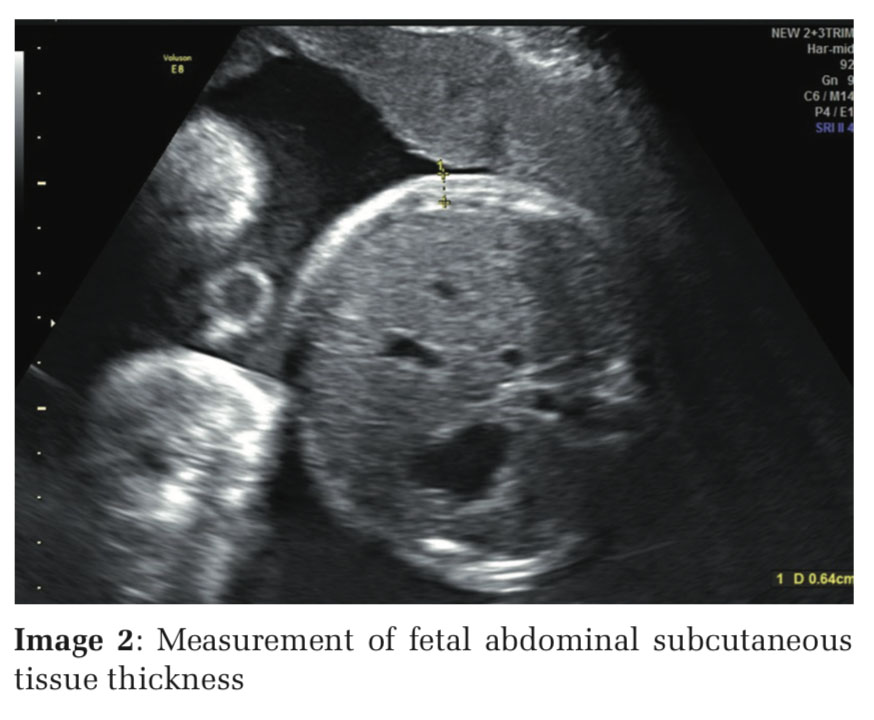
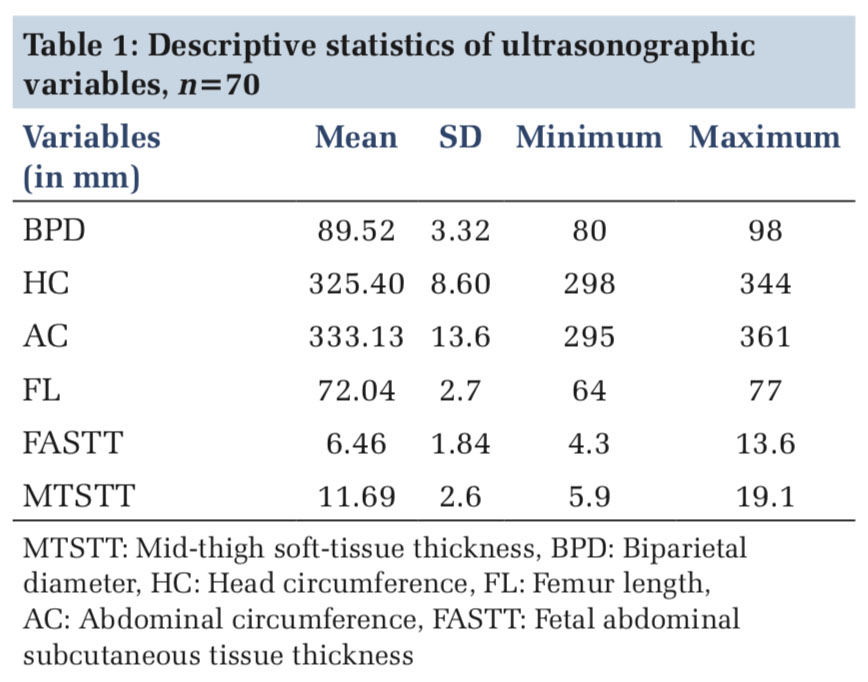
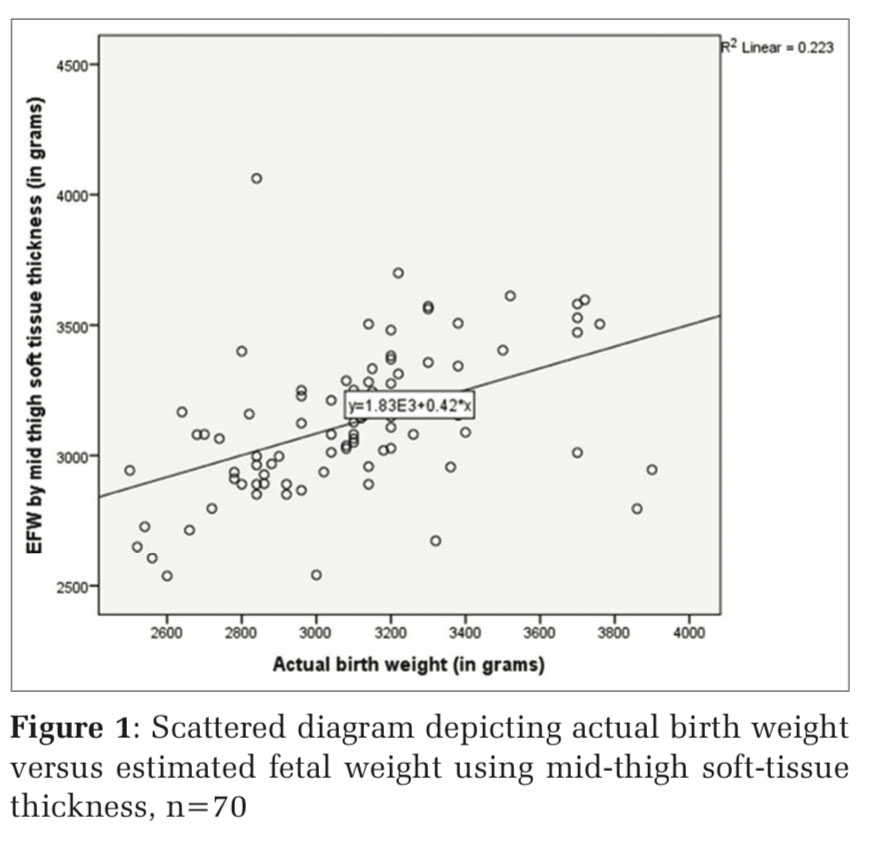
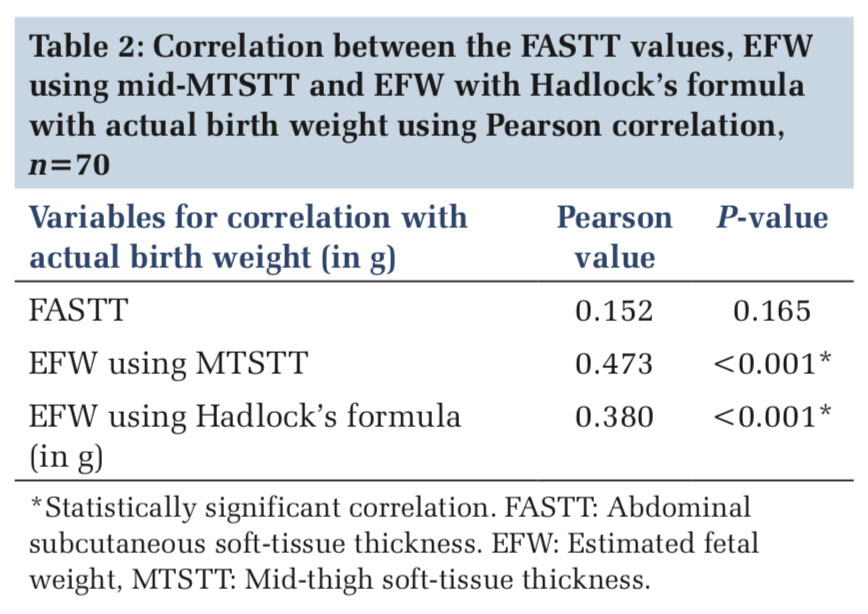
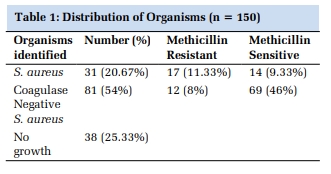
IntroductionUltrasonography (USG) is commonly used to assess fetal growth and further to estimate fetal weight. Estimated fetal weight (EFW) gives valuable information for planning and managing labor. This estimation is done using various formulae, the majority of them introduced in the 1980s. Various standardized fetal parameters such as biparietal diameter (BPD), head circumference (HC), femur length (FL), and abdominal circumference (AC) are used in combinations in these formulae. Among these parameters, AC is quite commonly used for estimation of fetal weight though it is quite variable. However, there is an underestimation of fetal weight as these parameters do not account for soft tissue mass. And also, at extremes of the weight spectrum, these formulae are found to be less accurate.[1] Materials and MethodsThis was a prospective observational study conducted in the Department of Radio Diagnosis of a medical college hospital of coastal Karnataka. Ladies with a singleton pregnancy who gave written informed consent were selected as study participants. A sample size of 70 was derived using the formula 4pq/d2. The prevalence (p) was taken from a previous similar study conducted by Banerjee et al.[5] and was found to be 83%, q was 100-p and was 17% and d was absolute precision of 10%. With non-response rate of 20%, the sample size was calculated to be 68, which was approximated to 70. The study was conducted for a duration of 2 months, from November 29, 2018, to January 25, 2019. Consecutive sampling was done. Ladies with a singleton pregnancy of gestational age 37–39 weeks and delivered in the same institution within 7 days of ultrasound assessment and who gave written informed consent were included in the study. Only those ladies who had similar gestational age by USG and last menstrual period (LMP) were included in the study. Ladies with maternal diabetes were also included in the study. Ladies with oligohydramnios (amniotic fluid index < 7), multifetal gestation, who delivered after 7 days of the assessment and babies born with congenital anomalies, were excluded from the study. ResultsThe mean age of the participants was 25.41 (±4.03) years. Among the 70 participants, 41 (58.5%) had completed 38 weeks of gestation and the rest had 37 completed weeks. Table 1 depicts the descriptive statistics of the various variables assessed using USG. These variables were further used to calculate the EFW using formulae. The birth weights were further categorized as normal and macrosomia. Among the newborns, who had completed the 37 gestational weeks, 12 (17.14%) were macrosomic. Among newborns with 38 completed weeks, 8 (11.43%) were macrosomic. The correlations between the estimated birth weights using MTSTT and Hadlock’s formula with actual birth weights were assessed using Pearson’s correlation. The correlation between FASTT value and actual birth weight was also assessed. Fetal weight estimated using MTSTT and actual birth weight showed a moderate positive correlation (Pearson value 0.473). Fetal weight estimated using Hadlock’s formula, and actual birth weight was also found to be moderately correlating (Pearson value 0.380). Both these correlations were found to be statistically significant (P < 0.05). The correlation between FASTT value and actual birth weight was not statistically significant (Pearson value: 0.152 and P: 0.165). DiscussionThe fetal ultrasound parameters were assessed in this study, along with the estimation of fetal weight. The correlations between the EFW using MTSTT and actual birth weight were tested, and moderate correlation was observed. This observed correlation was statistically significant. [Table2] The scatter plot with these variables in Y- and X-axes, respectively, also showed clustering of the values [Figure 1]. Similar findings were obtained by the study conducted by Abuelghar et al. where, a highly significant correlation was obtained between EFW using MTSTT and birth weight (Pearson value 0.609, P < 0.001).[6] Kalantari et al. also found a similar correlation between these values, which was highly significant (Pearson value 0.50, P < 0.001).[9]
|
ConclusionIn this study, we estimated the fetal weight of term, singleton pregnancies using MTSTT and Hadlock’s method. The FASTT was measured as well. These obtained values were correlated with the actual birth weight was observed. A moderate correlation was found between the EFW using MTSTT and Hadlock’s method. Fetal weight estimation using MTSTT was more sensitive and specific compared to that of Hadlock’s method. We thus conclude that the estimation of fetal weight using MTSTT is more superior to that of Hadlock’s method. |
Subscribe now for latest articles and news.