Journal of Medical Sciences and Health
DOI: 10.46347/jmsh.v8i3.22.350
Year: 2022, Volume: 8, Issue: 3, Pages: 288-291
Case Report
Shwetha Basavaraj1 , P B Saniha1 , U Geethalakshmi1 , Ramesh Babu1 , R P Vinayaka1
1Shimoga Institute of Medical Sciences, Shimoga, Karnataka, India
Address for correspondence:
P B Saniha, Shimoga Institute of Medical Sciences, Shimoga, Karnataka, India.
E-mail: [email protected]
Received Date:23 July 2022, Accepted Date:28 September 2022, Published Date:19 December 2022
Colorectal cancers (CRC) are on the rise globally with increased incidence rate 5.7/100000 cases in developing countries like India. 1 Majority (90%) of CRC are adenocarcinoma. The primary adenosquamous carcinoma (ASC) of the colon is exceedingly rare variant of adenocarcinoma with incidence of 0.025% and accounts for 0.1% of colonic epithelial malignancies. 2 The squamous differentiation accounts for its aggressiveness and poor prognosis. Here we report a rare case of primary ASC in 80year old male who presented with large bowel obstruction and peritonitis. A 80-year-old male brought to causality with history of fever, vomiting, pain in abdomen, altered sensorium since three days. The clinical examination revealed intestinal obstruction and peritonitis. Patient was immediately subjected for radiological and hematology investigations which showed signs of bowel obstruction and perforation. On emergency exploratory laparotomy, colonic perforation was identified along with an ulcer proliferative mass in ascending colon. Gross examination of right hemicolectomy revealed 9x6x3cm ulcero proliferative mass in ascending colon. The microscopic examination showed an infiltrating tumor composed of adenocarcinoma component and areas of squamous differentiation (60%) noted. Tumor was invading through muscularis propria and serosa. Final diagnosis of primary ASC was made. Colonic ASC is rare and associated with poorer prognosis. The squamous cell differentiation has greater metastatic potential than adenocarcinoma. Compared to adenocarcinoma, ASC is more likely to manifest with advanced disease and complications.
Keywords: Adenosquamous, Carcinoma, Colon
Colorectal cancers (CRC) are on the rise globally with increased incidence rate of 5.7/100000 cases in developing countries like India. It is second most common cancer in women and third most common cancer in males. 1 Majority (90%) of CRC are adenocarcinoma. However, primary adenosquamous carcinoma (ASC) of the colon is exceedingly rare variant of adenocarcinoma with incidence of 0.025% and accounts for 0.1% of colonic epithelial malignancies. 2 With presence of glandular and squamous differentiation this carcinoma is known for its aggressiveness and poor prognosis.
53% of colorectal adenocarcinoma were located in the sigmoid colon, rectum, and anus, but ASC is usually located in the right colon. 3
The symptomatic manifestations of ASC are similar to colon adenocarcinomas except that there are late presentations with complications. Clinical features include: abdominal pain, abdominal mass, weight loss, change in bowel habits, hematochezia, symptoms of obstruction, perforation and peritonitis. 4 It has been demonstrated that patients with ASC may present with paraneoplastic syndromes such as hypercalcemia.3 In association has been noted between squamous metaplasia in colorectal carcinoma and ulcerative colitis. 2
Here we report rare case of primary ASC in 80-year-old male who presented with large intestine obstruction, perforation, and peritonitis which was treated by surgical management.
An 80-year-old male brought to the emergency room with history of fever, vomiting, pain abdomen for three days and altered sensorium since one day. He also had altered bowel habits since a month. His family history, past history and personal history was not contributory.
On physical examination, his GCS score of 14, without signs of meningeal irritation. The Vital signs–Temperature: 101.6F, BP: 60/40, PR: 144bpm, RR: 24cpm. On systemic examination, per abdominal examination revealed rebound tenderness and abdominal distension. Bowel sounds were sluggish to absent. With clinical diagnosis of intestinal obstruction with suspicion of peritonitis patient was immediately subjected for various haematological, biochemical and radiological investigations.
Laboratory test results showed significant neutrophillic leucocytosis with evidence of sepsis. Plain radiography (X-ray) of the abdomen showed signs of bowel obstruction and perforation (Figure 1). On emergency exploratory laparotomy colonic perforation was identified along with a fungating mass in ascending colon near hepatic flexure. A right hemicolectomy was done with ileotransverse colon anastomosis. The hemicolectomy specimen was sent in formalin for histopathological examination. Patient expired a day after surgery due to respiratory failure and septic shock.

Right hemicolectomy specimen measuring 39cm in length was received in histopathology department which was grossly examined, cut opened along the antimesentric border and further fixed in 10% Neutral Buffered Formalin(NBF). There was a solid, grey, ulceroproliferative growth measuring 7× 6×3cm seen in the ascending colon near hepatic flexure. Tumour showed foci of necrosis and haemorrhage and was invading the wall. No lymph node was identified grossly (Figure 2).

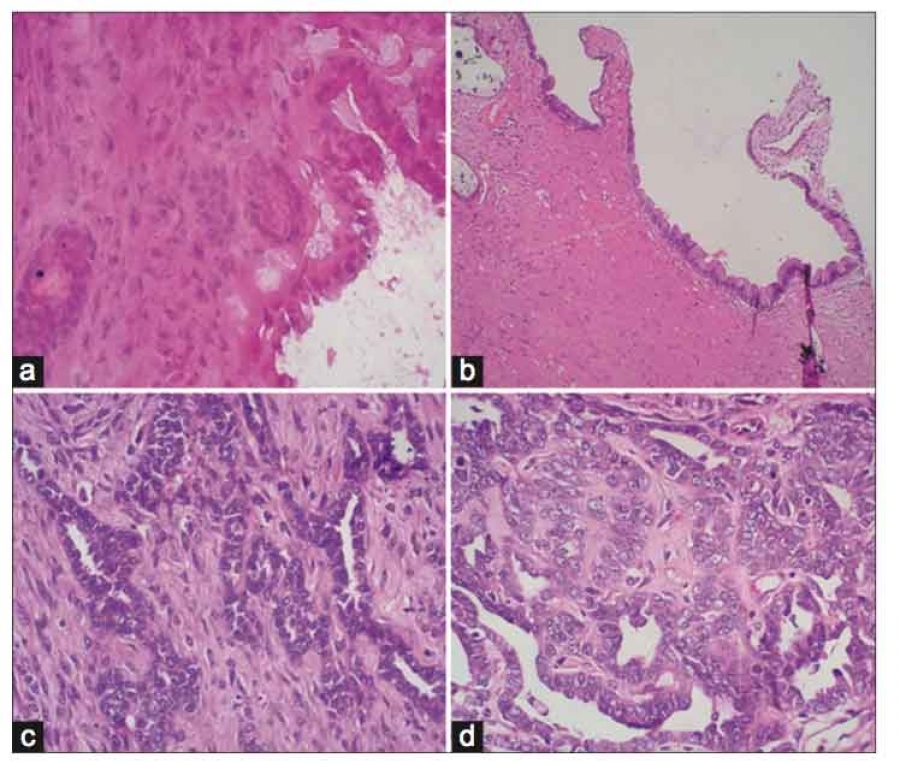
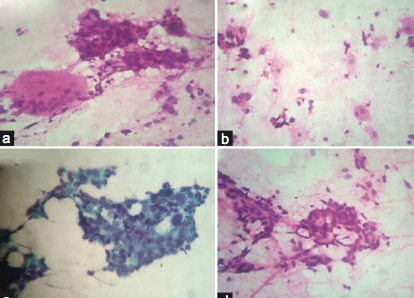
Microscopic examination showed an infiltrating tumour composed of pleomorphic cells arranged in glands, clusters, nests and sheets (Figure 3 & Figure 4a, b). Areas of squamous differentiation (60%) noted. The tumour cells were having high N:C ratio, hyperchromatic oval to round nuclei, 1-2 prominent nucleoli and abundant eosinophilic cytoplasm. Bizzare cells, tumour gaint cells, atypical mitosis 1-2/10HPF noted. Areas of extensive necrosis and haemorrhage seen. Tumor was invading through the muscularis propria and serosa. Lymphovascular invasion present. No evidence of signet cells or mucin. Final diagnosis of primary ASC was made with pathological staging-T3 N0 M0. 5


The first case of colorectal ASC was reported by Herxheimer 6 in 1907 and was described as a tumour containing both an adenocarcinoma and a squamous cell carcinoma component. Generally, the epithelium near the dentate line is anatomically capable of differentiating into both glandular and squamous epithelium, but the pathogenesis of squamous cell carcinoma components of the colon remains unclear. 7, 8 Several hypotheses have been advanced for its histogenesis in the gastrointestinal tract. Four hypotheses have been suggested:
Ectopic squamous cells in the colonic mucosa may be directly transformed into squamous malignant cells.
Undifferentiated or reserve cells in the colonic epithelium may be transformed directly into squamous cell carcinoma.
Normal glandular cells may be transformed into a malignant squamous neoplasm.
Adenocarcinomas in situ can directly be transformed into malignant squamous cells. 9
Kang et al 9 and Beversdrof et al 10 reported cases of ASC in 6th decade. The ASC cases in 5th decade was described by Sunkara et al 4 and Toumi 11 et al. In our study, an 80 y old case was presented. Kang et al 9 and Sunkara et al 4 described ASC in males whereas Beversdrof W 10 et al and Toumi et al 11 in females. Our study was inconcordance with Kang 9 and Sunkara et al.4
The most common clinical presentation were abdominal pain and distension, as described by Kang et al, 9 Sunkara Tet al 4 Beverdrof et al, 10 Toumi et al, 11 which was also similar to our case.
Right colon was the most common site of tumour according to Sunkara et al, 4 Beverdrof et al, 10 Toumi et al, 11 which was corresponding to our study. But Kang et al 9 reported in Left colon (Table 1).
Kang et al 9 and Toumi et al, 11 has given pathological staging as stage III which is similar to our study. 5
As squamous cell component has greater metastatic potential than the glandular cell Component, they have poorer prognosis than adenocarcinoma, 1, 3 that is 5-year survival rates of ASC and AC are approximately 30% and 50–60%, respectively. The most common metastatic sites of colonic ASC are liver, peritoneum and lung, respectively.3 Overall rate of regional metastases and distant metastases were reported to be 46.0% and 42.4%, respectively. 9, 11 Thus, early detection and prompt treatment of ASC is important.
Frizelle et al.12 reported a 5-year survival rate of 86% for patients with Stage II disease and only 24% for patients with Stage III disease.
Surgical resection along with regional LN dissection is considered to be the definitive treatment for colorectal Ad-SCC, and the exact role of adjuvant chemotherapy remains unclear because of its rarity.9 Hence Post resection follow up is necessary.
Colonic ASC is a rare variant of adenocarcinoma. It usually presents with advanced disease, complications and associated with poor prognosis. Colonic ASC should be considered in the differential diagnosis in elderly patients presenting with features of intestinal obstruction or perforation. Histpathological examination is crucial for establishing the diagnosis and further management of patients.
Subscribe now for latest articles and news.